
Abstract
Background: Sickle-cell disease (SCD) causes significant morbidity, premature mortality, and high disease burden, resulting in frequent health care use. Comanagement may improve utilization and patient adherence with treatments such as Hydroxyurea. The purpose of this study was to describe acute-care utilization in Medicaid-enrolled patients with SCD, patient factors associated with comanagement, and adherence to Hydroxyurea.
Methods: Data from 2790 patients diagnosed with SCD, age 1 to 65+ years, enrolled at least 1 month in North Carolina Medicaid between March 2016 and February 2017, were analyzed. Outpatient visits were categorized as primary care, hematologist, and nonhematologist specialist. Nurse practitioners or physician assistants with unidentified specialty type or family practice were categorized separately. Comanagement was defined as a minimum of 1 primary care and 1 hematologist visit/patient during the study period.
Results: There were notable age-related differences in utilization of health care services. Only 34.82% of the sample was comanaged. Comanagement was higher in the 1-to-9-year-old (44.88%) and 10-to-17-year-old groups (39.22%) versus the 31-to-45-year-old (30.26%) and 65+-year-old (18.75%) age groups. Age had the greatest influence (AUC = 0.599) on whether or not a patient was comanaged. Only a third of the sample (32.24%) had at least 1 Hydroxyurea (HU) prescription. Age was the most predictive factor of good HUadherence (AUC = 0.6503). Prediction by comanagement was minimal with an AUC = 0.5615.
Conclusion: Comanagement was a factor in predicting HUadherence, but further studies are needed to identify the frequency and components of comanagement needed to increase adherence and reduce acute care utilization.
- Child Health
- Emergency Departments
- Hematology
- Hospitalization
- Hydroxyurea
- Medicaid
- Minority Health
- North Carolina
- Primary Health Care
- Sickle-Cell Anemia
- Vulnerable Populations
Sickle-cell disease (SCD) is a genetic disorder and the most common rare blood disease in the United States.1 Patients suffer from complications, including but not limited to stroke, acute chest syndrome, and severe painful crisis that contributes to morbidity and premature mortality. Individuals also suffer from significant disease burden, often resulting in a high number of hospitalizations, readmissions, emergency department (ED) visits, and other associated costs to the health care system. In 2006 people with SCD had an estimated 232,382 ED visits, 68,410 hospitalizations from the ED, accounting for an estimated $2.4 billion dollars.2 In 2010, SCD was associated with the highest 30-day readmission rate (31.9%) among all diagnoses excluding cancer and cancer-related conditions.3 Other national data representing about ⅓ of the SCD population found a similar 30-day readmission rate of 33.4% and 14-day readmission rate of 22.1%.4 Extremely high ED use has also been well described.5,6 In a prospective cohort study of SCD, health care utilization was examined in 3 EDs over 2 years and found 342 unique patients had a total of 2934 ED visits.6 Understanding there is significant health care utilization due to disease severity, there has been an increasing effort to leverage outpatient primary care providers (PCPs) using a care model in which hematology specialists and PCPs partner to comanage SCD. Primary care and outpatient management using evidence-based guidelines can improve disease burden, improve patient outcomes, and prevent the need for ED visits and inpatient hospitalizations.7⇓⇓–10
The National Heart Lung and Blood Institute (NHLBI) published the Evidence-Based Management of SCD Report, in 2014. This comprehensive guide consists of health maintenance and prevention information, including the use of hydroxyurea (HU). HU is an oral agent found to reduce the median number of SCD pain episodes per year by 44%, but is historically underutilized.11 Only 32% of general internists and 35% of pediatricians report feeling comfortable caring for SCD patients.12 In a study of 129 PCPs with greater than 10 years (median) since graduating from medical school, 80% reported relying on knowledge gained in residency when deciding how to manage SCD patients and 68% did not regularly communicate with other providers regarding their SCD patients.12 In a survey of 53 primary care physicians in North Carolina, 65% indicated they are already comfortable comanaging HU prescriptions with a SCD specialist.9 More specific to family physicians, in a large survey of over 1000 family physicians, comfort level for managing patients with SCD was low (20%); however, 80% and 68% of respondents indicated they would be willing to comanage pediatric and adults patients with a SCD specialist.13 Thus, a gap exists in the implementation of current evidence based practices in the management of SCD in the ambulatory setting.
As adults with SCD age, they are at risk for developing comorbidities unrelated to SCD. Thus, individuals with SCD are recommended to have both a PCP and a SCD specialist comanage their care. Comanagement is defined as collaborative and coordinated care that is conceptualized, planned, delivered, and evaluated by 2 or more health care providers. Nationally, there is often a lack of providers and comanagement for individuals with SCD is not common practice.11 It is possible that comanagement of patients with SCD, in combination with dissemination of evidence based guidelines, could lead to an increased comfort level of family physicians, internists, and pediatricians. Therefore we designed a dissemination and implementation project to promote comanagement between SCD specialists and PCPs. Our team partnered with Community Care North Carolina (CCNC), a statewide primary case management program for North Carolina (NC) Medicaid enrollees.14 CCNC spans 14 community-based primary care networks throughout the state and works collaboratively with physicians and other health care professionals to promote quality-improvement and care-management initiatives.14 For the purposes of this project, we defined comanagement as a minimum of 1 PCP and 1 hematologist visit/patient during the study period. We adapted the NHLBI recommendations into user-friendly tools (health maintenance charts and treatment algorithms) designed specifically for and with the input of PCPs and ED providers, which are easy to access and use. These tools are available on 2 Web sites (sickleemergency.duke.edu and www.communitycarenc.org) as well as via a mobile application (www.scdtoolbox.com).
This article reports baseline Medicaid data from NC before dissemination efforts, including 1) ED encounters and re-encounters within 7, 14, and 30 days, hospitalization and rehospitalization within 7, 14, and 30 days; 2) PCP, hematologist, nonhematology specialist visits and comanagement (at least 1 PCP and hematologist visit per patient during a 1 year period); and 3) HU prescription fills and adherence. In addition, this article will identify predictors of HU adherence and comanagement for patients insured under Medicaid in NC.
Methods
Dataset—Medicaid North Carolina
In fiscal year 2017 almost 2 million people (approximately one fifth of NC's population) were covered by Medicaid; making it the third largest Medicaid population in states that did not expand the program.15 In fiscal year 2016 there were 68,583 NC Medicaid providers.15 In partnership with CCNC, we obtained a dataset of Medicaid administrative claims of enrollees with a diagnosis of SCD including HbSS, HbSC, and HbS-thalassemia, excluding sickle-cell trait (International Classification of Diseases, [ICD] 10 CM codes: D57.0x, D57.1, D57.2x, D57.8x).
Sample
Data are reported for a cohort of 2045 patients with a diagnosis of SCD, age 1 to 65+ years, enrolled at least 12 months in NC Medicaid between March 1, 2016 and February 28, 2017. Table 1 further describes the sample. Institutional Review Board (IRB) approval and waiver of consent were obtained.
Demographic Characteristics and Enrollment in CCNC Programs (Sample = 2045)
Measures
Emergency Department Encounters and Hospitalization
ED encounters were identified using a CCNC-developed logic model that used revenue codes (450 to 452, 456, and 459) and excluding Medicare Part A crossover-inpatient, inpatient, management fee, drug and capitation claim type codes. ED re-encounters and rehospitalizations within 7, 14, and 30 days were identified using the time between the date of service listed on the ED or hospital claim and the next date of service in the subsequent claim. Individual ED Reliance (EDR) score was calculated as the total number of ED encounters divided by the total ambulatory visits (outpatient + ED encounters) per enrollee.16,17 An EDR of >0.33 is a high score.17 Inpatient claims were identified using category of service code (0015, 0017, 0018, 0040, 0041, 0051, and 0058) and with either a Medicare Part A crossover-inpatient or inpatient claim type.
Outpatient Visits and Comanagement
Outpatient visits were identified by the Current Procedural Terminology (CPT) code listed on the claim. Outpatient visit types (PCP, hematologists, and nonhematology specialists) were identified using the descriptions from the Medicare Provider/Supplier to Health Care Provider Taxonomy that matched the billing provider code and the rendering provider code listed on the claim.18 Visits were classified into the following categories: 1) PCP (including pediatrician), 2) hematologist (including pediatric hematologists), 3) nonhematology specialist (see Table 2 for the list of nonhematology specialists), and 4) nurse practitioner (NP) or physician assistant (PA) visits. NP and PA visits in which a PCP, hematology, or nonhematology specialty was indicated on the claim were included into the corresponding category. When we were unable to determine if an NP or PA visit provided primary care, hematology, or other specialty care, they were included in the NP or PA unidentified specialty type or family practice. The “Other Specialty” category includes outpatient visits not historically linked to SCD care or with a frequency of ≤1% of the total number of nonhematology specialty visits. If the billing provider or rendering provider code was either missing or did not link to a specific provider type, then those visits were placed in the “Null” category to signify they were unidentifiable. “Acute care visits” signified medical care occurred outside the ED, and were not inpatient stays but occurred in an acute care location. Comanagement is defined as a minimum of 1 PCP and 1 hematologist visit/patient during the study period. Our team discussed this definition at length and agreed this is a bare minimum and comanagement should include more than 1 visit by both the PCP and SCD specialist. However, because comanagement for patients with SCD is so rare, we agreed to examine a bare minimum of 1 visit for each.
List of Non-Hematology Specialist by Type and Visit Frequency for Age 1 to 65+ (Sample N = 2045)
HU Prescription Fills and Adherence
HU claims were identified using the drug name. Only those enrolled in Medicaid for 12 months were included in this analysis. The number of HU prescriptions filled per enrollee by age group was determined by summing the number of filled HU prescriptions over the study period for each eligible enrollee. The number of HU days supplied is the sum of the days of supply on the prescription (eg, 30-day supply) in a 12-month period per person. The duration of HU treatment days was measured as the number of days between the date of the first HU prescription filled and the last day of the study period. The number of days between breaks in treatment is the sum of days with no HU supplied, divided by the number of gaps (missing next HU prescription fill) per person.
HU adherence was categorized into 1 of the following: 1) Good—if number of days supplied is ≥80% of duration of HU treatment, 2) Fair or Moderate—if number of days supplied is 60% to 79% of duration of HU treatment, 3) Poor—if number of days supplied is <60% of duration of HU treatment.19,20
Predictor Measures
Age-related differences in SCD health service utilization have been found in several studies.16,21⇓⇓–24 Young adults that are transition aged (16 to 25 years) have particularly high rates of acute (emergency and inpatient) care utilization.23 However, 18-to-30-year-olds with SCD have the highest reported rates of acute care encounters per patient per year, before decreasing throughout middle and older ages.4 Differences in EDR depending on age have also been previously noted in SCD patients, with highest EDR noted in those transitioning to adulthood.16 For this study, patients were categorized into age categories similar to previously published groups.25,26The following groups were utilized: 1 to 9 years, 10 to 17 years, 18 to 30 years, 31 to 45 years, 46 to 64 years, and ≥65 years.25 Gender differences in frequency and intensity of pain have previously been reported. Several studies have found an increased sensitivity and lower tolerance to pain in women and have shown related increased health service utilization.27⇓–29 However, prior studies in reporting SCD pain have reported no difference in pain experiences between men and women, but higher health care utilization by men.30,31 For this study enrollees were categorized as either male or female. Number of months enrolled in the CCNC network (1 to 12 months) was obtained to account for variations in comanagement and HU adherence that could be affected by the length of time in the network. Differences in the geographic location of people with SCD have been linked to differences in health-service utilization.32 Prior studies indicate that the further away clients with SCD are from clinics, the lower the rate of health service utilization.32,33In this study patient zip codes were used to categorize the sample by county using the US Department of Agriculture Economic Research Service (ERS) 2013 Rural-Urban Continuum Codes classification to distinguish metropolitan (metro) counties by population size and nonmetropolitan (nonmetro) counties by their degree of urbanization and adjacency to metro areas.34 This method allows for consideration of regional factors such as proximity to an urban area that may influence utilization of health care services.
Analysis
Descriptive statistics, means, and standard deviations for interval variables and frequencies and percentages for categorical variables were computed to summarize demographic characteristics of the sample. Inpatient and ambulatory health care and HU utilization were summarized by frequencies, medians, and interquartile ranges (IQRs), due to skewed distributions. Utilization summaries were presented for the overall sample and by 6 age categories. Only those participants age 1 to 65+ years, who were enrolled in Medicaid for all 12 months and had at least 1 Medicaid claim for HU were included in the calculation of the HU utilization summary statistics. There were no HU Medicaid claims in the 65+-year age group, thus they were excluded from the analysis. Logistic regression models were used to evaluate participant factors' influence on comanagement and HU treatment adherence (good vs fair or poor). Both models were conditional on age, gender, rural residence, and months enrolled in the CCNC network. A regression analysis including primary care and hematology visits as main effects with their interaction (comanagement) were added as predictors in the HU adherence model. For each outcome (comanagement and HU adherence), an area under the curve–receiver operating characteristic curve (AUC-ROC) was created. AUC-ROC provides an estimate of how capable the model is of distinguishing between the outcomes. The higher the AUC the better the model is at predicting good adherence versus fair or poor adherence. When AUC = 0.5, the model does not distinguish between levels of adherence.
Results
The participants in the sample were majority female (56.82%), lived in metropolitan areas (76.19%) and had a mean age of 22.87 years old (SD = 16.41), see Table 1. Table 3 displays the summary of utilization of acute care and outpatient services of the sample.
Emergency Department Encounters, In-Patient Stays, Out-Patient Visits, Emergency Department Reliance and Co-Management for North Carolina Medicaid Enrolled 12 Months and Age 1 to 65+ (Sample = 2045)
ED and Hospital Utilization
Of the 6834 total ED encounters, 70.95% of the total sample had an ED encounter during the 12-month study period. There was a mean of 3.34 (SD = 7.51) and median of 1 (IQR = 0 to 4) ED encounters per patient for the sample. Those who were 18 to 30 years old had the highest mean and median ED encounters per patient (5.22; SD = 9.38 and 2; IQR, 1 to 6). The 31-to-45-year-old group had the second most, with 5.20 (SD = 12.15) total ED encounters. The percentage of the sample with an ED re-encounter within 7, 14, and 30 days was also highest among the 18-to-30-year-old group (30.91%, 35.20%, and 42.64%) followed by those 31 to 45 years old (20.49%, 30.36%, and 36.02%), respectively. The mean EDR was highest among 18-to-30-year-old patients (0.35) and 44.69% of this age group had an EDR of 0.33 or greater. In the 31-to-45-year-old age group, the mean EDR was 0.27 and 34.01% had an EDR of 0.33 or greater. The overall sample had a mean of 1.32 (SD = 2.78) hospitalizations/patient. The 18-to-30-year-old age-group also had the highest mean total hospitalizations (2.26, SD = 3.91) and mean rehospitalizations within 7 (0.16; SD = 0.78), 14 (0.44; SD = 1.78), and 30 (0.89; SD = 2.97) days. The 31-to-45-year-old age group had the second most hospitalizations/patient and rehospitalizations (Table 3).
Outpatient Visits and Comanagement
The 46-to-64-year-old and the oldest (65+ years) of the sample had the highest median number of total outpatient visits (9 each), as well as nonhematology specialty visits (4 and 4.5), respectively. The youngest (1 to 9 years old) and the oldest (65+ years) had the highest median number of PCP visits (3 and 4, respectively). Participants that were age 1 to 9 years had the highest median number of hematology visits.1 Overall, there were a large total number of nonhematology specialist visits: 8827 (Table 2). Outpatient acute care visits, PA and NP visits accounted for 60% of the total number of nonhematology specialist visits. Only 34.82%, however, of the study sample met our definition of being comanaged. Comanagement was higher in the 1-to-9-year-old (44.88%) and 10-to-17-year-old groups (39.22%) versus the 31-to-45-year (30.26%) and 65+-year (18.75%) age groups, see Table 3. Age had the greatest influence (AUC = 0.599) on whether or not a patient was comanaged, whereas, gender, months enrolled in CCNC, and residence had very little predictive influence on comanagement (Figure 1).
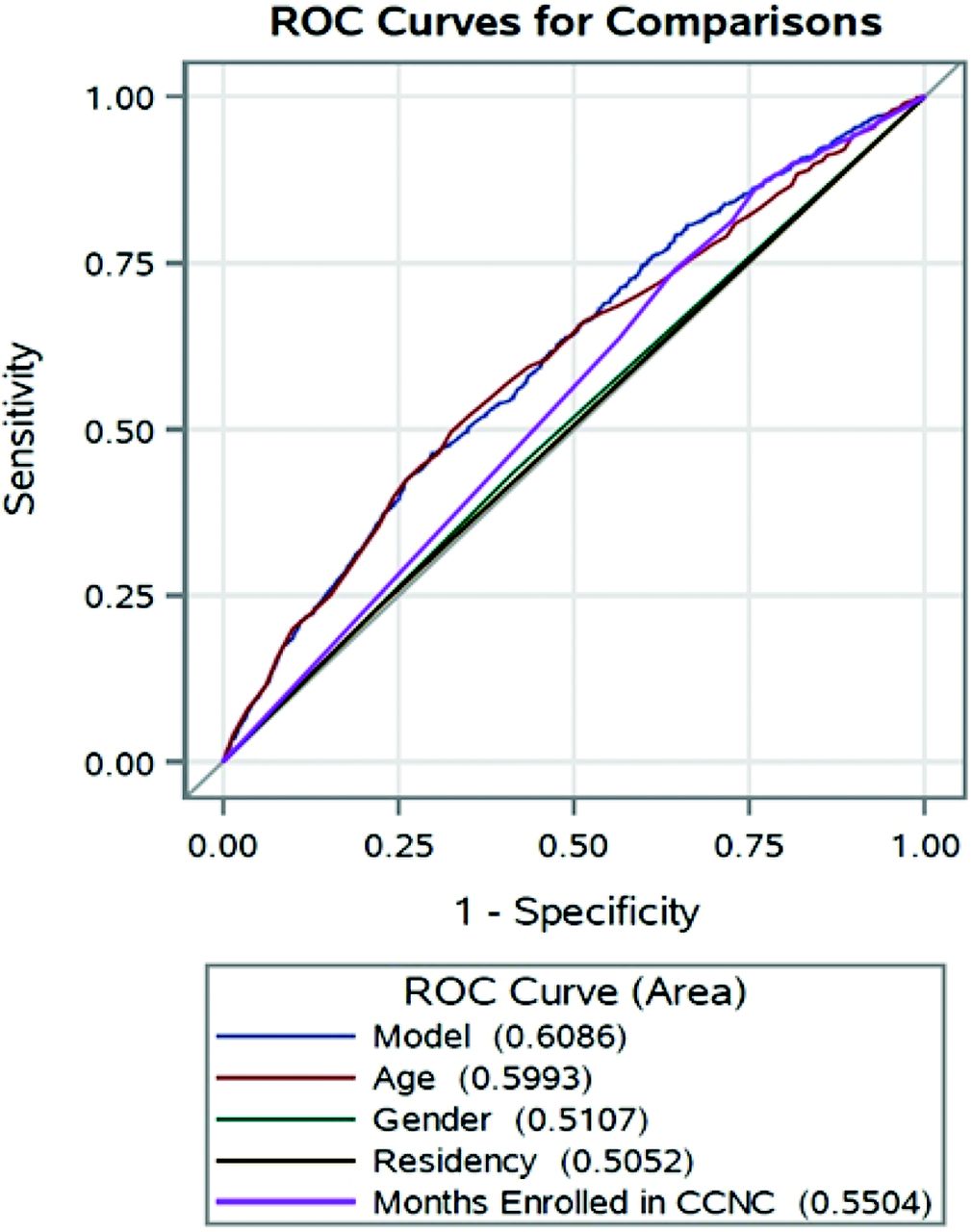
Area under the curve–receiver operating characteristics (AUC-ROC) curve for comanagement. Performance of predictor measures and a combined model including age, gender, residency, and months enrolled in Community Care of North Carolina (CCNC) for comanagement with area under the curve values for each.
HU Utilization
A third of the sample (32.24%) had at least 1 HU prescription during the study period (Table 4). Those who were 1 to 9 years old had the highest median number of days supplied (221; range, 21 to 750), the least median days between breaks in HU treatment (14.21; range, 0 to 318), and the longest duration of HU treatment days (median, 340; range, 0 to 364). Those who were 18 to 30 years old had the lowest number of median days supplied (110; range, 4 to 366) and the most median days between treatment (49.3; range, 0 to 337). The 1-to-9-year-olds also had the highest number of patients classified as good HU adherence (47.50%) and conversely the lowest classified as poor HU adherence (37.50%). In contrast, the 18-to-30-year-old age group had the lowest good HU adherence (18.03%) and the highest poor HU adherence (69.40%) in the sample. The 31-to-45 year-old age groups had the next lowest good HU adherence (20.93%) and next highest poor HU adherence (60.47%). Age was the strongest predictive factor of good HU adherence (AUC = 0.6503). Prediction by comanagement was minimal with an AUC = 0.5615, but it was greater than the prediction of primary care only (AUC = 0.5481) or hematology care only (AUC = 0.5481) (Figure 2). Gender, residency, and number of months enrolled in CCNC had little influence on HU adherence.
Hydroxyurea (HU) Prescription (Rx) Fills and Adherence for North Carolina Medicaid Enrolled at least 12-monthnths Age 1 to 64 (N = 2013)
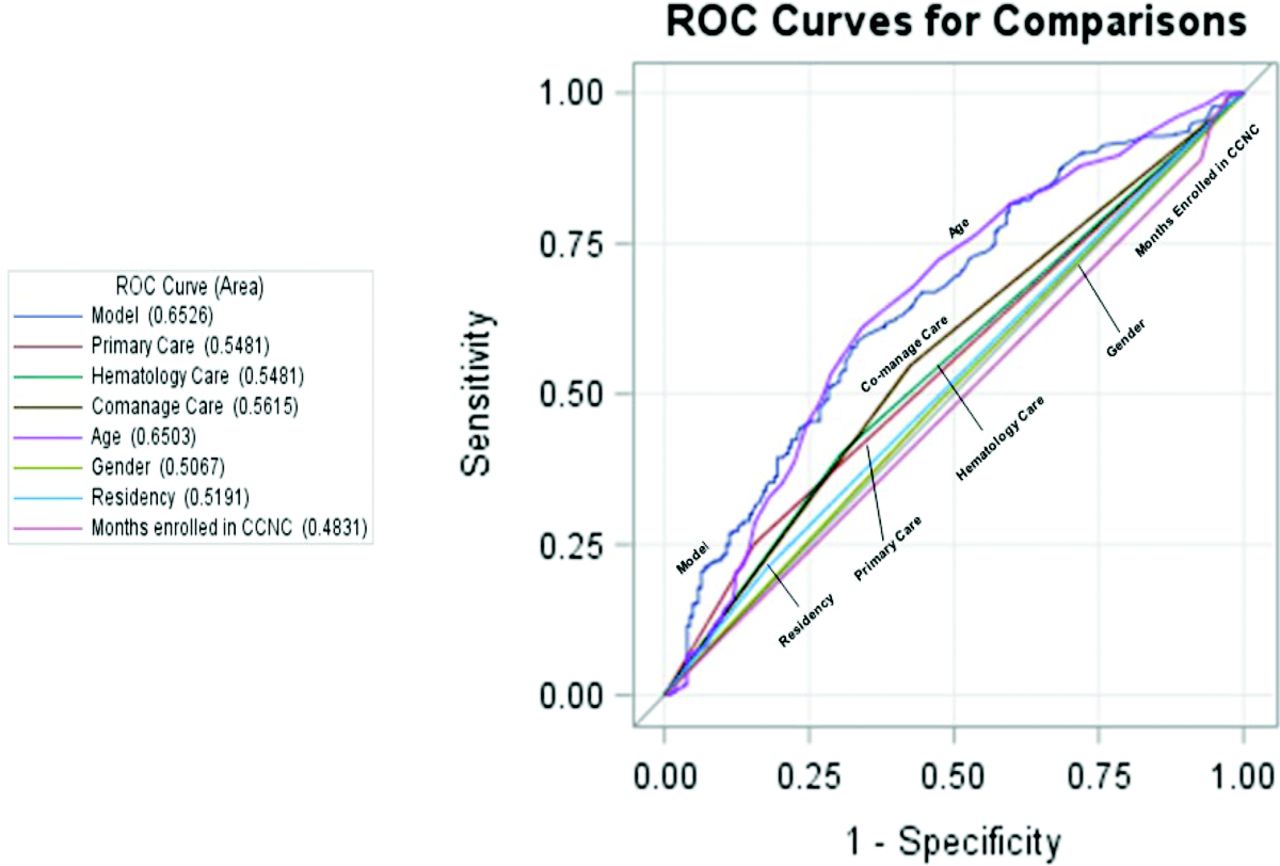
Performance of predictor measures and a combined model including Primary Care visit alone, Hematology visit alone, Co-management, age, gender, residency and months enrolled in Community Care of North Carolina (CCNC) for good versus fair or poor hydroxyurea adherence with area under the curve values for each.
Discussion
Our study revealed high health service utilization and low rates of HU adherence, which are consistent with prior studies of SCD health care utilization.16,25,35⇓⇓–38 We also found, however, a strikingly low rate of comanagement between the PCP and SCD specialist, simply defined as 1 visit to both a PCP and hematologist. Furthermore, we noted high utilization of additional services by nonhematologist specialist and significant variations in HU adherence by age group.
ED Encounters and Hospitalization
Prior national assessments of ED encounters in 1 year were estimated to be 232,381 and primarily by adult patients (81% by adults, 19% by those <18 years).2 Similarly, our sample revealed 18-to-30-year-old and 31-to-45-year-old age groups had the highest rate of ED encounters, with close to three quarters of those age groups having at least 1 ED encounter. This rate was lower than prior rates of up to 90% reported by Brousseau et al4 In the <18-year-old group, our sample had a lower ED encounter rate (65.88%) compared with the national estimate of 67%.38 In addition, previous studies have highlighted the highest EDR among the patients transitioning from pediatrics to adult medical care with an associated high health care cost.39 Our sample also highlighted poor transition to adult medical care with a significant percentage of 18-to-30-year-old patients (44.69% of the sample) having greater than 0.33 EDR, which indicates a high reliance on the ED.17
Patients with SCD are frequently admitted to the hospital for further pain control after initially being seen in the ED, supported by our findings that almost half of our sample were hospitalized during the study period. Furthermore, SCD has a higher rehospitalization rate than other chronic diseases such as heart failure and diabetes and rehospitalization is a measure of quality of care related to hospitalization.40 A significant contributor to health care costs in the chronically ill is 30-day rehospitalization rates, which may reflect the lack of access and quality of ambulatory care for patients with SCD.2,37,41,42 We found 7-, 14-, and 30-day rehospitalization rates were lower than prior findings (5% to 16%).2,40 These lower rates may be due to state-based efforts by CCNC to reduce hospital admissions and readmissions, variations in access to care and insurance benefits by state and previous studies performing analysis on data over a decade ago. Risk factors for rehospitalizations such as age, (particularly the age at transition from pediatric to adult care) and having public health insurance have been previously identified.43 Our study supports prior findings indicating a spike in utilization that coincides with the age of transition from pediatric to adult SCD care and high utilization in a sample of NC Medicaid enrollees. Moreover, it indicates a continued need to develop interventions for SCD patients and providers that will improve care throughout the care transition period in this population. Finally, a lack of follow-up care with the PCP or hematologist has also been consistently reported as an important factor associated with rehospitalizations and return to the ED within 30 days of discharge.35,37,40,43,44
Outpatient Visits
In addition to evaluating PCP visits and hematology visits, our study included data on the number of outpatient visits with various specialists. We found a large number of nonhematology specialty visits, many by PAs and NPs, and age-related differences in the types of outpatient services utilized. To the best of our knowledge, we are the first group to report this level of complex outpatient care and the use of multiple specialty services by SCD patients. This important finding has implications for care coordination. Use of patient navigators may be 1 intervention to assist patients with the high number of specialists and associated appointments required to manage SCD.45 Two projects funded by Patient Centered Outcomes Research Institute (PCORI) are currently evaluating the use of community health workers and peer mentoring to improve the transition period for emerging adults with SCD.46,47 These projects hope to generate evidence that will support the routine use of some type of support systems necessary to navigate the complex health care needs for individuals with SCD.
There was little difference between the percentages of enrollees that had a PCP visit and a nonhematology specialist, although the total and mean number nonhematology specialist visits exceeded the total and mean number of PCP visits. This demonstrates the wide variety and high frequency of specialty care requirements for this population. The 1-to-17-year-old sample age groups had similar total outpatient visit rates to the 18+-year age groups. Prior studies have reported a higher number of mean outpatient visits (12.6 vs 7.9 in our sample) for Medicaid-enrolled children.48 However, there was a downward trend in the rate of hematology specialists visits in older SCD age groups. This trend was reversed in the nonhematology specialist visits, which were lowest in the youngest age group and highest in the oldest age group. Studies of SCD patients have previously shown that the absence of a PCP and missing or forgetting outpatient visits were associated with both hospitalizations and rehospitalizations of SCD patients.35,37 The effect of nonhematologist specialty visits on ED or inpatient health service utilization, in contrast, has not been reported. Information on the type of services provided by nonhematology specialists and the mechanisms (eg, referral processes) used by patients to access these services are needed. Service delivery may be influenced by restrictions in advanced practice provider practice, which vary by state. Patterns of outpatient specialist utilization are needed. This includes nonhematology specialists visits, before ED and hospitalizations for common complaints such as pain, as this is the most common reason for SCD patient hospitalization, is complex and difficult to manage.35,36,49,50 These findings support the need for alternative care models. However, models such as the patient- centered medical home (PCMH) care model have been difficult to implement and for patients to access.7,51 A recent national survey of 1060 family practice physicians, found that only 20% reported being comfortable with overall management of SCD.13 However, 80% of respondents indicated they would be willing to comanage pediatric patients, and 68% reported they would be willing to comanage adult patients.13
Comanagement
It has been previously identified that there is a need to improve comanagement between specialists and PCPs for chronic diseases. In a large survey of 702 primary care practices, only 27% of primary care patients with chronic diseases were comanaged, despite evidence that comanagement can improve care of chronically ill patients.52 For example, comanagement by nephrologists and PCPs has been found to improve the PCP's ability to identify chronic kidney disease, referral to nephrologists, execution of comanagement plans, and improved monitoring of anemia and metabolic bone disease.53,54 Comanagement between rheumatology and primary care has also been suggested to improve management of patients with rheumatoid arthritis and cardiovascular disease.55 Our sample rate of comanagement was 34.82%, but varied by age group. Comanagement was lower in the 18-and-older age groups and age also contributed the most to our comanagement prediction model. This finding, along with the high number of nonhematology specialist visits in adults suggest a need to promote comanagement of SCD patients to a wider group of providers including PAs, NPs and other specialists such as obstetrician/gynecologists that have not been considered part of usual care for SCD patients. Similar to other chronic diseases, a comanagement model using a combination of a PCP and a hematology specialist to manage the care of SCD patients could potentially improve SCD quality of care by reducing disease complications and high acute care utilization. For example, comanagement models of care could specifically focus on increasing the rate of prescription and use of HU, which is often under prescribed and the mainstay of therapy for SCD.
HU Prescription Fills and Adherence
HU has been shown to reduce the frequency of pain episodes, acute chest syndrome, need for red blood cell transfusions, hospitalizations, and mortality.10,56 Reported HU adherence rates vary widely depending on the assessment method used and the sample size.57⇓⇓–60 Although there is no perfect measurement of adherence, HU pharmacy refills have been used to identify SCD patients at risk for poor response due to nonadherence.60 Using Medicaid HU prescription claims, we found only a third of patients were classified as having good HU adherence, which was similar to the rate reported in a prior study (35%) of NC Medicaid enrollees, using prescription claims data to obtain medication possession ratio as a measure of adherence.20 Factors leading to poor adherence include patient negative perceptions about benefits of HU, adverse symptoms, and poor emotional response to SCD.56,61,62 Age has been shown to have a significant effect on HU adherence, with older age being associated with poorer adherence.57 We found a similar trend, with increasing age and decreasing number of participants with a filled HU prescription, the number of HU prescriptions filled, number of days supplied, and adherence. HU adherence in the 65+-year age group was excluded from our analysis because they had no HU prescription fills. Age was more highly associated with good versus fair or poor HU adherence than the proposed statistical model. However, comanagement was associated with HU adherence, despite low overall rates of comanagement in our sample. This finding warrants further analysis of the relationship of comanagement to HU adherence, which may in turn influence ED and inpatient utilization.
Study Limitations
There were several limitations of our study. Our study only included Medicaid enrollees with SCD, a group that has been found to have higher rates of health service utilization in several other studies.2,4,36,63⇓–65 Only Medicaid claims from 2016 to 2017, after the initiation of the Patient Protection and Affordable Care Act (ACA) were used in our study. Although NC did not expand Medicaid coverage, studies on ED and outpatient health service utilization after the ACA went into effect have varied greatly between states.66⇓–68 Variations in utilization may also result from between state differences in the number of new Medicaid enrollees, coverage limits and the number of years since expansion occurred. Future comparisons of health service utilization that considers these payer differences (Medicaid expanded and not expanded) by state would provide a more robust understanding of utilization in the SCD population.
Differences in the number of SCD-related ED visits have been noted depending on the volume and proximity of the ED to metropolitan areas.2 Our data did not include the location of the ED where the encounter occurred, so this level of analysis was excluded from our study. In addition, the study observation period was shorter, (12 months) in our study compared with other studies that have included more than 2 years of utilization data.2,4,63,69 The episodic nature of SCD, including intermittent periods of very high service utilization followed by periods of lower service utilization may have led to over- or under-representation of data during our 12-month study period. We were also unable to classify claims with no rendering provider information. These claims were categorized into an unidentifiable (null) category, but likely caused an underrepresentation of another nonhematology specialist category. We were also unable to determine the practice type of PAs and NPs, specifically whether they were SCD specialists or primary care. In addition, we were unable to review medical records to describe the type of comanagement that occurred between the specialist and PCP, the type of care provided by the PCPs, or “who” prescribed HU. This article reports our baseline data, before dissemination of the NHLBI evidence based guidelines and we cannot yet comment on how they will affect practice.
Conclusion
In our study, age was the most important factor in predicting comanagement and HU adherence and there were notable age-related differences in health care utilization. As in prior studies, the age at which ED and inpatient use increases, coincides with the period of transition from pediatric to adult care.16,26,70 Increased utilization from acute care services has been described in several studies of pediatric to adult care transition.11,22 Our study further supports the need for increased focus on acute care utilization in the 18-to-45-year-old age group and considerations for improved care transition interventions.71 Interventions that improve HU adherence are of particular importance in reducing acute care utilization. Importantly, we found comanagement is associated with HU adherence. Further studies of the influence of comanagement on known drivers of high SCD acute care utilization such as acute pain episodes are needed, as well as studies that identify the frequency and components of comanagement needed to increase adherence and reduce acute care utilization. While we were able to report preliminary data on outpatient utilization including utilization of nonhematology specialist, we did not report specifics such as procedures or the chief complaint associated with these visit (eg, pain related) or include nonhematology specialist utilization in our comanagement or HU adherence models. Future research that considers nonhematology specialist in understanding of SCD health service utilization is also needed.
Notes
This article was externally peer reviewed.
Funding: Supported by National Heart, Lung and Blood Institute (R18 RHS024501A).
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/33/1/91.full.
- Received for publication April 18, 2019.
- Revision received August 21, 2019.
- Accepted for publication August 25, 2019.




{kind=link}
{kind=link}