
Abstract
Background and Objectives: The goal of this study was to decrease admission and readmission rate for the 2296 Medicaid patients in our clinic. Our focus was to eliminate patient identified barriers to care that led to decreased quality of care. The identified barriers for our clinic included distance to care, poor same-day access, communication, and fragmented care. A team-based, collaborative approach using members from all aspects of patient care.
Methods: An initial survey identified which barriers to care our patients felt obstructed their care. With this data, along with a national literature review, our team used biweekly quality team meetings with LEAN methodology and Plan-Do-Study-Act cycles to create a 4-phase quality improvement project. A home-visit program to decrease distance to care, walk-in clinic to improve same-day access, strengthened collaboration with outside care managers and clinic staff to improve communication, and the introduction of an in-house phlebotomist to improve fragmented care were created and studied between June 2015 and December 2018. Admission rate, avoidable readmission rate, as well as other quality of care measurements were assessed with electronic medical record reports and through North Carolina Medicaid data reports.
Results: Overall Medicaid admissions decreased 32.7% from starting numbers, 40.2% below expected benchmarks. Avoidable readmissions decreased 41.8%, 53.8% below the expected benchmark. Improvements in same-day access numbers and lab completion rate were also seen.
Discussion: The team-based approach to eliminating patient-identified barriers decreased both admissions and avoidable readmissions for our Medicaid patients. It also improved quality-of-care measures. This approach has been shown to be beneficial at our clinic and can easily be replicated in other settings.
- Ambulatory Care Facilities
- Electronic Health Records
- Health Services Accessibility
- House Calls
- Medicaid
- North Carolina
- Patient Readmission
- Primary Health Care
- Quality Improvement
- Surveys and Questionnaires
Introduction
Primary care provides the first line of access to health care by providing high-quality care in an efficient manner with an emphasis on patient experience. However, due to multifactorial barriers surrounding access to primary care, many patients do not get the care that they need, which in turn allows their condition to progress to the point of needing care in settings such as the Emergency Department (ED) or hospital.1
At Coastal Family Medicine, our residency clinic panel size is approximately 4000 patients: 56% of our patient population has primary Medicaid coverage and an additional 13% have secondary Medicaid coverage. Through regular assessments of our panel, we noted multiple social determinants of health that negatively impacted our patients’ care and access to our clinic. In a review of the national literature, the most common patient barriers include distance to care, difficulty with attending multiple appointments, accessibility of appointments, and cost of care.2 Another study showed that approximately 21% of the general population face nonfinancial barriers to care. In addition, 66.8% of the population with financial barriers was noted to have nonfinancial barriers as well.3 This reflects the confounding effect of poverty toward social determinants of health. This became even more prevalent after the passing of the Affordable Care Act with the national insured rate improving 6.2 to 9.5% from 2013 to 2016.4 Even if a patient has coverage and access to care, there still may be barriers limiting the health care they can receive.5 The affect can be seen in a 2015 study where Medicaid patients are 1.8 times more likely than privately insured patients to be admitted urgently or emergently for diagnoses such as diabetes 6 A 2015 survey of 110 Coastal Family Medicine patients yielded similar results to these national studies with distance to the clinic (52 responses, 47%), clinic availability (40 responses, 36%), difficulty being able to make it to different clinic sites (25 responses, 23%), and hours of operation (33 responses, 30%), and clinic communication (28 responses, 25%) being the most common patient-identified barriers to care.
Our team decided to directly address the most common patient-identified barriers to care from our survey in an attempt to improve quality of care as well as decrease both Medicaid admissions and preventable readmissions to the hospital. This was accomplished by constructing a long-term, 4-phase project rooted in addressing and eliminating these barriers for our patient population.
The 4 barriers selected were distance between the patient and their care, limited same-day access, communication, and fragmented care. These barriers were shown to be prevalent in the national literature as well, especially for patients with lower socioeconomic status.7 Patients who were unable to get to the clinic have been shown to be at vulnerable to avoidable hospital admissions8 and lack of same-day access has shown similar increases in hospitalization from patients who wait to seek care until they are at the point of hospitalization.9 Even after a patient has established with a clinic, poor communication can lead to adverse outcomes.10 Improved communication is a key component of care coordination that has been shown to improve health outcomes and lower health care spending.11 Patients dealing with fragmented care at multiple site locations has been shown to lead to increased rates of nonadherence and decreased quality of care. This can be improved with services such as on-site pharmacy, and on-site phlebotomy to decrease the trips a patient has to take to complete their care.12
The team-based approach to quality improvement has been shown to be beneficial not only in the initial phases of improvement but with sustainability of results.13 Having voices from all areas of the clinical system present through the improvement process gives a wider scope of the issues at hand as well as potential solutions.14 Before this study, our team collected data on low acuity pediatric emergency department visits and found that tailoring our interventions toward patient level interventions using a team-based approach was successful in decreasing these types of visits.15 Our current 4-phase quality improvement intervention was created in a similar fashion to assess if our process could benefit the entirety of our Medicaid population for hospital admissions, avoidable readmission rate, and measures in quality of care by using an expanded collaboration and full team-based approach.
Methods
Using LEAN methodology, our clinic held a 2-day Kaizen event aimed at improving our clinic’s services, patient experience, as well as clinic flow. The LEAN process for quality improvement is a team-based framework dedicated to assessing the current state of a process and eliminating waste from the system, creating an optimized flow where all work has value.16 From there, our process consisted of multiple Plan-Do-Study-Act (PDSA) cycles focusing on our patient identified barriers to care, which was then broken down into 4 phases. These PDSA cycles were managed at biweekly quality team meetings that consisted of members from our clinic faculty physicians, medical director, practice manager, resident physicians, front desk staff, rooming staff, phone operators, pharmacy team, and medical students. In addition in attendance were the Care Manager and Provider Services Team members from Community Care of the Lower Cape Fear (CCLCF), a local independent, nonprofit, partnering with Primary Care Providers and other community organizations to improve the quality of care and health care costs in our region. In this setting we were able to produce multiple ideas and standard work algorithms to structure our interventions. By having members representing all aspects of our clinic team as well as CCLCF representatives, we were able to gain valuable perspective from all members of the patient’s care team. This team was responsible for managing our process throughout the 4 phases of intervention.
Distance
The first phase to improve care for our patients began in 2015, establishing a home-visit program designed to bring care to our sickest patients who had limited mobility and are homebound. This eliminated the barrier of traveling distance to the clinic. We focused on the most vulnerable patients on our panel including patients with the highest ED use, patients with the highest admission rates, and patients who were homebound who had difficulty getting to the clinic site. A multidisciplinary team consisting of attending physicians, resident physicians, pharmacists, pharmacy residents, nursing staff, and medical students all took part in visiting patients in their home settings to deliver quality care, which they were unable to obtain in the traditional medical system. The visits completed home safety checks as well as pharmacy medicine reconciliations and education. Care gaps (including any missing lab work and vaccines) and any acute issues were also addressed. Patient Emergency department use and admission rate were monitored during this phase through electronic medical record reports as well as through Medicaid database reports of our clinic data versus statewide benchmarks.
Same-Day Access
Phase 2, which began in 2016, started another PDSA cycle focused on an additional patient barrier: improving same-day access and clinic availability. Through our collaborative quality team, we began reevaluating our clinic process for same-day access patients. Common feedback from our patient surveys included that people had trouble getting same-day appointments for acute issues. This led to patients going elsewhere for care, including the ED. Using multiple A3s, a LEAN process of assessing current state issues, identifying problem areas, and eliminating wasted opportunities, our collaborative team created a solution of offering Monday to Friday walk-in hours from 8 am to 5 pm, using resources already present in our current system. This service line became operational in September 2016. Instead of calling for an appointment that may not be available that day, patients were instructed to come to the clinic between those hours to be seen. The changes were worked into our current schedule and required no increase in staffing or physician presence. Same-day visit completion data and emergency department use were monitored through Electronic Medical Record (EMR) reports. CCLCF monitored our Medicaid cost per patient, admissions, and ED use.
Communication
In January 2018, our third phase of PDSA cycles began assessing the clinic-patient communication barrier. Our multidisciplinary team worked to focus on 2 interventions. The first created a “no-show” letter and call policy for our clinic. Letters were generated whenever a patient did not come to 1 of their appointments and the letter was mailed to their residence. These letters discussed barriers to care and ways to partner with our clinic to aid in receiving the care they needed. It also gave a direct phone number to our practice manager for the patient to discuss how we could best meet their care needs. Our second intervention strengthened our partnership with CCLCF, using their team and resources to reach out to our Medicaid patients. Our CCLCF nurse care managers and Health Check coordinators contacted those patients with 2 or more no-show visits, as well as patients who were identified to be high risk by their providers. In speaking with patients, the care managers and Health Check coordinators were able to assess how best to get the patients the care they needed. This included providing care management services, home visits, pharmacy support and connecting patients to the appropriate resources to address patient-specific barriers including social determinants of health. The most common solutions included securing patients’ transportation to the clinic through the Department of Social Services, scheduling home visits, and rescheduling visits with the patient’s PCP.
Fragmented Care
In April 2018, our fourth set of PDSA cycles began to focus on fragmented care in multiple locations. The burden of driving to multiple offices or labs at different times was identified as a significant barrier through the patient survey. Again referring to LEAN methodology, our collaborative team determined that our laboratory testing could be optimized for improved patient care. Patients were required to travel to an offsite lab, which only yielded a 40% lab completion rate on average. We partnered with the New Hanover Regional Medical Center lab team to hire a full-time phlebotomist within our clinic to reduce fragmented care for our patients. This also aided in improving our lab surveillance of serious medical conditions. Lab order completion rate was then monitored through Epic EMR reports and CCLCF continued to monitor our Medicaid cost per patient, admissions, and avoidable readmissions.
Our target was to reach a 15% sustainable decrease in Medicaid admissions, a 15% sustainable decrease in Medicaid potentially avoidable readmissions (measured by 3 M/L Health Information System’s Clinical Risk Grouper algorithm), and maintain our current cost per patient per month to the Medicaid system. Each of these measures was tracked concurrently with Medicaid expected benchmarks, which were also calculated using 3 mol/L Health Information System’s Clinical Risk Grouper software combining Medicaid average data with our patients algorithmically assigned in Clinical Risk Groups.17
In addition, quality of care data were measured through Epic EMR reports for ED use and admissions for our home visit panel during Phase 1, by same day clinic access during Phase 2, by care coordination patient interactions in Phase 3, and through lab completion rate in Phase 4. All interventions continued from their stated start times through the entirety of the project. The project was reviewed though our institutional Institutional Review Board (IRB) as well as through North Carolina Medicaid and was granted exemption as quality improvement.
Results
Overall
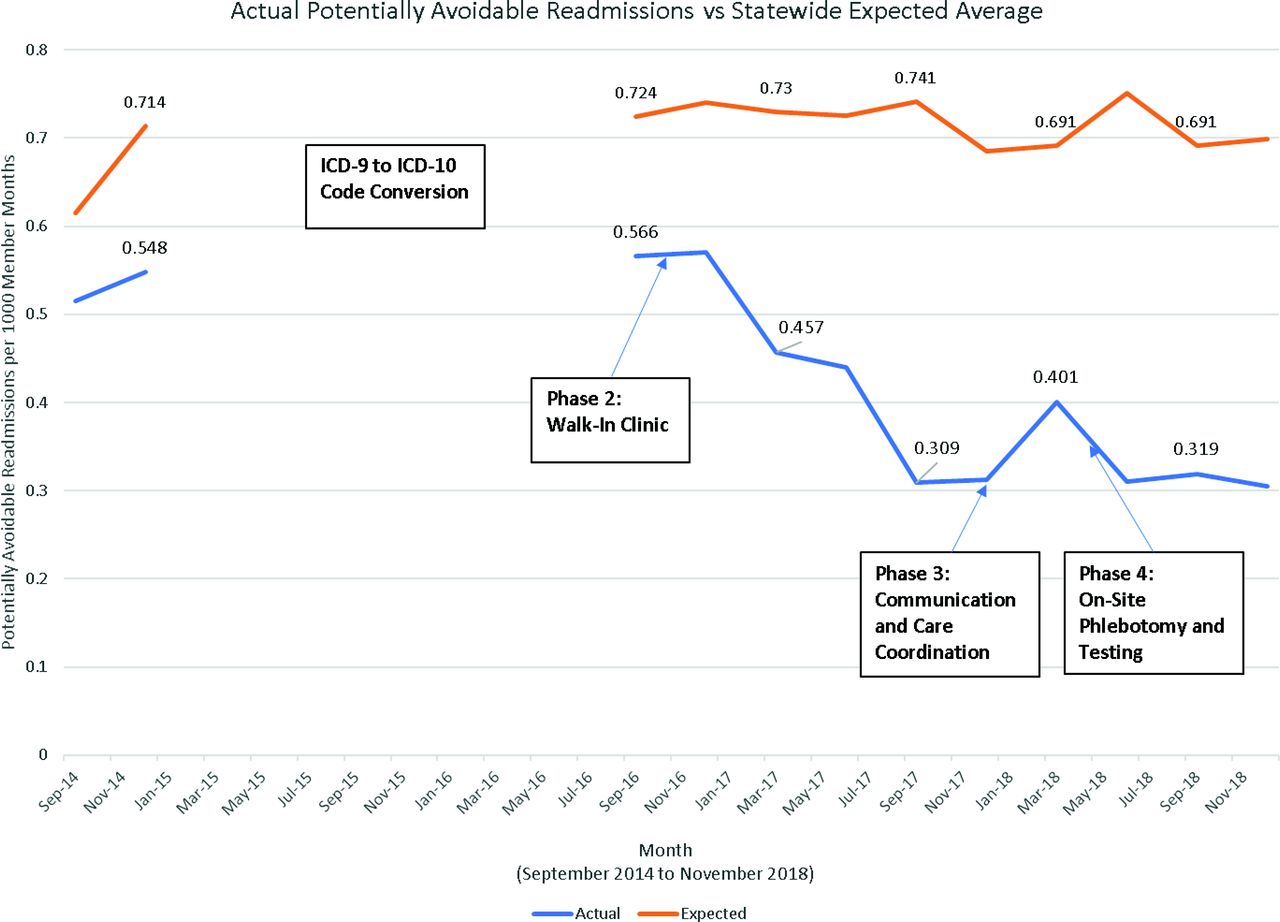
An overview of all 4 phases shows a continued and sustained downtrend of Medicaid admissions and potentially avoidable readmissions, both below the expected benchmark for the state (Figure 1 and Figure 2). After the 4 phases were complete, our Medicaid admissions improved by 32.7% from our starting rate (P < .0001), and were 40.2% below the expected benchmark data (Figure 1). Our potentially avoidable readmissions dropped 41.8% from our preintervention rate (P = .0002) and were 53.8% below the statewide expected data (Figure 2). Our cost to the Medicaid system initially showed a decrease from $207.66 per patient per month to $189.36 during our initial phase in 2015. Since that time, our cost per patient per month has remained stable, most recently at $190.40 per patient per month in December of 2018. The expected statewide benchmark cost has remained stable throughout the measured time frame, most recently at $227.07 per patient per month. We have maintained a $35 to $40 less cost per patient per month to the Medicaid system than the expected benchmark throughout the entirety of the study.

The overall trend of Medicaid inpatient admissions at our clinic vs the statewide expected benchmark. Our admission rate decreased by 32.7% through all interventions from our starting point. Before interventions our clinic was 14.3% below expected. Following interventions Medicaid admissions were 40.2% below expected. The greatest drop was seen during phase 2, the walk-in clinic phase. A decrease was also seen after Phase 1, however, the improvement was not sustained.
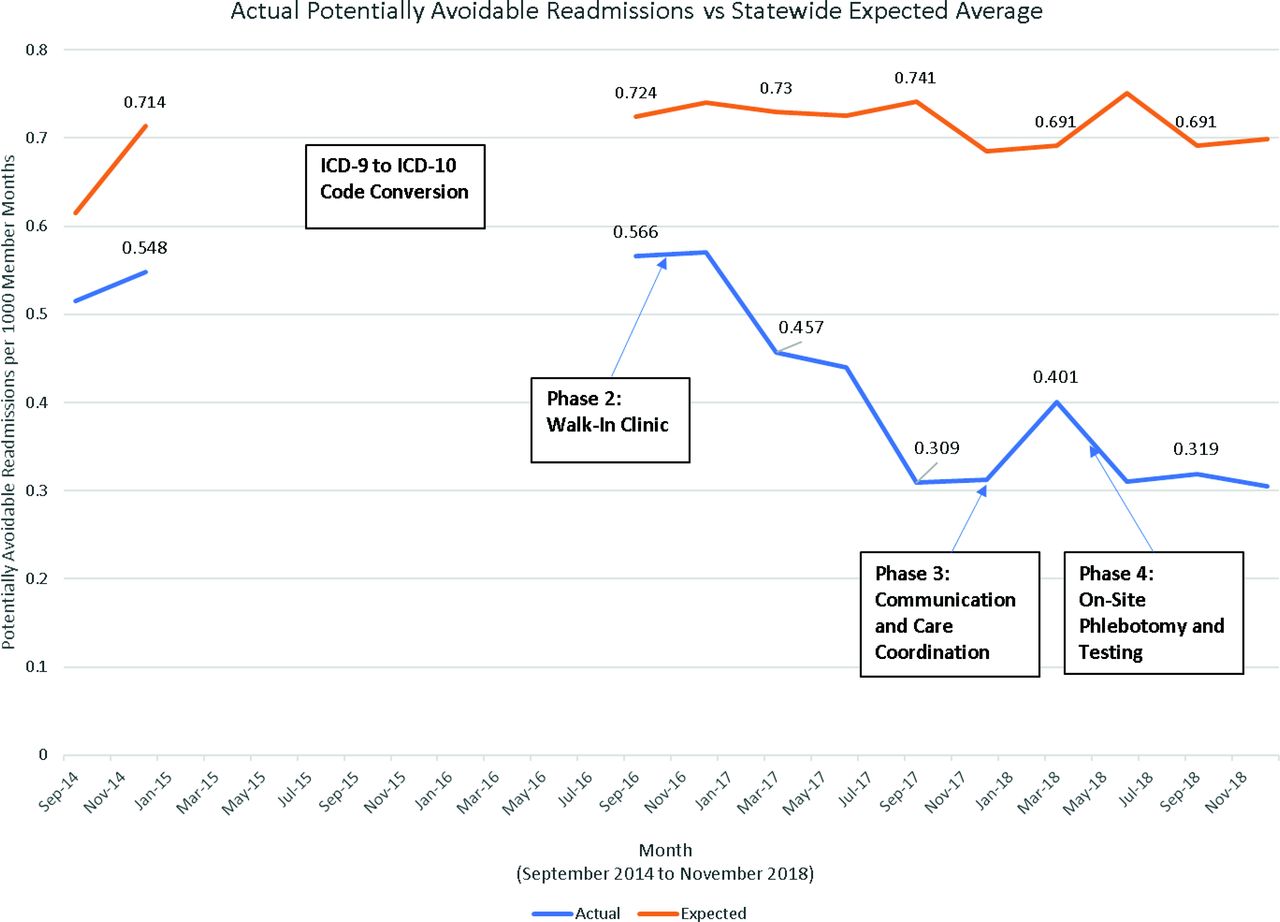
The overall trend of potentially avoidable readmissions for our clinic compared with the statewide expected benchmark. The 3 M/L panel reporting software used to collect data were unable to do so accurately during the ICD-9 to ICD-10 conversion, however, we have data from before the conversion and after. There is an overall down trend in potentially avoidable readmissions. Our clinic rate dropped 41.8% from preintervention and is 53.8% below the statewide expected. The greatest drop was seen following Phase 2. Abbreviations: ICD-9, International Classification of Disease version 9; ICD-10, International Classification of Disease version 10 .
Distance
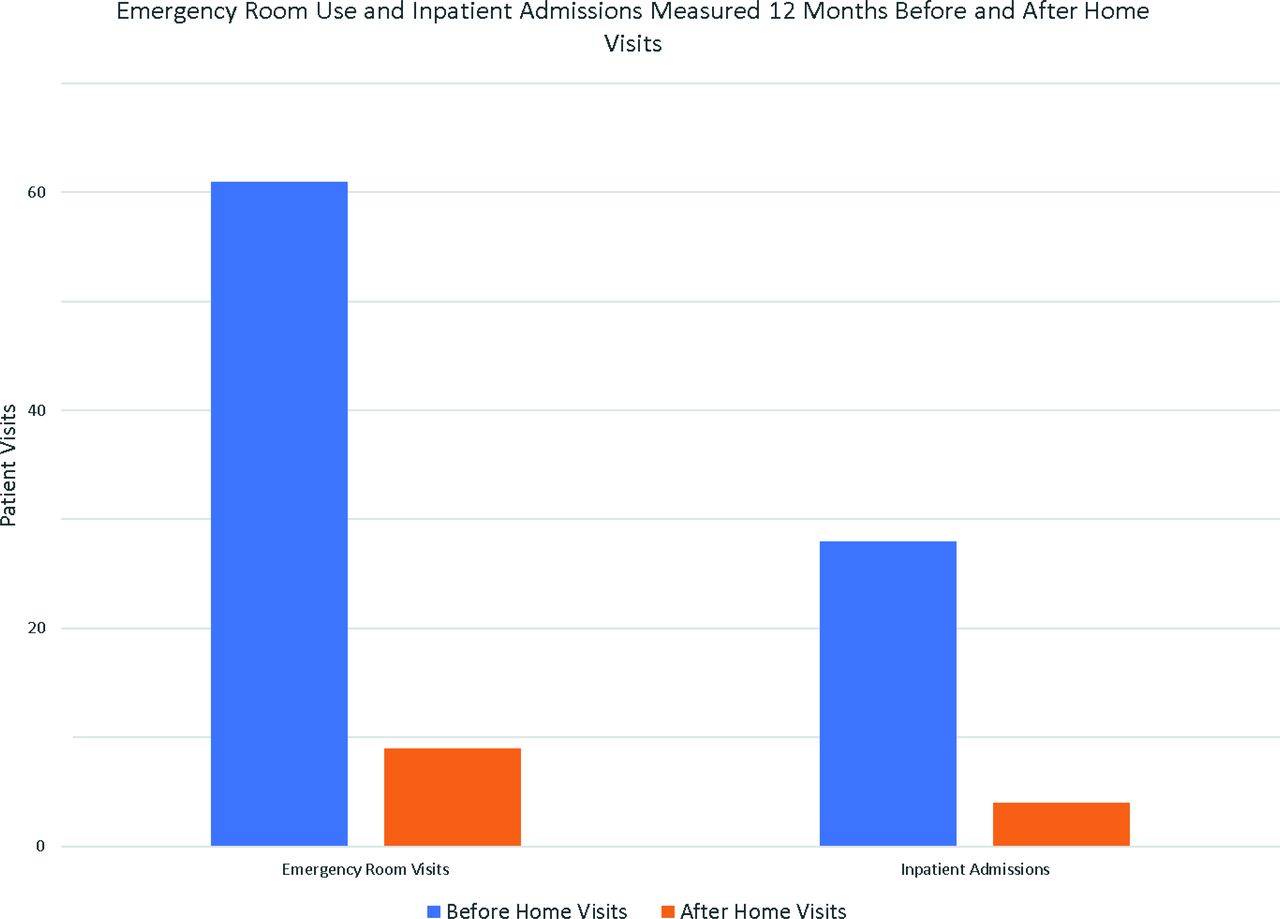
The first phase of our study showed an initial decrease in Medicaid admission rate. The initial decrease of 17.1% initiating home visits was not sustained in the 17 months before Phase 2 (Figure 1). Potentially avoidable readmissions could not be measured for this phase due to the concurrent conversion of ICD-9 to ICD-10 and the corresponding updates needed to the algorithm used to calculate the data on the 3 mol/L software. A more in-depth analysis of the home visit panel containing our 18 highest-risk patients had a combined 61 emergency department visits in the 12 months before home visits. In the 12 months of 2018, with home visits, the same 18 patients had an 85.2% decrease in ED visits (Figure 3). A similar trend was seen for inpatient admissions. In the 12 months before home visits, the 18-patient panel had 28 inpatient admissions. During the 12 months of 2018, the same 18 patients had 80.1% decrease in admissions (Figure 3).
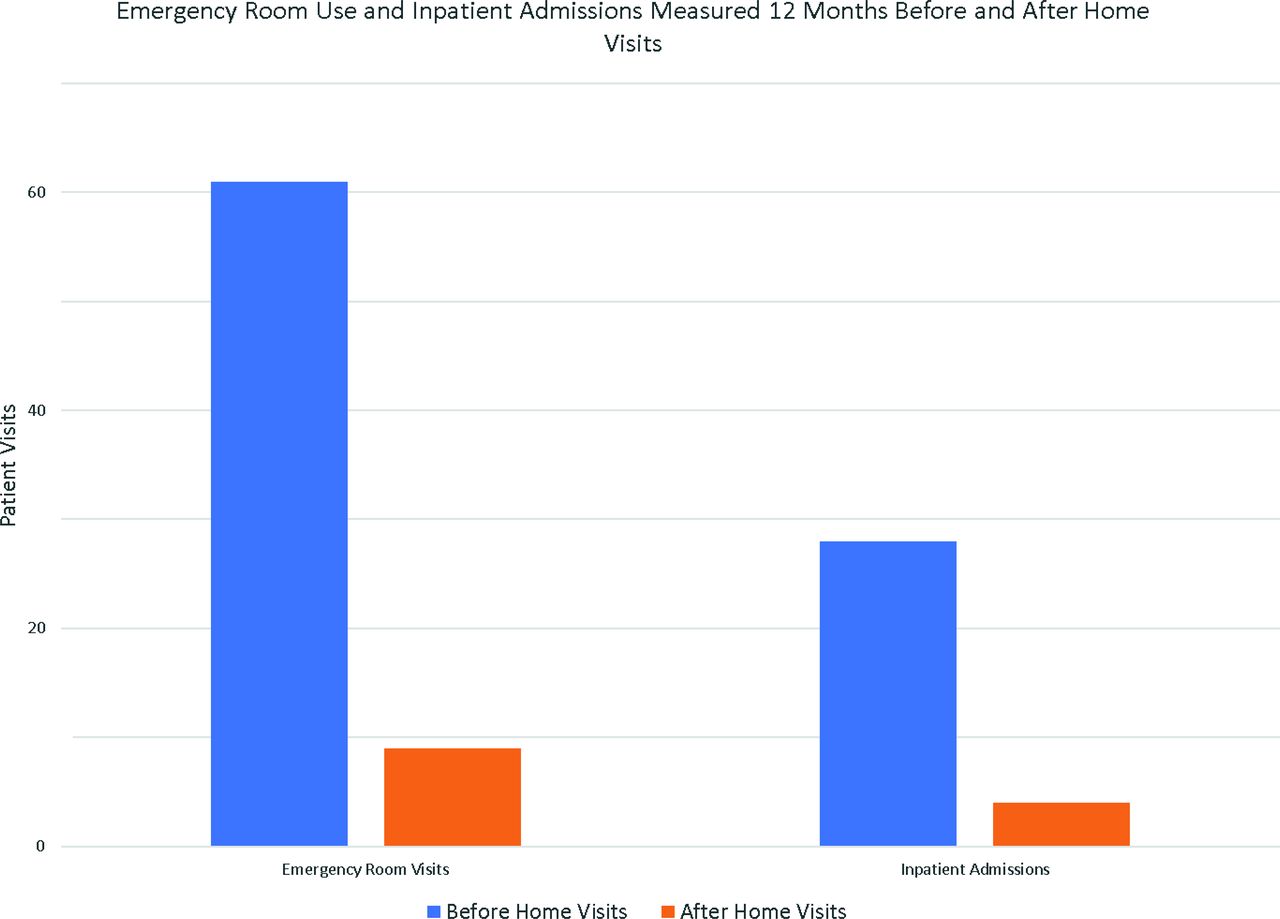
Our 18-patient home-visit panel of highest risk patients showing their use of the Emergency department (ED) and admission rate in the 12 months before and after enrollment in the home visit program. These patients were all covered either by Medicaid or with the combination of Medicare with Medicaid Secondary coverage. An 85.2% decrease in ED visits and 80.1% decrease in admissions was seen.
Same-Day Access
During the second phase, the average same-day visit completion rate rose from 57 to 214 per month, an increase in same-day access of 73.4% (Figure 4). A downtrend in our Inpatient admissions for our Medicaid population can be seen around the same time that our walk-in clinic became operational (Figure 1). There was a 28.0% decrease in Medicaid hospital admissions during this phase (P < .0001), which equates to approximately 4 Medicaid admissions per month at our panel size. A similar decrease is seen in potentially avoidable readmissions with a decrease of 45.5% during Phase 2 (P = .0001).

The increase in same day access for all patients shown in 2018 to 2019 after restructuring our process to accommodate a walk-in clinic, Monday to Friday, 8 am to 5 pm. The 2015 data were before our restructure and shows a much lower rate of completed same day visits per month.
Communication
Maximizing our relationship with CCLCF and no-show letter template did not show any decrease in Medicaid admissions or readmissions, however, did create improvement in our patient-centered care. In the last 6 months, we have been able to help multiple patients identify and address individual barriers to their health care. We have been able to plan 35 new Medicaid rides to the clinic, add 5 more high-risk patients to our home visit panel, and reschedule 243 patients for better-fitting appointments. These are patients who are more actively invested in their medical care with improved clinic-to-patient communication.
Fragmented Care
Our in-house phlebotomist did not affect Medicaid admissions or readmissions, but other quality-of-care benefits were seen. In the 8 months before having an in-house phlebotomist, our lab order completion rate ranged from 38% to 50%. Within the first month of hiring a full-time phlebotomist within our clinic, the rate jumped to 75% lab completion. In the 8 months since that time, our lab order completion rate has ranged between 90% to 95% (Figure 5). Medicaid admissions and readmissions were stable during this phase.
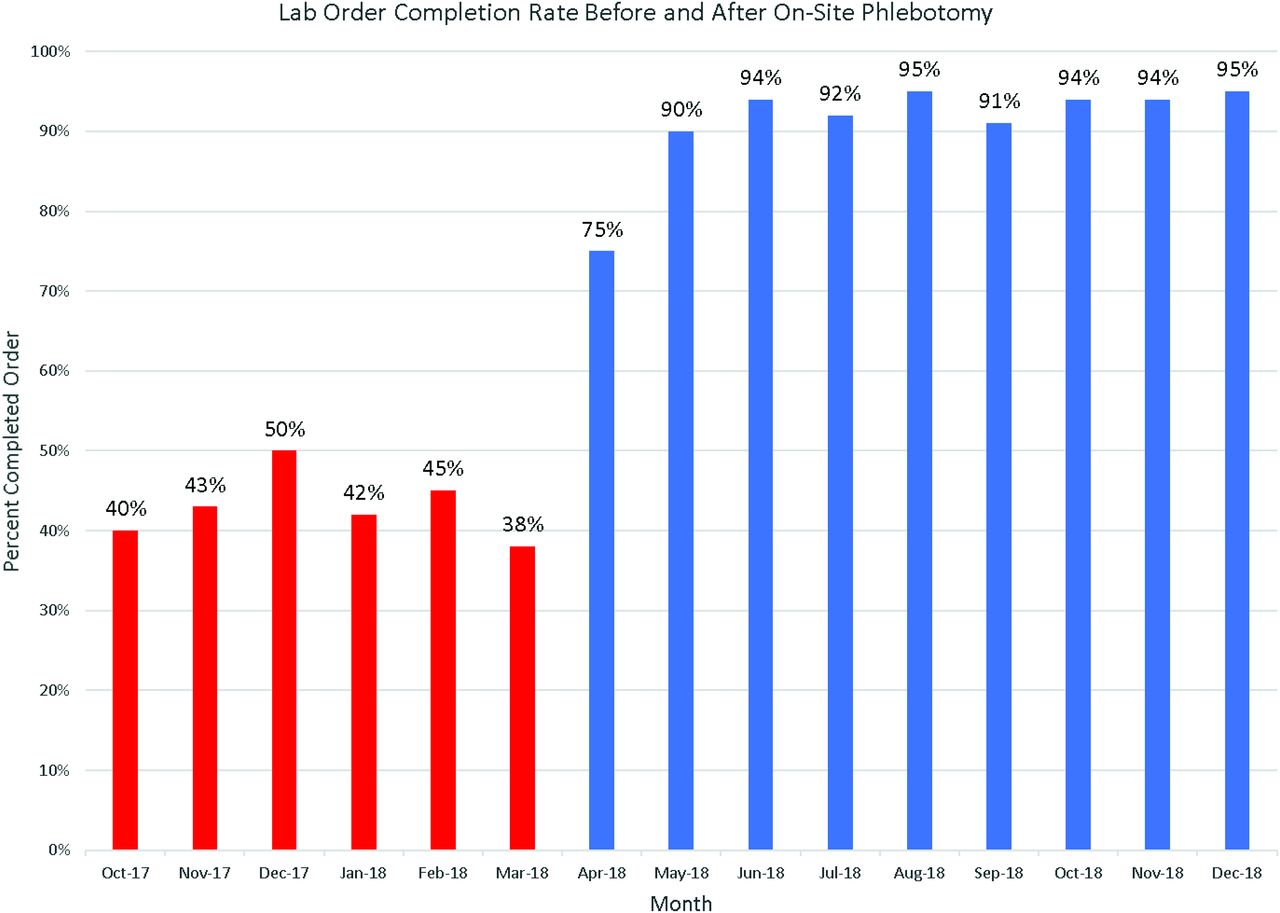
The increase in lab order completion rate after April 2018, when the in-clinic phlebotomist started, compared with the previous months with use of the off-site lab. The increase in completion rate occurred quickly and has been sustained since the intervention was initiated.
Discussion
Our clinic’s focus on reducing patient barriers to care has been a tremendous learning opportunity for our organization and has further illustrated the impact that it can have on receiving medical care. This project has also displayed that using a team-based approach can improve patient’s access to quality care by altering existing structures and routines within our clinic. With the proposed changes of Medicaid Managed Care in North Carolina and further discussions of value-based care in the health care system, these results are of importance to our medical system. Not only have these interventions showed a decrease in inpatient admissions and potentially avoidable readmissions in Medicaid patients, our cost per patient per month remains at $35 to $40 a month less than expected to the Medicaid System. If this cost difference is added to the 2296 patients on our panel primarily insured by Medicaid, this amounts to $80,000 to $91,000 a month. This demonstrates the vital role primary care plays in a sustainable medical system. Not only are family physicians capable of higher quality care for patients, they are capable of doing so without unnecessarily draining the system of funding.
Our home-visit program was able to decrease both ED use and admissions for our highest-risk patients. Due to the limit of resources and the labor-intensive process of home visits, our panel could only hold around 20 patients at a time. Even though the results for the patients who received the services were positive, it had a less sustainable effect on overall Medicaid admissions. This was likely due to the number of those enrolled only represented 1% of our total Medicaid population; however, this 1% of our population held 12.1% of our Medicaid admissions before intervention. This patient panel was 3.3% of our Medicaid admissions for all 2018, postintervention. There was no effect to on-site clinic availability with this intervention given the small panel size. In our experience, while this service is not feasible for us to use on all our patients, it is very important for our most complex, high-risk patients.
Same-day-access visits went from an average of 57 visits completed per month to 224 completed per month after Phase 2 interventions. This allowed for our clinic to accommodate more patients who could be seen with urgent issues and funnel them back from the emergency department, or into the clinic before they need urgent hospitalization. This phase showed the greatest decrease in both admissions and readmissions. These decreases have now been successfully sustained for nearly 2 years. Of all the phases, this was the most complex to implement because it restructured how our clinic half days functioned. The team-based approach helped with stakeholder buy in since every member of the team had a voice in process of implementation.
Our Nurse Care managers and Health Check Coordinators from CCLCF in combination with our direct phone access and no-show letters helped bridge the communication gap between patients and the clinic. Different communication barriers among our patients complicated this barrier. Many did not have working phone numbers or valid addresses. Many did not use computers and therefore could not access our hospital’s online portal information. Care managers utilized multiple levels of communication including text reminders, article letters, phone calls, direct interaction in the clinic, and computer portal messages, to individualize patient care plans and optimize patient communication methods. These methods helped aide in rescheduling as well as securing interventions such as home visits, Medicaid ride assistance, refill assistance, and general patient education.
With the addition of an in-house phlebotomist, lab order completion rate improved to an average of 95%. The removal of travel distance between our clinic and the outside laboratory led to the improvement in completion rate and our ability to closely monitor and actively manage chronic disease states. With this phase, we saw no increase in our cost to Medicaid data. This shows that an in-house phlebotomist did not increase our use of unnecessary labs, which if proper education is not completed, could become a complication of easier access.
Limitations of this study include the use of our residency patient population, which carries a high proportion of Medicaid patients. Our patient complexity scores were assessed and found to be similar to the internal medicine residency program at our institution. Readmission rates of patients seen by residents and faculty physicians were nearly identical. In the inpatient setting our patients are cared for by our residency team, the same physicians that care for them in the outpatient setting. There were no major changes to the structure of the inpatient service during this time, however, the physicians all had knowledge of this project’s Quality initiatives and used them when counseling patients.
Looking into the future, we would like to examine what other types of services we can bring into our clinic to further improve our care to patients. We also plan to send another version of our initial barrier survey to our patients to see if there have been any changes after our initial round of interventions.
Every patient population has unique barriers to their medical care. If a health care system seeks to deliver the highest-quality care possible to its patients, these barriers need to be adequately analyzed and intervened on. However, it should be noted that these barriers do not end with improvements in access. The patient’s social situation must be examined as well to optimize their care. Multiple studies have concluded that the Medicaid population is at higher risk of missing care opportunities, admissions to the hospital, and avoidable readmissions.18 These results can be addressed through a team-based approach similar to the one taken by Coastal Family Medicine. Our team was able to improve our patients’ care by listening both to their individual voice as well as the voices of everyone on the patient’s primary care team. This approach has proven to be helpful in decreasing overall Medicaid admissions and avoidable readmissions in our setting and is something that can be easily adapted and replicated. Through our process, we have been able to bring higher-quality care to our patients while keeping inpatient admissions, avoidable readmissions, and overall costs down.
Acknowledgments
Editing credits to Carly Devis and Jesse Harlin.
Notes
This article was externally peer reviewed.
To see this article online, please go to: http://jabfm.org/content/33/2/220.full.
- Received for publication August 5, 2019.
- Revision received October 4, 2019.
- Accepted for publication October 6, 2019.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}