
Abstract
The family physician’s role in recognizing and managing sudden sensorineural hearing loss (SSNHL) is crucial. A recently updated otolaryngologic clinical practice guideline has been released for this emergency syndrome, but dissemination is limited to a specialty journal. As a result, the guidelines may not be widely available in the primary care setting where patients often present. We provide this focused review to clarify and disseminate SSNHL guidelines for the frontline family physician.
- Audiology
- Clinical Decision-Making
- Conductive Hearing Loss
- Family Medicine
- Family Physicians
- Otolaryngology
- Primary Health Care
- Sudden Hearing Loss
Introduction
Sudden sensorineural hearing loss (SSNHL) is a medical emergency in which patients experience a sudden (within 72 hours) drop in hearing that is sensorineural in nature, not the result of mechanical blockage from fluid or wax buildup. Prompt recognition is critical as there is a window of time in which medical interventions may be successful in restoring hearing and/or reducing tinnitus, thus providing significant improvement in patient quality of life.1 Although SSNHL can result from a variety of identifiable causes (neoplastic, infectious, autoimmune, neurologic, ototoxicity), 90% of cases are idiopathic.2⇓–4 SSNHL affects 5 to 27 per 100,000 people annually, with about 66,000 new cases per year in the United States.4⇓⇓–7 The incidence, debilitating consequences of missed diagnosis and management, and the scarcity of randomized controlled trials led the American Academy of Otolaryngology–Head and Neck Surgery to develop a clinical practice guideline (CPG) that was recently updated in 2019 to assist providers in appropriately managing this condition.7,8
The CPG for SSNHL is intended for all clinicians who diagnose or manage patients aged 18 years and older that present with sudden hearing loss. The CPG is focused specifically on idiopathic SSNHL—hearing loss that is rapid in onset, not due to conductive pathology, and not explained by an identifiable cause. Despite intense efforts to disseminate CPGs, previous studies have shown that uptake of recommendations in CPGs is limited and adherence to certain key action statements is low.9⇓–11 The need to disseminate the guidelines beyond the otolaryngology community is crucial, as the majority of patients with SSNHL are first evaluated by nonotolaryngologists, with 15,000 to 66,000 patients visiting family medicine clinics, urgent care centers, and emergency rooms for assessment of this complaint annually.7 To our knowledge, this is the first report specifically aimed at disseminating the guidelines for SSNHL into the family medicine literature, with a goal of achieving broader adherence to the CPG.
The family physician’s role in recognizing and managing SSNHL is pivotal. In their role at the frontline, family physicians can provide the highest quality assessment, management, and patient centered care. Timely recognition of SSNHL by the initial evaluating physician affects the availability of treatment options, as well as the success rates of treatment. Improved awareness, clarity, and dissemination of CPGs is critical to improve adherence and the quality of clinical care.7,10 We describe a case report of a typical patient presenting with SSNHL, followed by a summary of the current CPG to equip the frontline family physicians with tools for managing sudden hearing loss.
Case Report
A 64-year-old man with hypertension presents to his family medicine physician complaining of blocked hearing in his left ear for 1 day. He noticed a loud ringing sound and the feeling of the left ear being plugged. He has not had any dizziness, pain in his ear, or drainage from his ear. He denies any recent trauma, noise exposures, respiratory illness, change in medications, or other neurologic symptoms.
On physical examination, the left external ear and ear canal are unremarkable. The left tympanic membrane is normal in appearance and no definite middle ear effusion can be seen. A vibrating 512-Hz tuning fork placed on the midline of the forehead is perceived louder in the right ear. Cranial nerve examination is otherwise intact, and there are no other abnormalities noted on a complete head and neck examination nor focal neurological examination.
The family physician is concerned that the patient may be experiencing SSNHL and discusses the diagnosis, natural history, treatment options, and current evidence regarding this condition. The patient and physician jointly decide to try a course of oral steroids as initial therapy, and the patient is prescribed 60 mg prednisone daily for 10 days, followed by a 7-day taper. The family physician also orders magnetic resonance imaging (MRI) brain/internal auditory canal protocol with gadolinium and places an urgent referral to an otolaryngologist for a hearing test and further evaluation.
The otolaryngology office schedules the patient for an urgent audiogram and evaluation by an otolaryngologist the following day. The audiogram demonstrates a significant drop in sensorineural hearing levels throughout the frequency spectrum. After discussion, the patient elects to complete his oral steroid therapy before any further intervention is taken. He has a partial response to therapy 2 weeks after onset of symptoms, and he elects to undergo an intratympanic (IT) injection at this time. At followup 1 week later, his hearing has returned to his baseline level.
CPGs for SSNHL
The guidelines discussed below were adapted from S. Chandrasekhar, B. Tsai Do, S. Schwartz et al, Clinical Practice Guideline: Sudden Hearing Loss (Update), Otolaryngology–Head and Neck Surgery. vol. 161, no. 2, pp. 195 to 210. Copyright © 2020 by Andrew Prince. Reprinted by permission of SAGE Publications, Inc.
Discussion
Based on the CPG for SSNHL, the following approach is recommended, described in stepwise fashion from the moment of patient presentation. Figure 1 depicts the management schema.
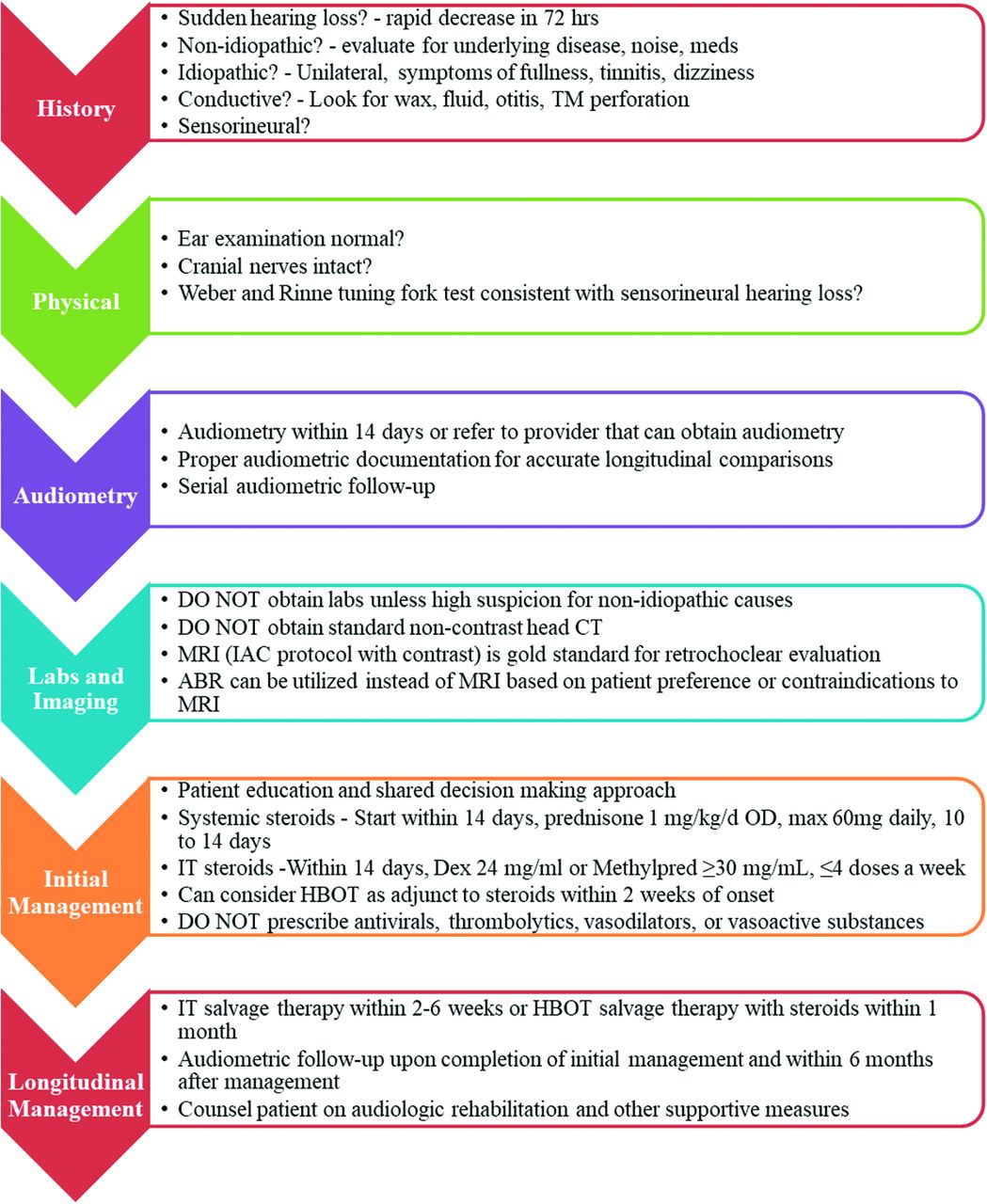
Sudden sensory hearing loss management schematic. Abbreviations: TM, tympanic membrane; CT, computed tomography; MRI, magnetic resonance imaging; ABR, auditory brainstem response; OD, once daily; Dex, dexamethasone; Methylpred, methylprednisolone; HBOT, hyperbaric oxygen therapy; IT, intratympanic.
History and Physical
When a patient presents with sudden hearing loss, the CPG recommends (Grade C) a detailed history to look for clinical features in patients with idiopathic SSNHL that may be associated with an underlying disease such as vestibular schwannomas, stroke, noise, and ototoxic medications (Table 1).12⇓⇓–15 Typical clinical features of SSNHL include the rapid development of unilateral hearing loss, a normal ear examination, and associated clinical symptoms of a stuffy or full ear, tinnitus, and dizziness.2,3 Patients may notice difficulty hearing on awakening, when hearing had been normal or at baseline the evening prior. Ipsilateral tinnitus is very common, and dizziness is present in 30% to 60% of cases of SSNHL. If persistent and bothersome both may portend a poorer prognosis, and significant economic and psychological burden.16⇓–18
Nonidiopathic Causes of Sudden Sensorineural Hearing Loss
There is a strong recommendation (Grade B) to distinguish between SSNHL and sudden conductive or mixed hearing loss, as this will define potential treatments and prognosis.7 Delay in treatment of SSNHL often results when a clinician assumes that a patient has conductive hearing loss (CHL) without considering a diagnosis of SSNHL.2 Collecting a good history as discussed above can help accurately distinguish patients with SSNHL; however, some of the associated symptoms including tinnitus, ear fullness, and vertigo may also be present in CHL.2,19,20 Patients with SSNHL often present with a chief complaint of a “blocked ear,” which may bias the examiner toward a perception of fluid in the middle ear. A focused head and neck physical examination with tuning fork examination is required to differentiate CHL from SSNHL.
Examination should include inspection of the ear canals, visualization of the tympanic membrane, and cranial nerve testing. Most causes of CHL can be diagnosed by otoscopy including cerumen impaction, foreign body impaction, middle ear fluid, otitis externa, tympanic membrane abnormalities, trauma, and cholesteatoma. Unlike CHL, patients with SSNHL will almost always have a normal otoscopic examination.7 The authors acknowledge, however, that definitive otoscopic diagnosis of a middle-ear effusion may be challenging in some situations and encourage the addition of a tuning fork test to distinguish between CHL and SNHL when audiometric data are not readily available. In general, the tuning fork evaluations provide a reliable method to acutely assess the type of hearing loss and are supported by the CPG.7,8 Figure 2 demonstrates proper tuning fork technique and result interpretation. Ahmed et al,21 proposed the hum test as an alternative to the Weber tuning fork test with similar sensitivity and specificity. This test can be used without a tuning fork by asking the patient to hum; if he or she hears one’s own hum louder in the affected ear, there is likely CHL in that ear. A complete history and targeted physical examination with tuning fork testing are essential but do not supplant formal audiometric testing.
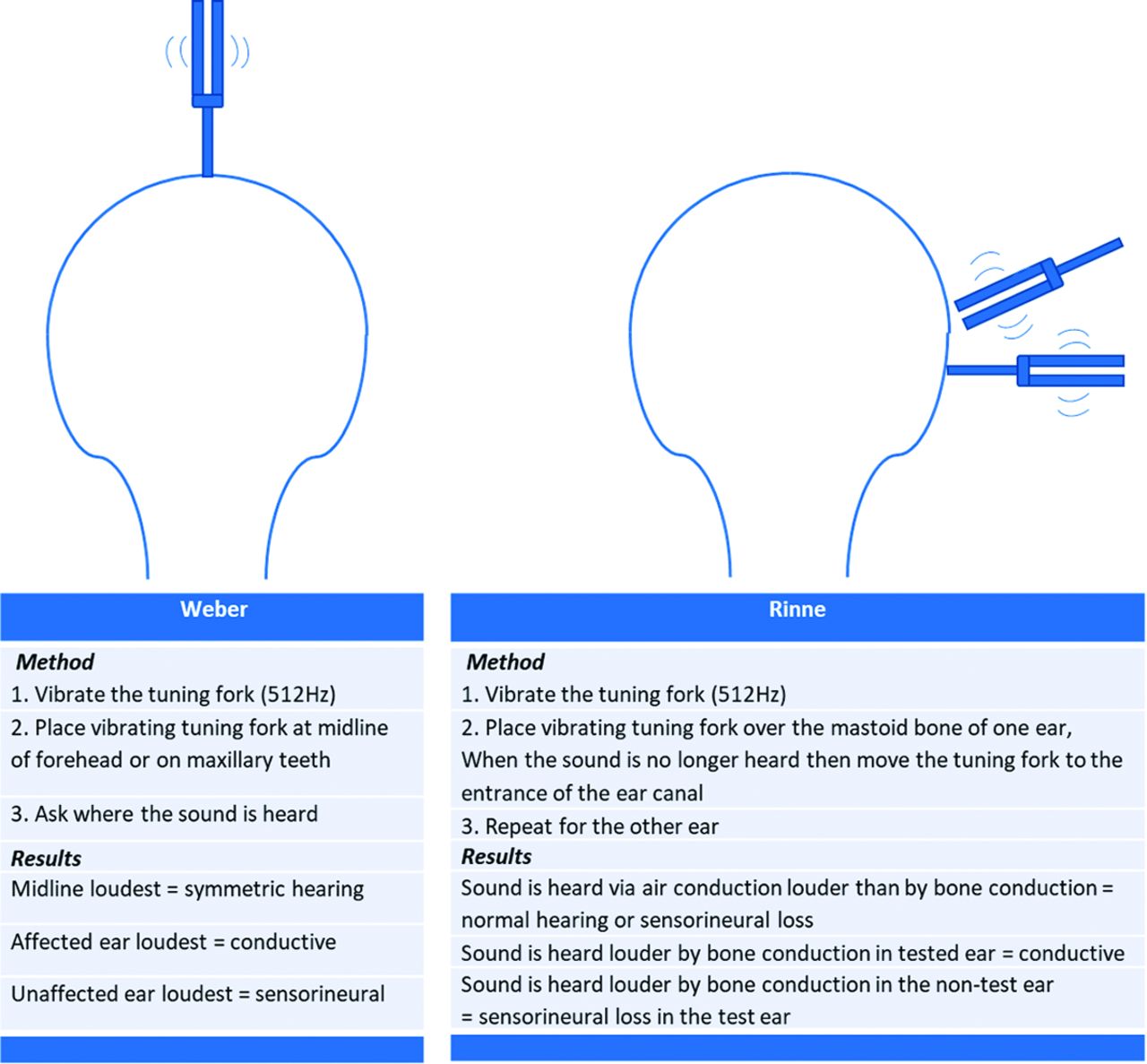
Recommended technique and result interpretation for Weber and Rinne testing.
Labs, Imaging, and Audiometry
Though most SSNHL is idiopathic, there are several other possible etiologies to consider. CPG guidelines strongly recommend against (Grade B) routine, “shotgun,” laboratory workup as the evidence supporting their use is limited to observational and case-control studies.7 Within the literature most studies are underpowered and none support that a laboratory test improves management or outcomes.8,22⇓–24 Furthermore, labs have associated cost and potential harms related to false-positive or false-negative results. Laboratory studies should be limited to specific tests cued by pertinent findings in the history or physical examination.
It is recommended (Grade C) that an audiometric evaluation is obtained for SSNHL, or a referral made to a physician that can obtain one, within 14 days of presentation and for serial evaluations.7 Audiometry is the most reliable evaluation for differentiating CHL from sensorineural hearing loss and establishes frequency-specific hearing and word recognition ability. There may be concern regarding the logistic ability for a patient to undergo an audiometric evaluation within the specified time frame. To address this, most, otolaryngology practices have a specific workflow to triage referrals for sudden hearing loss and assure that these patients are seen promptly.
Imaging is an important adjunct to SSNHL workup and choosing the most effective modality is key. Routine computed tomography of the head is strongly recommended against (Grade B) in the initial assessment of patients with presumptive idiopathic SSNHL without focal neurologic findings.7 A routine head computed tomography scan is a very low-yield study for examination of the inner ear, and yet is often ordered.11 It is recommended (Grade B) to obtain an MRI to evaluate for alternate pathologies involving the pathway from the cochlea through the brainstem commonly referred to as “retrocochlear pathology.”7 Vestibular schwannomas are the most frequent mass lesion discovered in cases of SSNHL, with an incidence of 2.5%.15 An MRI is the standard and we advise the sensitive and widely available internal auditory canal protocol MRI with gadolinium enhancement.5,8,25,26 Auditory brainstem response (Grade C) may be offered for patients with SSNHL who do not wish to have an MRI. However, a normal auditory brainstem response is less sensitive than MRI and may miss small tumors.8,27⇓–29
Management
A shared decision-making approach to management and developing a plan of care for patients with SSNHL is important. There are a myriad of inconclusive or modestly beneficial treatment options ranging from observation to combination modality steroid therapy. The CPG strongly recommends (Grade B) educating patients about the favorable natural history, benefits, and risks of interventions, and the limitations of existing evidence.7 Despite the intuitiveness of this recommendation, it is one of the most frequently skipped by otolaryngologists and nonotolaryngologists alike.11 We encourage practitioners to reference the CPG, which provides a useful patient education handout titled, “Frequently Asked Questions/Patient Education.”7
A widely used treatment of idiopathic SSNHL is administration of corticosteroids, either oral or IT. The CPG provides the option (Grade C) to use corticosteroids as initial therapy to patients with SSNHL within 2 weeks of symptom onset.7 Historically, systemic steroids have been utilized by clinicians because steroid administration is one of the few treatment options that has shown efficacy, despite mostly equivocal data.5,7,8,30,31 Systemic steroid therapy may be contraindicated in cases of insulin-dependent or poorly controlled diabetes, tuberculosis, or peptic ulcer disease. Treatment with corticosteroids seems to offer the greatest recovery when initiated in the first 2 weeks following SSNHL, with little benefit after 4 to 6 weeks; this is similar to the timeline of spontaneous improvement in hearing, making it difficult to conclude corticosteroids offer greater benefit than observation alone.2,5,6 IT steroid administration was first described for SSNHL in 1996.28 IT steroid use is increasing in popularity due to a reduction in systemic side effects.29 IT injections may be offered either as primary therapy for SSNHL, in combination with systemic steroids as primary therapy, or as salvage therapy after a patient has failed an initial course of systemic steroids.7 The 2019 CPG does not make a specific recommendation on route of administration (systemic, IT, or combination therapy) for primary treatment.7 This differs from salvage therapy, which will be discussed separately.
If an IT steroid injection is selected, this procedure is performed in the clinic setting by an otologist or general otolaryngologist comfortable with the procedure. It can be performed at the initial visit to an otolaryngologist’s office, without the need for special scheduling. This procedure is performed under otomicroscopic guidance and entails direct topical anesthesia of the tympanic membrane (no systemic sedation or anesthesia is administered), followed by a controlled puncture of the tympanic membrane to instill a liquid steroid formulation to the middle ear space. IT injections provide a high concentration of steroid to the inner ear by diffusion through the round window membrane, while minimizing systemic absorption.30,31 Multiple trials, reviews, and meta-analyses have yet to show any significant difference in therapeutic outcomes between systemic therapy, IT, and combination therapy (with the exception of the Battaglia study,32 which suggested that initial therapy with IT steroids, either alone or in combination with oral steroids, conferred benefit over systemic steroids alone).32⇓⇓⇓⇓⇓⇓⇓–40 Ultimately, when you consider the devastating effects of SSNHL to patients, even a small possibility of hearing improvement makes corticosteroids a reasonable treatment to offer patients.
If systemic steroids are chosen for initial treatment, they should be given within 14 days. The recommended dose of oral prednisone is 1 mg/kg/day in a single (not divided) dose, with the usual maximum dose of 60 mg daily prescribed for 7 to 14 days, then tapered over a similar period of time.8,32,40 The equivalent dose of prednisone (60 mg) is 48 mg for methylprednisolone and 10 mg for dexamethasone.7 Early treatment is of the utmost importance, and adequate initial dosing is important, with avoidance of the methylprednisolone and prednisone dose packs, which do not provide adequate steroid dose for this indication.7 Serious side effects should be closely monitored including blurred vision, glaucoma, weight gain, muscle weakness, osteoporosis, susceptibility to infections, worsening of diabetes, and hypertension. The CPG does not specify which provider should initiate steroid therapy. If the history and physical examination strongly suggest SSNHL, and there are no contraindications present, it is most prudent for the initial provider to begin the treatment regimen, given the time-sensitive nature of response-to-therapy.
Among the other initial treatment options available, the CPG strongly recommends against (Grade B) routine prescription of antivirals, thrombolytics, vasodilators, or vasoactive substances to patients with SSNHL.7 Studies examining antiviral, vasoactive, vasodilatory, and rheologic agents have been inconclusive, revealed no significant benefit, or pose significant side effects.8, 41,42 Less frequently implemented in the United States is the option (Grade B) to refer to a clinician who can provide hyperbaric oxygen therapy (HBOT) combined with steroid therapy within 2 weeks of onset, or as salvage therapy within 1 month of the onset of SSNHL.7 The therapy is not currently approved by the U.S. Food and Drug Administration, but there have been multiple trials and reviews that demonstrated potential benefit.7,43,44
When initial therapy fails, guidelines recommend (Grade B) IT steroid therapy for incomplete recovery from SSNHL 2 to 6 weeks after the onset of symptoms.7 Salvage therapy refers to failure of systemic or topical steroids, HBOT, or observation. Data suggests that IT steroids are an effective modality for salvage therapy. Conflicting and weak data exists for the use of systemic steroids and HBOT alone, or as combination with IT for salvage therapy.34,35,45,46
Patient reported hearing recovery is not an accurate measure of response to treatment. Audiometric evaluation is recommended (Grade C) for all patients with SSNHL at the conclusion of treatment and within 6 months of treatment completion.7 Longitudinal followup is important as some patients (close to one third) will have an underlying cause that is eventually identified but was not evident at initial presentation.47 In addition, the patient with partial or no hearing recovery and/or persistent tinnitus will require ongoing management from otolaryngologic, audiological, and psychological perspectives.48 If there is residual or permanent hearing loss and/or tinnitus, it is strongly recommended (Grade B) that clinicians counsel patients about the possible benefits of audiologic rehabilitation and other supportive measures.7 There are a variety of further management options for SSNHL sequela that start with appropriate patient centered counseling and decision making. Besides counseling, some patients require therapeutic interventions such as speech reading, and auditory training.7 Further data-supported measures include hearing aids, hearing-assist devices, and cochlear implantation, which may rehabilitate hearing and quality of life.7,8,49,50
Conclusion
The family physician is often the initial provider to interface with patients who present with SSNHL. The family medicine provider plays a crucial role in the early recognition and initial management of SSNHL. A thorough history and physical examination are the cornerstones of evaluation to differentiate between sudden CHL and SNHL, and to assess for important neurologic diagnosis such as stroke. Prompt initiation of steroid therapy is recommended for patients with SSNHL, along with MRI imaging, audiology evaluation, and consultation with an otolaryngologist. We encourage the family physician to feel empowered to begin initial therapy with oral corticosteroids if their suspicion for SSNHL is high, even while awaiting formal audiometric confirmation or referral to a specialist.
Notes
This article was externally peer reviewed.
Conflict of interest: None.
Funding: None.
To see this article online, please go to: http://jabfm.org/content/34/1/216.full.
- Received for publication May 6, 2020.
- Revision received July 25, 2020.
- Accepted for publication July 30, 2020.




{kind=link}
{kind=link}