
Article Figures & Data
Figures
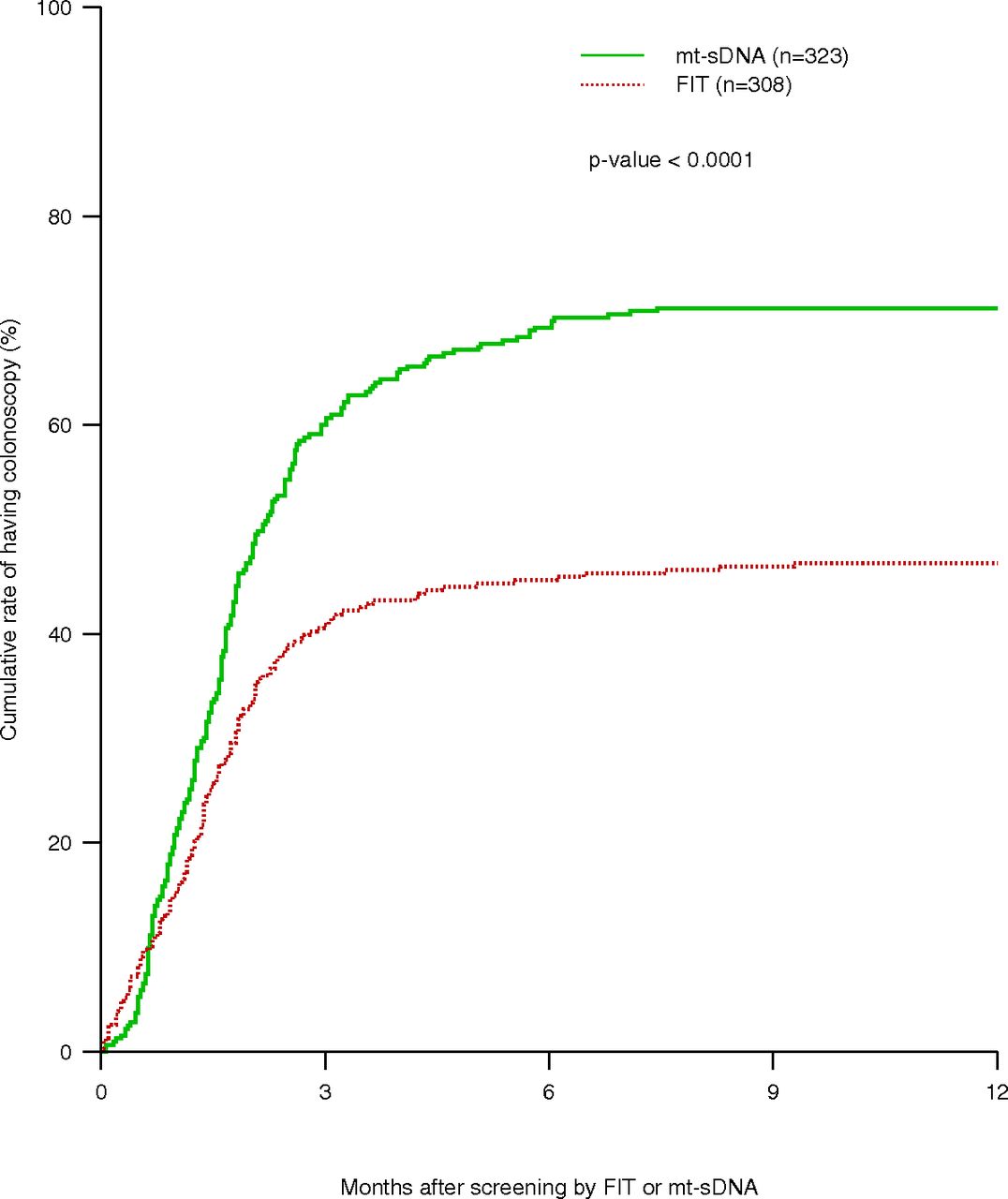
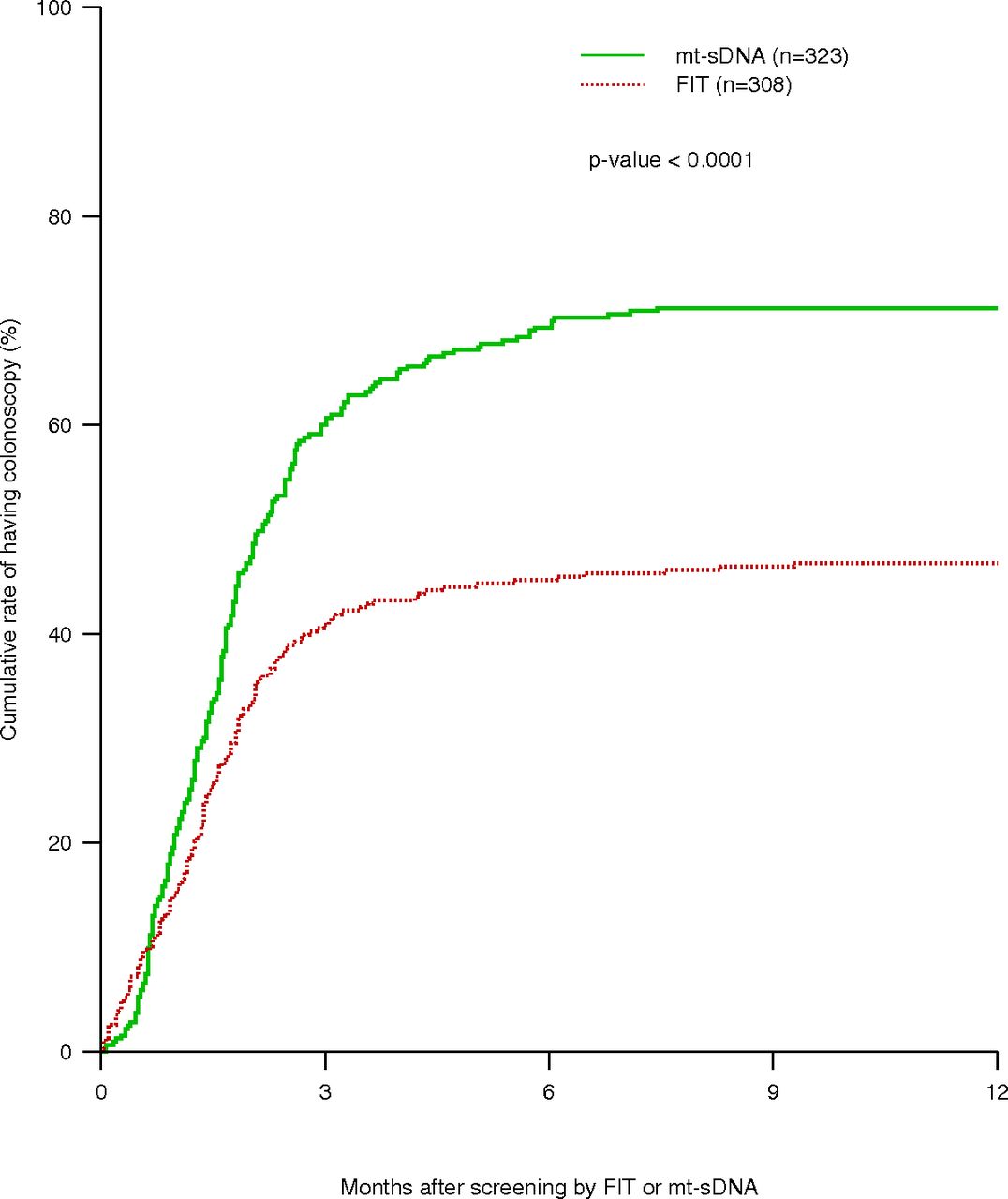
- Figure 1.
Kaplan-Meier estimation of time-to-colonoscopy of patients who had FIT test and who had mt-sDNA. The median time-to-colonoscopy for patients FIT was N/A (50% rate was not reached for this group). The median (95% CI) time-to-colonoscopy for patients who had mt-sDNA was 2.16 (95% CI, 1.80-2.52) months. Abbreviation: FIT, fecal immunochemical testing.
Tables
Characteristic FIT Mt-sDNA Measures stool hemoglobin Yes Yes Measures genomic markers No Yes Approved as screening test Yes Yes Labeling restricted to average risk patients No Yes Recommended interval 1 year 3 years Kit distribution In-person or mail from local lab Mail from external site Kit return In person or mail to local lab Mail to external site Reminder calls to return No Yes Medicare out-of-pocket cost $0 $0 Medicare reimbursement $22 $483 FIT, fecal immunochemical testing.
Variables All Patients (n = 631), Mean (STD)/Frequency (%) Mt-sDNA (n = 323) FIT (n = 308) P Value* Age (years) 69.19 (10.57) 69.55 (7.95) 68.82 (12.76) .39 Sex Female 349 (55.3) 205 (63.47) 144 (46.75) <.0001 Male 282 (44.7) 118 (41.84) 164 (53.25) Hispanic No 573 (99.13)) 285 (99.30) 288 (98.97) .66 Yes 5 (0.87) 2 (0.70) 3 (1.03) Race Asian 3 (0.49) 0 (0.00) 3 (0.99) Black 48 (7.77) 17 (5.41) 31 (10.20) Other 1 (0.16) 0 (0.00) 1 (0.33) .064 White 563 (91.10) 296 (94.27) 267 (87.83) Hispanic 2 (0.32) 1 (0.32) 1 (0.33) Native 1 (0.16) 0 (0.00) 1 (0.33) Insurance Commercial 301 (47.7) 151 (46.7) 150 (48.7) Medicaid 11 (1.7) 5 (1.6) 6 (1.9) Medicare 290 (46) 158 (48.9) 132 (42.9) .18 Self-pay 9 (1.4) 3 (0.9) 6 (1.9) Unknown 20 (3.2) 6 (1.9) 14 (4.6) Specialty Family Medicine 368 (58.3) 143 (44.3) 225 (73) Internal Medicine 242 (38.3) 163 (50.5) 79 (25.7) GI 20 (3.2) 16 (4.9) 4 (1.3) <.0001 Gynecology 1 (0.2) 1 (0.3) 0 (0) Provider Gender Female 317 (50.2) 175 (54.2) 142 (26.1) .43 Male 314 (49.8) 148 (45.8) 166 (53.9) Mid-Level Provider Yes 37 (5.9) 22 (6.8) 15 (4.9) .3 No (physician) 594 (94.1) 301 (93.2) 293 (95.1) ↵*P value was based on the comparison between two cohorts (FIT, mt-sDNA) of patients.
GI, gastroenterology; FIT, fecal immunochemical testin; STD, standard deviation.
FIT (n = 164) Frequency (%) Mt-sDNA (n = 92) Frequency (%) System GI clinic referral 48 (29.3) 11 (12.0) Colonoscopy not scheduled 5 (3.0) 17 (18.5) Total 53 (32.3) 28 (30.4) Provider level Attributed to false positive 3 (1.8) 0 (0.0) Failure to inform patient 0 (0.0) 7 (7.6) Attributed to other reasons 39 (23.8) 1 (1.1) Recent colonoscopy done 24 (14.6) 1 (1.1) Other health issue to prioritize 8 (4.9) 11 (12.0) Unknown 21 (12.8) 20 (21.7) Total 95 (57.9) 40 (43.5) Patient level Patient refused (before ordered) 8 (4.9) 8 (8.7) Patient refused (after ordered) 4 (2.5) 15 (16.3) No show/cancellation 42 (25.6) 26 (28.3) Did not complete bowel prep 0 (0) 1 (1.1) Other reason 6 (3.7) 3 (3.3) Total 60 (36.6) 53 (57.6) ↵*Determined by medical record review.
FIT, fecal immunochemical testing; GI, gastroenterology.
Variables Univariate Cox Regression Multivariable Cox Regression HR 95% CI of HR P value HR 95% CI of HR P Value Age (per year increase) 0.99 0.98, 1.00 .13 0.99 0.98, 1.00 .181 Sex (female vs male) 1.17 0.95, 1.43 .14 1.09 0.83, 1.32 .717 Race (Black vs White) 1.30 0.91, 1.85 .16 1.38 0.95, 2.00 .089 Insurance (commercial vs Medicare) 1.12 0.91, 1.38 .29 1.10 0.87, 1.39 .411 Screening test method (mt-sDNA vs FIT) 1.83 1.48, 2.25 < .0001 1.75 1.40, 2.19 < .0001 Specialty (FM vs IM) 0.87 0.71, 1.08 .202 Provider gender (female vs male) 1.30 1.06, 1.60 .01 1.19 0.95, 1.50 .125 Mid-level provider (yes vs no) 1.16 0.77, 1.75 .483 FIT, fecal immunochemical testing; FM, family medicine; HR, hazard ratio; IM, internal medicine; CI, confidence interval.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Joint Asian Pacific Association of Gastroenterology (APAGE)-Asian Pacific Society of Digestive Endoscopy (APSDE) clinical practice guidelines on the use of non-invasive biomarkers for diagnosis of colorectal neoplasia
- Joint Asian Pacific Association of Gastroenterology (APAGE)-Asian Pacific Society of Digestive Endoscopy (APSDE) clinical practice guidelines on the use of non-invasive biomarkers for diagnosis of colorectal neoplasia
- Impact of Patient Adherence to Stool-Based Colorectal Cancer Screening and Colonoscopy Following a Positive Test on Clinical Outcomes
- Advancing Research Methods for Common Problems in Family Medicine and Family Medicine Practice Management