
Abstract
Background and Objectives: Clinical decision support systems (CDSSs) may help clinicians prescribe opioids for chronic noncancer pain (CNCP) more appropriately. This scoping review determined the extent and range of the current evidence on CDSSs for opioid prescribing for CNCP in primary care, and whether investigators followed best evidence and current guidance in designing, implementing and evaluating these complex interventions.
Methods: We searched 9 electronic databases and other data sources for studies from January 1, 2008 to October 11, 2019. Two reviewers independently screened the citations. One reviewer extracted data and a second verified for accuracy. Inclusion criteria: study of a CDSS for opioid prescribing for CNCP in a primary care clinical setting. We reported quantitative results in tables and qualitative results in narrative form.
Results: Our search yielded 5068 records, of which 14 studies met our inclusion criteria. All studies were conducted in the United States. Six studies examined local (eg, health center) CDSSs and 8 examined prescription drug monitoring program CDSSs. Three CDSSs incorporated evidence-based components. Study aims were heterogeneous and study designs included both quantitative and qualitative methodologies. No studies assessed patient health outcomes. Few studies appeared to be following guidance for evaluating complex interventions.
Conclusions: Few studies have rigorously assessed the use of CDSSs for opioid prescribing for CNCP in primary care settings. Going forward, investigators should include evidence-based components into the design of CDSSs and follow guidance for the development and evaluation of complex interventions.
- Biomedical Technology Assessment
- Chronic Pain
- Clinical Decision-Making
- Clinical Decision Support Systems
- Electronic Health Records
- Information Technology
- Opioid-Related Disorders
- Outcomes Assessment
- Prescription Drug Monitoring Programs
- Translational Medical Research
Introduction
Two countries at the epicenter of the opioid crisis, Canada and the United States,1⇓⇓–4 recently released clinical practice guidelines for opioid prescribing for chronic noncancer pain (CNCP).5,6 These guidelines recommend against using opioid analgesics for CNCP as a first-line medication because the harms frequently outweigh the benefits.7⇓⇓–10 When opioids are prescribed for CNCP, the guidelines recommend risk mitigation strategies and opioid dose tapering. Both guidelines target primary care providers (PCPs), since they write about half of all opioid analgesic prescriptions in North America.11⇓–13 However, evidence shows that PCPs may have difficulty adopting recommended clinical practices.14⇓⇓⇓⇓⇓⇓–21 Clinical decision support may provide assistance.
Clinical decision support systems (CDSSs) are electronic systems that assist health care providers in clinical decision-making, by providing patient-specific data at the point-of-care.14⇓–16 Studies show that CDSSs lead to improvements in clinician performance (a care process measure), such as ordering appropriate tests and safer prescribing.17⇓⇓⇓⇓⇓⇓⇓–25 Some CDSS design components are evidence-based, including requiring a reason for an override, activating automatically (ie, the CDSS runs without requiring provider initiation), integrating into the electronic medical record (EMR), and providing advice to patients (eg, written materials), as well as clinicians.14,20,26⇓–28 These components lead to improvements in care process outcomes. Studies in which the CDSS evaluators are also the developers tend to show positive impact on process outcomes.26,27
However, the impact of CDSSs on important patient or population health outcomes is unclear,17⇓⇓–20 and widespread adoption is often limited by implementation issues.29⇓⇓⇓⇓–34 In addition, CDSSs can be difficult to develop and evaluate because they are complex interventions that seek to change the functioning of a complex adaptive system, such as a primary care clinic.35 The Medical Research Council in the United Kingdom (UK) recommends that researchers design and evaluate complex interventions through a carefully staged series of studies targeting key uncertainties, as well as a definitive evaluation.35,36 All steps should include process evaluations and assess for unintended consequences.37
CDSSs can have a variety of roles in improving adherence to opioid prescribing guidelines for CNCP. They can be used to reduce the number of new opioid prescriptions for acute pain38 and to reduce the initiation of opioid prescribing for CNCP. They can also be used to improve prescribing and other measures, like risk mitigation strategies for patients already receiving opioids for CNCP. This is the most challenging role for a CDSS as these patients are at high risk of harms and changing prescribing is very difficult.39,40
Several studies have evaluated CDSSs for opioid prescribing for CNCP in primary care settings.41⇓⇓–44 These studies report that the use of a CDSS led to a reduction in opioid prescribing or improved adherence to clinical practice guidelines.41⇓⇓–44 Several studies have also evaluated prescription drug monitoring program (PDMP) CDSSs for opioid prescribing for CNCP in primary care settings. PDMP CDSSs are large, centralized, government-run databases that prescribers can access for point-of-care information on a patient's opioid prescriptions.45,46 While 1 PDMP CDSS study found that physicians wrote fewer opioid prescription in 61% of cases,47 another study reported no association between PDMP implementation status and requirement levels (from no requirements to a mandatory requirement to check the PDMP before prescribing) and physicians' opioid prescribing for CNCP.48 Four other PDMP CDSS studies examined PCPs' use of, and views on PDMPs.49⇓⇓–52 To date, however, the literature in this emerging field has not been systematically summarized and analyzed so the benefits and risks of implementing a CDSS are unclear.
This scoping review determined the extent and range of the current evidence on CDSSs for opioid prescribing for CNCP in primary care. Our secondary aim was to determine whether researchers followed best evidence for the design of the CDSSs and current guidance for the evaluation of complex interventions.
Methods
We conducted a scoping review using the frameworks53,54 described by Colquhoun et al,55 and the methods outlined by The Joanna Briggs Institute.56 We followed the reporting guidelines from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension for Scoping reviews.57 We created an a priori protocol and used an iterative approach. Modifications included a secondary research aim and a change to the data extraction plan.
Study Eligibility
We included peer-reviewed and nonpeer-reviewed studies that used quantitative, qualitative, and mixed-methods methodologies. We excluded nonsystematic reviews, letters, opinion articles, analysis articles, clinical practice guidelines, and policy documents. We included all studies where the population was PCPs (ie, family physicians, emergency medicine physicians, nurse practitioners, and primary care internists) working in a primary care setting. Studies that reported less than 50% PCPs or did not report the percentage of PCPs were excluded, unless results were reported by subgroup. We included all studies that assessed a CDSS that sought to improve opioid prescribing for CNCP patients in a primary care clinical setting. We excluded studies where PCPs were working in a secondary and tertiary settings, such as a pain clinic or addiction clinic. We excluded primary care pediatric clinics. We defined a CDSS as an electronic system that assisted health care providers in clinical decision-making, by providing patient-specific data at the point-of-care.14⇓–16 We included studies where the CDSS was integrated into the EMR, or functioned independently (eg, Web-accessed), or was embedded within a larger intervention. We excluded studies where CDSS use was not specified, where it was used for another reason, or where it was not implemented in clinical settings.
Data Sources and Searches
We searched electronic databases (MEDLINE [via OVID], EMBASE, CINAHL, CENTRAL, PsycINFO and International Pharmaceutical Abstracts [via OVIDSP]) from January 1, 2008 to October 11, 2019. CDSSs developed before this period likely evolved or became obsolete.59 We built a comprehensive search strategy, including the terms “opioid,” and “clinical decision support systems.” Since studies used a large number of different keywords and medical subject headings for a CDSS, we had to conduct a broad search using a large variety of terms, including computer systems, health informatics, clinical decision-making (Appendix 1 Medline search strategy). The Medline strategy (Appendix 1) was adapted for the other databases. We used the Canadian Agency for Drugs and Technologies approach to our gray literature search (Appendix 2 Gray literature search).60 We also searched trial registries (ClinicalTrials.gov, World Health Organization International Clinical Trials Registry Platform), checked reference lists of additional eligible studies and contacted experts (ie, lead authors on included studies, registered protocols and systematic reviews of CDSSs).
Screening and Selection
Two researchers independently screened abstracts to determine whether they met inclusion criteria. Two researchers then independently screened the full text of all relevant articles. For both steps, after we screened 10 to 15 titles and articles, we checked inter-reviewer agreement to ensure it was at least 80% before continuing further. When there were disagreements, a third researcher (MAO) assisted in making the final decision. We contacted authors for more information when full text was not available online.58
Data Extraction
We created and pilot tested a data extraction form to record the following items: study population and setting, description of the intervention and implementation process, type of CDSS, inclusion of evidence-based CDSS components (components that the literature has consistently found to have an impact on outcomes: requiring a reason for an override; activating automatically; integrating into the EMR; and providing advice to patients and clinicians),14,20,26⇓–28 study aims, methodology and design, study outcomes, funding information, conflicts of interest, and adherence to guidance for complex interventions (eg, study was part of a stepped approach to development and evaluation), assessment for unintended consequences, planned process evaluation, process and outcome measures, theoretical approach to guide implementation and/or evaluation. One reviewer extracted data and another researcher reviewed their work (SMS, MAO, QG, SM, SH). This was a modification from our protocol that specified that 2 researchers would independently extract the data.
Data Synthesis
We used a flow diagram to report on study selection. We reported quantitative data in tabular format. We wrote narrative summaries using contextual and process-oriented data. We did not conduct a detailed assessment of study quality, assess for reporting bias, or risk of bias consistent with current guidance on conducting scoping reviews.55⇓–57
Results
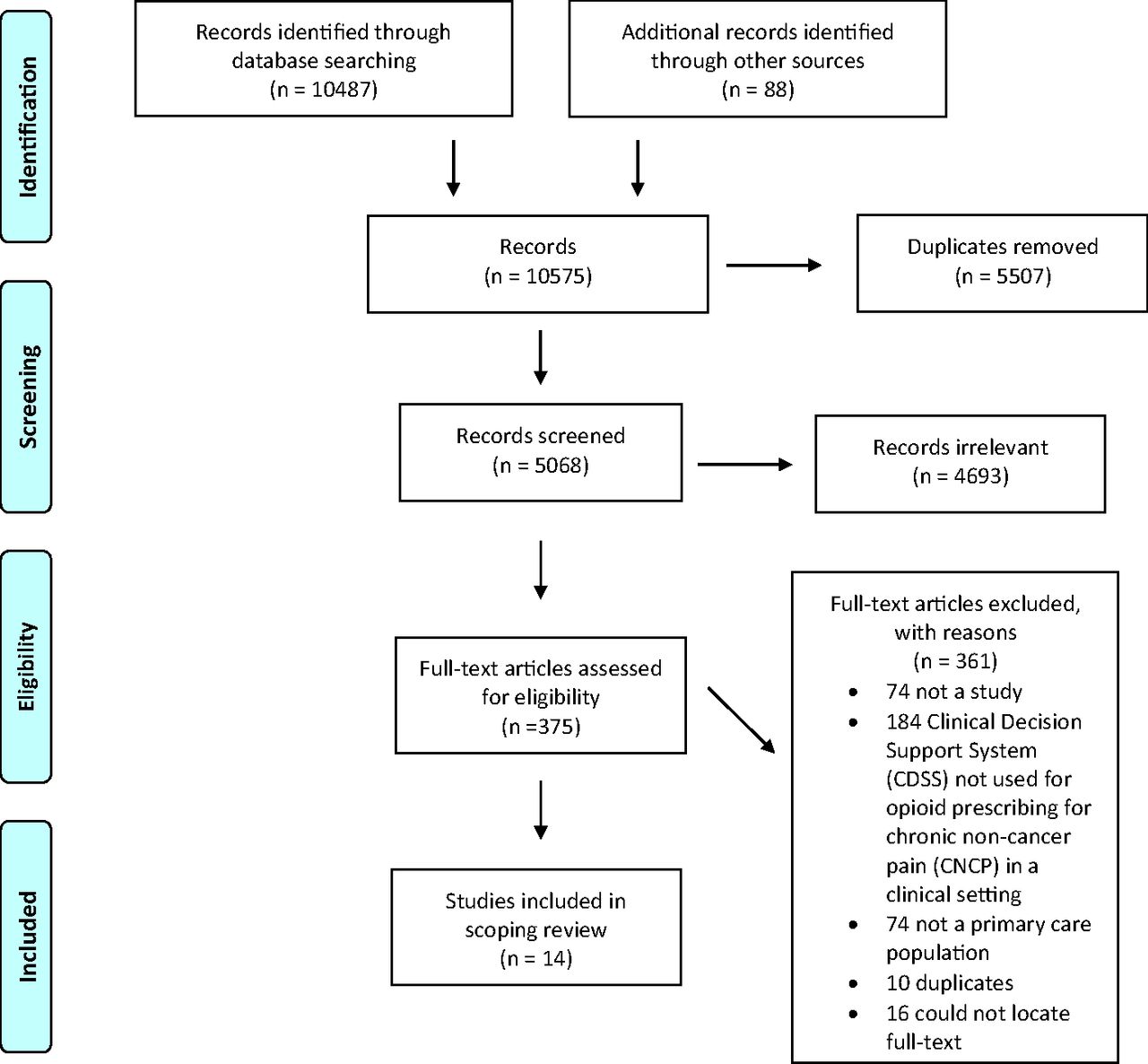
Our literature search identified 5068 citations from which 14 were included in the scoping review (Figure 1). Six studies examined local CDSSs (eg, specific health system, center or clinic)41,43,44,61⇓–63 while 8 examined state-run, Web-based, central PDMP CDSSs47,49⇓⇓–52,64⇓–66 Results using these 2 typologies are summarized in Table 1. Study descriptions are detailed in Appendix 3.

PRISMA Flow Diagram.
Study Setting, Participants, Clinical Decision Support System (CDSS) Type, and Inclusion of Evidence-Based Components
CDSS Description
Types of CDSSs included protocols (ie, forms that guide clinical management) in the EMR, Intranet dashboards, EMR alerts, data repositories and Web-based clinical tools. Four local CDSSs were integrated into the EMR43,44,62 and 2 automatically activated.44,62 The other 2 required the PCP to activate the CDSS. Studies assessing PDMP CDSSs did not report any evidence-based design components.
Study Characteristics
All studies occurred in the United States and practice settings were mostly primary care clinics. Three were set in the emergency department.44,47,49 All the local CDSSs, and 3 of the PDMP CDSS studies47,64,66 were designed to assess whether a CDSS alone or incorporated into a multi-faceted intervention improved prescribing or adherence to guidelines. The remaining PDMP CDSS studies determined providers' behavior, knowledge of, attitudes toward and use of CDSSs. Local CDSS study designs included 4 prepost interventions, a cluster randomized controlled trial (RCT) and a mixed-methods evaluation. The 8 PDMP CDSS studies included a wide variety of study designs including: 3 prepost interventions, a cross-sectional survey, 2 qualitative, 1 mixed-methods, and 1 retrospective cohort. Study aims and designs are summarized in Table 2 and described in detail in Appendix 3. One study was part of a stepped approach in evaluating a complex intervention.63 About half of the studies that assessed the impact of an intervention included a process evaluation (measures assessing if program components had been implemented as intended).41,43,47,49,62⇓–64 Two studies reported using a theoretical approach in implementation and evaluation processes.61,63
Aims and Designs of Included Studies
Implementation Processes
All the studies on local CDSSs described their implementation process, but provided little detail. None of the PDMP CDSS studies described implementation processes.
Study Findings
Local CDSSs
Anderson et al41 found that the CDSS and summary reports improved compliance with guidelines; Canada et al43 reported that a CDSS plus monetary incentives improved adherence to guidelines; Downes et al62 found that a CDSS and electronic reports reduced opioid prescribing and increased urine drug testing and use of pain contracts; Gugelmann et al44 found that the CDSS reduced opioid prescribing; Liebschutz et al61 reported that a multi-faceted intervention that included a CDSS in both study arms also reduced opioid prescribing; and Seal et al63 found in a multi-component intervention (with CDSS in both arms) that providers “abandoned use” of the CDSS.
PDMP CDSSs
Baehren et al47 found that physicians who used PDMP data wrote fewer opioid prescriptions in 61% of cases and more opioid prescriptions in 39% of cases; Binswanger et al64 found that a multi-component intervention improved adherence to guidelines; Chaudhary et al52 found that most PCPs reported always checking the PDMP before prescribing opioids to new patients. Click et al50 found that providers have positive views about PDMPs, but reported barriers in using them. Coleman51 found that in 5 of 7 records of patient prescribed opioids, providers accessed the PDMP. Freeman et al65 reported that PDMPs are key tools for PCPs and that barriers included a lack of integration; Kohlbeck et al49 reported that an educational intervention increased providers' knowledge of, behavior, and attitudes toward PDMP CDSSs; Patchett et al66 reported that a multi-component intervention increased use of a PDMP and led to a reduction in opioid prescribing.
Funding and Conflict of Interest
All but 2 local CDSS studies reported on funding for CDSS evaluation;44,62 and 3 others were missing information on funding for CDSS development.44,63 All PDMP studies except 166 provided information on funding for evaluation, but none provided information on funding for development. For all 6 local CDSS studies, the developers were also the evaluators or the relationship was unclear or not stated. No evaluators of PDMPs provided information on their relationship to the PDMP developer (Table 3).
Funding and Relationship between Developers and Evaluators
Discussion
We identified 14 studies published between 2009 and 2019 that examined CDSSs for opioid prescribing for CNCP in primary care clinical settings. Six of the studies examined local CDSSs (that were used locally within a specific health center, health system or clinic) and 8 examined PDMP CDSSs. Studies evaluating CDSS impact found that the CDSS (alone or more commonly, part of a dual or multi-component intervention) led to more appropriate prescribing practices and/or adherence to guidelines. Several PDMP CDSS studies assessed providers' views on, and/or their use of PDMP CDSSs. These studies reported frequent use of the PDMP CDSS and positive views toward the CDSS with some acknowledgment of the barriers and limitations. These findings are similar to a recent qualitative rapid review that asked providers about the use of PDMPs.67 No study in our review, however, contained an assessment of patient health outcomes or assessed for unintended consequences. In addition, in 4 studies the evaluators were also the CDSS developers, a potentially useful situation, but one that presents a potential conflict of interest,26,27 that was not addressed by the investigators. We also found that few CDSSs included evidence-based components and that in only 1 study investigators reported following current guidance for development and evaluation of complex interventions.35,36
Our finding that there were only 14 studies, and only 1 RCT, which met our inclusion criteria is surprising. In contrast, a 2015 systematic review found 7 RCT studies of CDSSs for antibiotic prescribing by primary care providers.28 There may be several contributing factors. The prescription opioid crisis only gained widespread attention in the last decade,68 and it takes time to develop a complex intervention like a CDSS.36 It is also possible that some CDSSs failed to show promise early on and development was subsequently stalled or halted. Accordingly, there are a number of reports on the development of a CDSSs for opioid prescribing for CNCP where clinical outcomes have not been reported yet.69⇓⇓–72 And finally, it is possible that CDSSs are being used without an evaluation plan, as has occurred with many PDMP CDSSs.73 This may be because of a demand for immediate solutions to the opioid crisis and an evaluation of a CDSS takes significant time and money. However, since CDSSs frequently do not improve patient outcomes,17⇓⇓–20 and may lead to unintended consequences, a comprehensive evaluation is essential.74
Most studies in our review that assessed the impact of the CDSS reported an improvement in prescribing or better adherence to clinical practice guidelines. This aligns with previous research in other fields: CDSSs have a modest impact on clinician performance (a care process outcome).17⇓⇓⇓⇓⇓⇓⇓–25 However, these results need careful interpretation. Most studies were prepost, nonrandomized control or observational designs. Although—consistent with guidance for scoping reviews55,56—we did not conduct a quality assessment; these types of study designs have greater threats to validity.75 In addition, in most of the studies, the CDSS was part of a larger intervention, so its specific impact was unclear. Another reason for caution is that no studies assessed patient health outcomes, such as quality of life, morbidity, and mortality.76⇓–78 Reductions in opioid prescribing and better adherence to guidelines may have unintended consequences.36 For example, studies report that patients often turn to illicit sources of opioids when they have reduced access to prescribed opioids, increasing their risk of overdose.79⇓⇓⇓⇓–84 Several studies in a systematic review found that heroin overdoses increased after a PDMP CDSS was implemented.74 A more recent systematic review, however, found no consistent association between population-level opioid-related harms (including heroin use and overdoses) and PDMP CDSSs.85 We also noted a conflict of interest in some studies where the developers were also the evaluators. Systematic reviews in other fields have demonstrated that when the CDSS evaluator is also the developer, outcomes are better.26,27 It is possible that developers achieve better outcomes because they design effective implementation plans,26 but it is possible that the conflict of interest leads to conscious or unconscious bias.26,86⇓⇓⇓⇓⇓–92 Interestingly, none of the studies reported funding from or involvement of for-profit entities. It is possible that CDSSs developed by for-profit entities are not undergoing a publicly reported evaluation. This is problematic, and as a recent criminal case demonstrated, can lead to potential harm to patients.93
We found that few of the CDSSs incorporated evidence-based design components. In only 1 study did researchers follow guidance for designing and evaluating complex interventions. Developers may not have incorporated evidence-based components because of the lag time between development and evaluation: when the CDSS was created the developers may not have had access to systematic reviews on the various components. The developer may also feel that the evidence does not apply to this particular subspecialty or setting.94 Another reason may be a general excitement and overconfidence in e-health technologies.95 Funders and developers may be too eager to solve the problem of unsafe opioid prescribing using eHealth technologies and are not ensuring that developers are building on information from the medical literature.95 Changes are occurring. Between 2012 and 2016, the Substance Abuse and Mental Health Services Administration funded 9 projects to integrate PDMP data into EMRs.96 Investigators might not follow guidance for complex evaluations because it is a lengthy and expensive iterative process before a definitive evaluation.35⇓–37,97 This is a widespread issue—few complex interventions seem to undergo modeling, pilot and feasibility testing,98 and many lack process evaluations.99,100 This is problematic. If researchers conduct a trial without testing components, possible causal pathways, uncertainties, contextual factors, and implementation approaches, they risk wasting resources on an expensive trial and perhaps causing harm.35,37,101 Conversely, if the evaluation takes too long, the technology could become obsolete before it gains widespread uptake.59 Adopting rapid, concurrent and iterative pilot and feasibility studies may be the best approach.102⇓–104
Limitations
There are 2 main limitations in our review. In the gray literature search we may have missed non-English-language studies, as we conducted the searches only in English. Second, several of the studies included both PCPs and other provider types (we excluded those with less than 50% PCPs), and, as these studies only reported aggregate outcomes, they may not accurately reflect the PCP population.
Conclusion and Next Steps
Our review reveals that few studies have rigorously assessed the use of CDSSs in the context of opioid prescribing for CNCP in the primary care setting. More high-quality studies are needed. Going forward, investigators should include evidence-based components into the design of CDSSs and follow guidance for the development and evaluation of complex interventions, including pilot studies, process evaluations, and an assessment for unintended consequences.
Acknowledgments
The authors would like to thank Kaitlin Fuller, Education & Liaison Librarian for the MD Program and the Institute of Medical Science; Gerstein Science Information Centre, University of Toronto.
Appendix
Medline Search Strategy
Gray Literature Search
Databases Gray Literature
Search Engine Searching
Notes
This article was externally peer reviewed.
Disclosures: None of the authors have any competing interests to declare.
Funding: This project did not receive specific funding. SS was supported by a graduate research award from the University of Toronto Department of Family and Community Medicine; SM received fellowship support in 2018 from a National Health and Medical Research Council (NHMRC) program Grant (#AP1113532) and 2019 NHMRC Early Career Fellowship (APP1158463); FS was supported by NYGH (North York General Hospital) as the Gordon F. Cheesbrough Research Chair in Family and Community Medicine; AS was supported by a graduate research award from the University of Toronto, Department of Family and Community Medicine and a research fellowship from the Medical Psychiatry Alliance, University of Toronto; QG was supported by a graduate research award from the Institute of Health Policy, Management and Evaluation, University of Toronto.
To see this article online, please go to: http://jabfm.org/content/33/4/529.full.
- Received for publication May 30, 2019.
- Revision received February 20, 2020.
- Accepted for publication February 23, 2020.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵




{kind=link}