
Abstract
Introduction: The delivery of team-based care relies on team structure and teamwork. Little is known about the landscape of team configurations in family medicine practices in the United States. Teamwork between diverse team members likely impacts both performance and physician well-being. We examined team configuration and teamwork and whether they are associated with family physician (FP) well-being.
Methods: We used data from practice demographic questionnaires completed by FPs who registered for the American Board of Family Medicine Family Medicine Certification Examination in 2017 and 2018. We grouped 14 types of health care professionals into medical assistant (MA)/nurse, nurse practitioner (NP)/physician assistant (PA), and specialist, and we characterized 3 common team configurations. We used FPs' subjective ratings to measure perceived teamwork efficiency and a validated single-item measure to identify FPs who were burned out.
Results: Among 2575 FPs in our sample, 22% worked collaboratively with MA/nurse only; 40% with MA/nurse and NP/PA or specialist; and 38% with MA/nurse, NP/PA, and specialist. The distribution of perceived teamwork efficiency was not statistically different across team configurations. In teams with greater perceived teamwork efficiency, FPs were less likely to be burned out. For FPs working with expansive teams, optimal perceived teamwork efficiency was associated with significantly reduced odds of burnout after controlling for practice and physician characteristics.
Conclusion: Most FPs practice in multidisciplinary teams. Regardless of the team structure, FPs who perceived their teams as having greater efficiency were less likely to be burned out. We found that optimal perceived teamwork efficiency was associated with significantly reduced odds of burnout for FPs in all types of team configurations. Improving teamwork efficiency may be an effective strategy for practice organizations to support not only team functioning but also physician well-being.
Introduction
Team-based care is the delivery of health services by 2 or more health care professionals working collaboratively.1 It has been increasingly embraced by family physicians (FPs) as a way to achieve the nation's quadruple aim while facing workforce shortages.2⇓⇓–5 Multidisciplinary teams have the potential to help meet the country's growing primary care needs.6 Innovative care delivery models, including accountable care organizations and patient-centered medical homes, rely on integration of care across team members to achieve better patient outcomes.7 However, simply having team members of different professions and occupations in the same practice does not guarantee seamless integration of primary care.8 Collaboration between diverse team members can be challenging due to different conceptual paradigms, vocabularies, communication styles, cultures, and positions of power. Teamwork is “dynamic, simultaneous and recursive,”9 potentially impacting both teamwork efficiency and well-being. For example, if responsibilities and expectations of each team member are not clearly communicated, the efficiency and effectiveness of the entire team suffers, which may also contribute to physician burnout.10
The delivery of team-based care relies on existing team structure. Yet, little is known about the landscape of team configurations in US family medicine practices. A recent study reported the proportions of FPs working with individuals from different health professions, such as nurse practitioners (NPs) and behavioral health specialists, but did not assess the breadth of disciplines commonly represented on FPs' teams.11 Although studies have found that interprofessional care teams and good teamwork are associated with better quality of care and patient experience,12⇓–14 the association between team configurations, teamwork, and physician well-being has not been holistically examined. Certain forms of team structure and better teamwork are associated with lower burnout among primary care physicians.15⇓–17 A recent study found that teamwork efficiency, a quality indicator of teamwork, was associated with a lower likelihood of burnout among physicians in a single health system.18
We examined team configuration and teamwork in family medicine practices and whether they are associated with physician well-being. Our first aim was to characterize common types of team configurations from a representative sample of US FPs. Our second aim was to determine if certain team configurations are more likely to have greater teamwork efficiency as perceived by FPs. Our final aim was to assess whether the odds of burnout among FPs differ by level of perceived efficiency and across configurations. We hypothesized that all types of team configurations can achieve efficiency and that perceived teamwork efficiency would be inversely associated with physician burnout.
We focused on physician well-being because of the disturbingly high percentages of FPs reporting burnout symptoms in prior studies: 25% for seasoned and 42% for early-career physicians.19,20 Adverse consequences of physician dissatisfaction and burnout include lower patient satisfaction,21,22 medical errors,23,24 higher cost of care,25 and higher physician turnover.26,27 Efficient teamwork, on the other hand, improves patient outcomes and may contribute to clinicians' well-being.14,28,29
Methods
Data Source
We used data from practice demographic questionnaires completed by FPs who registered for the American Board of Family Medicine (ABFM) Family Medicine Certification Examination in 2017 and 2018 as a representative sample of the overall population of FPs.30 All registrants were required to complete the main questionnaire, which included questions about principal practice site, practice size, and whether they worked collaboratively with other health care professionals (14 types in total). In addition to the main questionnaire, 1 of 5 subsets of questions were randomly chosen for each FP to answer, 1 of which (ie, the Mini Z questionnaire, adapted from the “Mini-Z” work experience instrument31) focused on physician satisfaction, burnout, and perceptions of teamwork efficiency. Physician demographic information was obtained from both the ABFM administrative data and the demographic questionnaire, including age, sex, race/ethnicity, and medical degree.
Outcomes
Self-reported burnout was the main outcome. We identified FPs as burned out if they reported “once a week” or more often to “how often do you agree with the following statements: I feel burned out from my work.” This single item is a validated and commonly used measure to capture the composite concept of burnout.19,32⇓–34
Explanatory Variables
Perceived teamwork efficiency was measured by “the degree to which my care team works efficiently together.” FPs rated their teamwork as having “poor,” “marginal,” “satisfactory,” “good,” or “optimal” efficiency. We grouped degrees of perceived teamwork efficiency into “poor/marginal,” “satisfactory/good,” and “optimal” to simplify analysis.
Team Configuration (Stratification Variable)
Given that a physician may work collaboratively with a single, multiple, or all the 14 types of health care professionals, we observed over 800 unique team configurations in the sample. To meaningfully examine physician burnout in the context of team, we first grouped medical assistant (MA), certified nursing assistant, licensed practice nurse, registered nurse, and care coordinator into “MA/nurse”; physician assistant (PA) and nurse practitioner (NP) into “NP/PA”; certified nurse midwife, psychiatric nurse practitioner, psychiatrist, licensed social worker, psychologist, physical or occupational therapist, and pharmacist into “specialist.” Then, we characterized 3 team configurations that are both practical and differentiable by the spectrum of members: (1) MA/nurse only, (2) MA/nurse + NP/PA or specialist, and (3) MA/nurse + NP/PA + specialist. These teams represented 96% of the sample. We excluded other team configurations (4%; eg, NP/PA only or specialist only) from the analyses.
Covariates
We controlled for potential confounders of physician well-being at the practice and physician level. At the practice level, we included practice organization (academic health center, safety net practice, eg, federal qualified health care [FQHC] or rural health clinic [RHC], hospital-owned practice, independently owned practice, and managed care/health maintenance organization [HMO] practice) and practice size (solo, small [2 to 5 physicians], medium [6 to 20 physicians], and large [>20 physicians]). In addition, we accounted for factors reflecting the FPs' practice environment, including satisfaction, control over workload, and value alignment with practice leaders.20 Finally, we evaluated the level of health-related disadvantages in FPs' practicing county by using the updated Social Deprivation Index (SDI).35,36 Counties with an SDI of ≥75 (out of 100) were identified as high deprivation. At the physician level, we included age groups (under 40, 41 to 50, 51 to 60, and over 60), sex, race, ethnicity, and medical degree (MD versus DO).
Analysis
We limited the sample to FPs who provided outpatient continuity care and who responded to the Mini Z. FPs who did not provide continuity care, for example, those working primarily in emergent/urgent care or as hospitalists, were excluded because their teamwork structure is likely different from their counterparts providing continuity care (n = 499). Because we were interested in care teams, FPs who reported working with no other health care professionals in the practice were also excluded (n = 101). If a physician registered for multiple exams in 2017 and 2018, we analyzed their responses from the latest questionnaire. Because we assumed that all teams can achieve efficiency and that no configuration is necessarily superior in improving efficiency, we stratified the sample by team configuration rather than choosing 1 as the reference group.
First, we examined the distribution of team configurations by both practice and physician characteristics. The prevalence of burnout was calculated by the same set of variables. We then stratified the sample by team configuration and assessed FPs' perceived teamwork efficiency. Furthermore, we examined the variations in the percentage of FPs who were burned out by degrees of perceived teamwork efficiency nested in care team configuration. In adjusted analyses, we estimated the association between FPs' perceived teamwork efficiency and burnout in logistic regression models stratified by team configuration, adjusting for all practice and physician covariates. All analyses were conducted in SAS 9.4 (SAS Institute Inc, Cary, NC). The American Academy of Family Physicians Institutional Review Board approved this study.
Results
Among 2575 FPs in our sample, 22% worked collaboratively with MA/nurse only; 40% with MA/nurse and NP/PA or specialist; and 38% with MA/nurse, NP/PA, and specialist (Table 1). Team configurations varied considerably by practice organization (P < .001) and practice size (P < .001). FPs worked collaboratively with a MA/nurse, NP/PA, and specialist configuration most frequently in safety net practices (74%), academic health centers (63%), and managed care/HMO (50%) practices and least frequently in independently owned practices (14%). In contrast, teaming with MA/nurse and either NP/PA or specialist was the most prevalent configuration among FPs in hospital-owned (46%) and independently owned (46%) practices.
Care Team Configurations of Family Physicians in Continuity Practice by Practice and Physician Characteristics
As expected, FPs in larger practices were more likely to work with a broader spectrum of health care professionals; the majority of FPs in large (62%) and medium practices (50%) worked with all 3 types of health care professionals. Over half of FPs in small practices worked with MA/nurse plus either NP/PA or specialist. Three in 4 solo FPs (75%) worked with MA/nurse only. The percentage of FPs working with MA/nurse plus either NP/PA or specialist was 36% in highly deprived counties compared with 41% in less-deprived counties; and the percentage of FPs working with MA/nurse only was 25% in highly deprived counties compared with 21% in less-deprived counties (P = .04). Compared with those who rated practice environment less favorably, FPs with more favorable practice environment were overall more likely to work with more expansive teams and less likely to work with MA/nurse only. FPs working with MA/nurse only were more likely to be older (over 60), male, MD, Asian, and Hispanic.
Overall, 80% of the FPs perceived their teamwork efficiency as good, 14% as optimal, and 7% as poor (Table 2). This distribution of perceived teamwork efficiency was not statistically different across team configurations according to Pearson's chi-squared test (P = .27).
Perceived Teamwork Efficiency by Care Team Configuration
Forty-one percent of FPs reported feeling burned out once a week or more (Table 3). The likelihood of burnout was not statistically different across team configurations (P = .17). Burnout was more prevalent in younger (under 60), female, MD, non-Asian, and non-Hispanic physicians. The prevalence of burnout varied across practice organizations, with the lowest in academic and highest in hospital-owned practices. FPs in solo practices were less likely to report burnout than others in larger practices. Burnout was less prevalent among FPs practicing in highly socially deprived counties (35% vs 43% in counties with lower deprivation, P = .002). Burnout was reported by nearly 7 in 10 FPs (68%) who were not satisfied with their practice but also by a substantial 35% of those who were overall satisfied. Burnout was much less likely among FPs who had better control over workload (30% vs 67%, P < .001) or whose values aligned with the practice leaders (32% vs 58%, P < .001).
Prevalence of Burnout by Team Configuration and Practice and Physician Characteristics
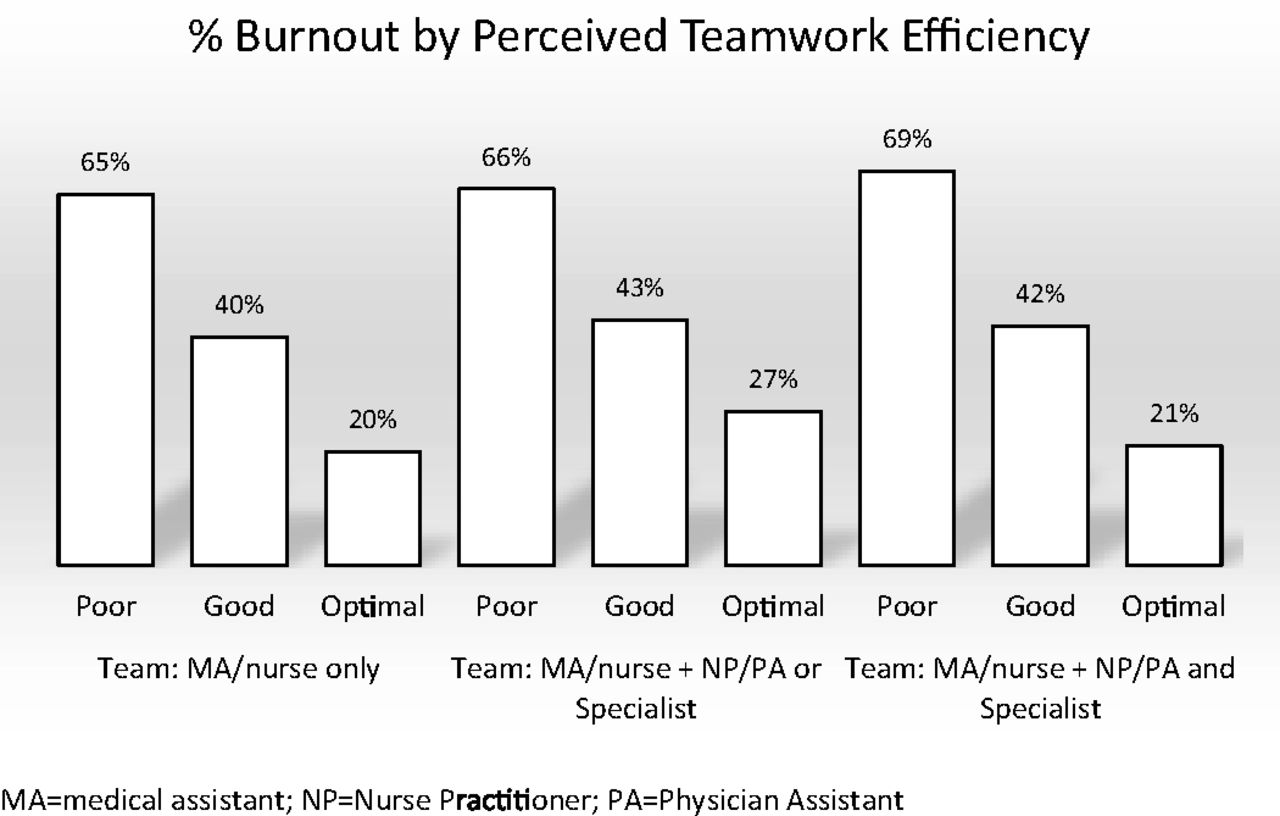
The percentage of FPs who were burned out clearly varied with degrees of perceived teamwork efficiency, irrespective of team configuration (Figure 1). FPs in teams with optimal perceived efficiency reported the lowest rates of burnout (20% to 27%). Most FPs perceived their teamwork efficiency to be good, of whom 40% to 43% were burned out. The risk of burnout increased to 65% to 69% for FPs whose perceived teamwork efficiency was poor. The pattern of burnout variations by degree of perceived teamwork efficiency was nearly identical for all team configurations.

Family physician burnout by perceived teamwork efficiency.
After adjusting for practice and physician variables, our hypothesis about the inverse relationship between perceived teamwork efficiency and physician burnout was confirmed for the more expansive team configurations, with a strong trend as well for teams with MA/nurse only (Table 4). For FPs working collaboratively with an MA/nurse and NP/PA or specialist, optimal (vs poor) perceived teamwork efficiency was associated with 46% lower odds of burnout (P = .04). For FPs in teams with an MA/nurse, NP/PA, and specialist configuration, the odds of burnout were 60% lower when perceived teamwork efficiency was optimal as opposed to poor (P = .01). Optimal perceived teamwork efficiency trended toward lowering the odds of burnout for FPs working with MA/nurse only, but the association was not statistically significant.
Logistic Regression Estimates of Perceived Teamwork Efficiency on Burnout, Stratified by Team Configuration
Discussion
This study was the first to characterize the care team configurations of practicing FPs by using a nationally representative sample and to examine the association of perceived teamwork efficiency and burnout across these configurations. We found a strong association between optimal perceived teamwork efficiency and reduced burnout across various team configurations. This protective association against burnout was significant after controlling for other organizational factors. As working with an NP/PA or a specialist or both are prevalent in all types of practice organizations, particularly in safety net practices (98%) and academic health centers (94%), improving teamwork efficiency would be an effective organizational strategy to combat physician burnout.37
We found a strong trend but not a significant association between optimal perceived teamwork efficiency and burnout for FPs working with MA/nurse only (adjusted odds ratio = 0.58, P = .07). However, it would be premature to conclude that perceived teamwork efficiency is not an important factor for burnout for FPs with a simpler team structure. The relatively small number of FPs in the reference group—poor perceived teamwork efficiency (n = 34)—might have limited the power to detect differences. Future studies with a larger sample size are needed to re-examine this association.
The success of team-based care relies on efficient teamwork. We measured teamwork efficiency by physician perceptions and found a pattern that holds true for all team configurations: in teams with greater perceived teamwork efficiency, FPs were less likely to be burned out, and vice versa. The distributions of perceived teamwork efficiency were comparable across different configurations, confirming our assumption that no team is necessarily superior in improving efficiency by design. Therefore, improving efficiency may be an attainable goal for all teams regardless of team structure.
On the other hand, poor perceived teamwork efficiency would put physicians at a higher risk for burnout and, thus, compromise the foundation for achieving the triple aim.5 Therefore, although FPs are increasingly practicing in teams, continuous efforts are required to assess how efficient the team works together after the team structure is in place. Timely action can be taken to prevent adverse consequences to team functioning, to physician well-being, and ultimately to patient care.
As expected, practice organization and practice size influenced what type of team FPs collaborated with. For example, NP/PA or specialist were available in 98% of the safety net practices, in 80% of hospital-owned practices, but in only 61% of independently owned practices. Only 25% of solo FPs worked with an NP/PA or specialist, who were accessible in 92% of medium-sized practices. These findings provide an overview of FPs' team structure in various organizations but also reveal areas where team-based care may not be adequately supported, for example, 20% of the FPs in hospital-owned practices had no NP/PA or specialist on their team.
In 2017 and 2018, 2 in 5 practicing FPs (41%) reported burnout symptoms. The prevalence is similar to that in a national sample of early career FPs,19 suggesting that burnout seems to affect physicians of all career stages. It is worth noting that despite apparent conceptual contradiction, 35% of the FPs simultaneously report satisfaction with their practice and burnout symptoms, suggesting the need to be alert to potential burnout symptoms even among satisfied physicians. Last but not least, practicing in highly socially deprived counties was a significant risk factor for burnout for FPs working with MA/nurse only but not for FPs working with an NP/PA or a specialist or both. A possible explanation may be that a scarcity of resources becomes a catalyst for physician burnout when the practice team does not have specific expertise to support patients with social needs.38 Therefore, preparing current team members and also bringing new professionals whose expertise is in addressing social needs may benefit not only the patients but also the physician.
Limitations
First, although our team configuration measure was designed to be inclusive, it did not assess the “tightness” of the collaboration between team members.15 Second, individuals who constitute the care team for FPs may map to only a part of the team configuration. It is possible that FPs indicated working with multiple care professionals but were referring only to a smaller group of the team, or “teamlet,”39 when rating the level of teamwork efficiency. Third, we lacked data to uncover what distinguished optimal from good perceived teamwork efficiency. Future research, especially qualitative work, is needed to provide organizations with practical guidance for improvement. Last, we examined physician's perceived teamwork efficiency, which may not reflect actual clinical performance. Future studies are warranted to investigate the agreement between perceived and actual teamwork efficiency.
Conclusions
Most FPs practice in multidisciplinary teams. We found that optimal perceived teamwork efficiency was associated with significantly reduced odds of burnout for FPs in all types of team configurations. Improving teamwork efficiency may be an effective strategy for practice organizations to support not only team functioning but also physician well-being.
Notes
This article was externally peer reviewed.
Conflicting and competing interest: The authors declared no conflict of interest.
Funding: This study was not funded.
To see this article online, please go to: http://jabfm.org/content/33/3/368.full.
- Received for publication September 24, 2019.
- Revision received January 20, 2020.
- Accepted for publication January 26, 2020.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- The effect of general practice team composition and climate on staff and patient experiences: a systematic review
- Qualitative examination of collaboration in team-based primary care during the COVID-19 pandemic
- Revitalizing Primary Care, Part 2: Hopes for the Future
- Well-Being, New Technologies, and Clinical Evidence for Family Physicians