
Abstract
Background: The role of family physicians (FPs) and college health professionals (CHPs) in stimulant treatment and nonmedical use of stimulants is not clear.
Objective: To investigate the current practices, concerns, needs, beliefs, barriers, and facilitators to appropriate pharmacological treatment of teens and young adults with attention deficit hyperactivity disorder (ADHD) and prevention of nonmedical use and diversion.
Methods: A cross-sectional survey developed by the project team and experts in the field, delivered to national sample of FPs and CHPs.
Results: A total of 794 completed surveys were analyzed. The average age of respondents was 51.6 ± 10.3 years; 50.6% of the respondents were female. The majority of CHPs (80.6%) reported they spend 75% to 100% of their time with patients age 17 to 24 years and 74.0% of FPs reported they spend less than 25% of their time with this age group. The majority (91.7%) of the respondents indicated that untreated ADHD affects quality of life, and 76.4% indicated untreated ADHD is often associated with risky behaviors. More CHPs than FPs always refer out for ADHD diagnosis (70.7% vs 52.1%; P < .001). Most respondents (81.2%) were concerned with ADHD medication diversion, and 84.2% believed that diversion or abuse is a problem overall. Respondents indicated they are unprepared to provide patient education on decisions about pharmacotherapy or behavioral therapy choices for adult ADHD.
Conclusion: There is an opportunity to enhance safety and effectiveness of ADHD management in young adults. Additional resources and interventions are needed to improve medication management, reduce misuse, and ensure safe and appropriate use of stimulants.
- Adolescent
- Attention Deficit Hyperactivity Disorder
- Central Nervous System Stimulants
- Cross-Sectional Studies
- Family Physicians
- Patient Safety
- Quality of Life
- Surveys and Questionnaires
- Universities
- Young Adult
Attention deficit hyperactivity disorder (ADHD) is a common neurodevelopmental disorder affecting about 3% to 10% of school-aged children and adolescents.1⇓–3 Nearly half of the children and adolescents with ADHD continue to have symptoms of the disorder in adulthood.4,5 Stimulants are the most common medications prescribed for ADHD, and pharmacological treatment has shown a positive impact on outcomes, long-term prognosis, and quality of life in children and adults with a diagnosis of ADHD. One important consideration related to stimulant medications is the appropriate use of these medications and their potential for abuse. Recent research has documented that the nonmedical use of prescription stimulants is a substantial and growing problem among young adults and college students.6⇓–8 Nonmedical use of stimulants on college campuses is a well-documented problem.9,10 Physicians have been identified as the second most frequent source of the misused stimulants.11 It is important to understand the role the health care professionals play in treating ADHD in young adults, and their potential role in prevention of nonmedical use of stimulants.
Even though ADHD patients have stimulant medications prescribed by both primary care providers and providers in college health centers, there is very little research on commonalities and differences in the way the settings manage ADHD, prescribe and monitor medications, and prevent inappropriate use of stimulants.
The objective of this article is to present methodology and results of a provider survey on the current care practices, concerns, needs, beliefs, barriers, and facilitators to appropriate pharmacological treatment, and the prevention of nonmedical use of stimulants among teens and young adults age 17 to 26 years. The survey study intended to provide descriptive data on primary care providers and providers in college health centers and was not designed to test any specific a priori hypothesis.
Methods
Study Overview
This study was a cross-sectional survey of national samples of members of American Academy of Family Physicians (AAFP) and members of the American College Health Association (ACHA). The study was approved by the AAFP Institutional Review Board (IRB).
Sample and Setting
The study was conducted with 1) a random sample of the AAFP nonretired members who reside in the United States, spend at least 50% of their time in direct patient care, and have responsibility for the care of teenagers and young adults (n = 2000; AAFP members, family physicians [FPs]); and 2) the segment of ACHA college health professionals working in student health centers (n = 573; ACHA members, college health professionals [CHPs]). At the time of the survey, the AAFP membership database included 68,300 active members working in primary care. The ACHA membership database included 2931 health care professionals working at college health centers across the United States. The ACHA target group included all registered members from all regions of the United States, from the sections of Advanced Practice Clinicians, Clinical Medicine, Nurse-Directed Health Services, and Nursing. The makeup of the final ACHA sample included 91 physicians, 369 nursing professionals, 24 other specialists (clinical psychologists, social workers), and 12 physician assistants; 77 had no identified role or credentials. Only the health professionals from these 2 samples, and not their young-adult and student patients, were invited to participate in this survey.
Survey Development
The project team developed a survey in collaboration with 3 ADHD experts (a family physician, a pediatrician, and an ADHD research expert). We followed the best practices in survey development and reporting described by Kelley et al.12 The details of the survey development and administration methodology are described in Appendix 1. Briefly, the survey was developed based on key themes derived from the literature review. The survey included the following constructs: knowledge and belief; practice; risk management; strategies, and resources. Initially, 77 survey items were developed; these were further refined into a 43-item questionnaire. We piloted the 43-item survey with 10 practicing physicians to evaluate their comprehension of the questions and answer choices. The final survey consisted of 42 items. We created 2 versions of the survey: article and online. The survey was administered between October 27, 2015, and January 31, 2016.
Statistical Analyses
After the data were cleaned for duplicates and errors and scale items were recoded for consistency, descriptive statistics (overall, AAFP members, and ACHA members) for all questions were completed. For the binary and multiple-choice questions, the data are reported as counts and percentage. For the 5-point Likert scale questions, the mean and SD was calculated for each group for each question. The lower the value of the mean, the more agreeable the statement is to the group's perceptions, feelings, or knowledge (for example, the scale 1 = Describes me completely/Always/Very likely to 5 = Does not describe me at all/Never/Very unlikely). For the analysis, 95% CIs (not shown) and t-tests comparing AAFP members and ACHA members were completed for the Likert scale questions of interest. For the yes/no and multiple-select questions of interest, χ2 tests comparing AAFP members and ACHA members were completed. An α of 0.05 was used throughout the analysis. When a statistically significant difference existed between FPs and CHPs, it is specified in the results; if no difference was identified, the data are presented for all respondents combined. All analyses were conducted with SPSS (IBM SPSS Statistics for Windows, Version 22.0., Armonk, NY). Select questions are included in the results. All responses are included in Appendix 2.
Results
Participant Characteristics
Overall, 817 participants returned surveys, including 678 AAFP members and 139 ACHA members (response rates: 33.9% and 24.3%, respectively). Several surveys were excluded from the analysis due to duplicate entries, incomplete surveys, or the respondent indicated she/he was retired, leaving the valid final sample of 794 respondents included in the analyses. Most of the surveys (n = 726; 91.4%) were completed on article and the remainder (n = 68; 8.6%) were completed online.
The average age of respondent was 51.6 ± 10.3 years, and the majority (80.0%) of respondents indicated their race/ethnicity was white (FPs: 79.0%; CHPs: 84.7%) with no differences between the groups (Table 1). Overall, slightly over half (50.6%) of the respondents were female with more female participants among CHPs (80.2% vs 44.8% among FPs, P < .01). More CHPs than FPs indicated that they are employed by a hospital, clinic, or university (82.9% vs 45.5%; P < .01). The majority of CHPs (80.6%) reported they spend 75% to 100% of their time with patients 17 to 24 years of age; 74.0% of FPs reported they spend less than 25% of their time with the patient in this age group (P < .01).
Respondent Demographic Characteristics
The sample of AAFP members in this study was largely representative of the overall AAFP membership based on gender, race, and years since residency, with the only exception of age distribution: the AAFP survey respondents were more evenly split between the 4 age categories than the overall AAFP member demographics (< 40 years old: 15.9% vs 47.1%; 40 to 49 years old: 24.3% vs 18.1%; 50 to 59 years old: 33.6% vs 15.6%; 60 years and older: 26.1% vs 19.1%). The representativeness of the ACHA respondents could not be established due to limited available data.
Knowledge and Belief
The majority (80.6%) of respondents estimated ADHD prevalence to be between 1% and 10% in adults, with more CHPs than FPs estimating a higher prevalence of ADHD in adults and college students (P < .01). Although 54.4% of participants believed that ADHD is overdiagnosed in teens and young adults, 78.6% reported it is “likely or very likely” that they have adult patients with undiagnosed ADHD in their practice. The majority (91.7%) of the respondents indicated that untreated ADHD affects quality of life, and 76.4% indicated untreated ADHD is often associated with risky behaviors. More FPs than CHPs indicated ADHD is easy to “fake” for drug-seeking patients, and it is difficult to determine when a patient is “faking” the symptoms of ADHD (66.7% vs 50.8%, P < .01; and 64.5% vs 43.1%, P < .01, respectively).
Overall, respondents agreed that stimulants have the potential for abuse (98.7%) and that stimulants are addictive (71.7%). The majority of respondents (81.2%) were concerned with ADHD medication diversion, and 84.2% believed that diversion or abuse is a problem. Almost all know the correct definition of misuse, abuse, and diversion (97.9%, 95.8%, and 95.6%, respectively). Over three fourths (83.6%) agree that the legal consequences of diversion are serious, and 81.2% agree that it is important to educate about the legal ramifications of diversion.
For FPs, the most frequent patient characteristics that are associated with abuse or diversions were history of drug use (80.8%), history of mental illness (61.1%), and male gender (49.3%). For CHPs, most frequent patient characteristics that are associated with abuse or diversions were: history of drug use (62.1%), competitive school or program (61.3%), and male gender (45.2%). The respondents believed that most patients only occasionally are engaged in nonmedical use or diversion of stimulants and much fewer patients engage very frequently. Fewer CHPs than FPs believed that their patients never or rarely engage in misuse, abuse, or diversion (8.2% vs 17.0%; 19.6% vs 25.7%; and 17.5% vs 30.0%, respectively).
Practice
In describing evaluation, diagnosis, and treatment for adult ADHD, more CHPs than FPs always refer out for diagnosis (70.7% vs 52.1%, P < .05), seek expert consultation for diagnosis and treatment (48.0% vs 19.1%, P < .05), never initiate drug therapy (42.2% vs 15.1%, P < .05), and never use a stimulant as their first choice for ADHD treatment (37.6% vs 13.1%, P < .05). More than one third of respondents reported that they never follow medication treatment recommendations (38.6%), and more than half always discuss effects and side effects of stimulants with patients (54.0%). See Table 2.
Analysis Results of Likert Scale Questions
More FPs than CHPs reported they felt comfortable prescribing stimulants (3.17 ± 1.20 vs 3.64 ± 1.37, P < .05), tended to try medication even when uncertain (4.51 ± 0.77 vs 4.79 ± 0.50, P < .05), and believed treatment should be withdrawn if side effects emerge (2.72 ± 1.12 vs 3.42 ± 1.20, P = .05). More FPs than CHPs were not concerned with suicidal ideation or depression when prescribing stimulants (4.5 ± 0.9 vs 4.77 ± 0.7, P < .05). About a quarter of FPs (23.0% vs 11.5% of CHPs) believed “medication holidays” were acceptable, with the differences in FPs' responses compared with CHPs' (2.5 ± 1.23 vs 3.3 ± 1.38, P < .05; see Table 2).
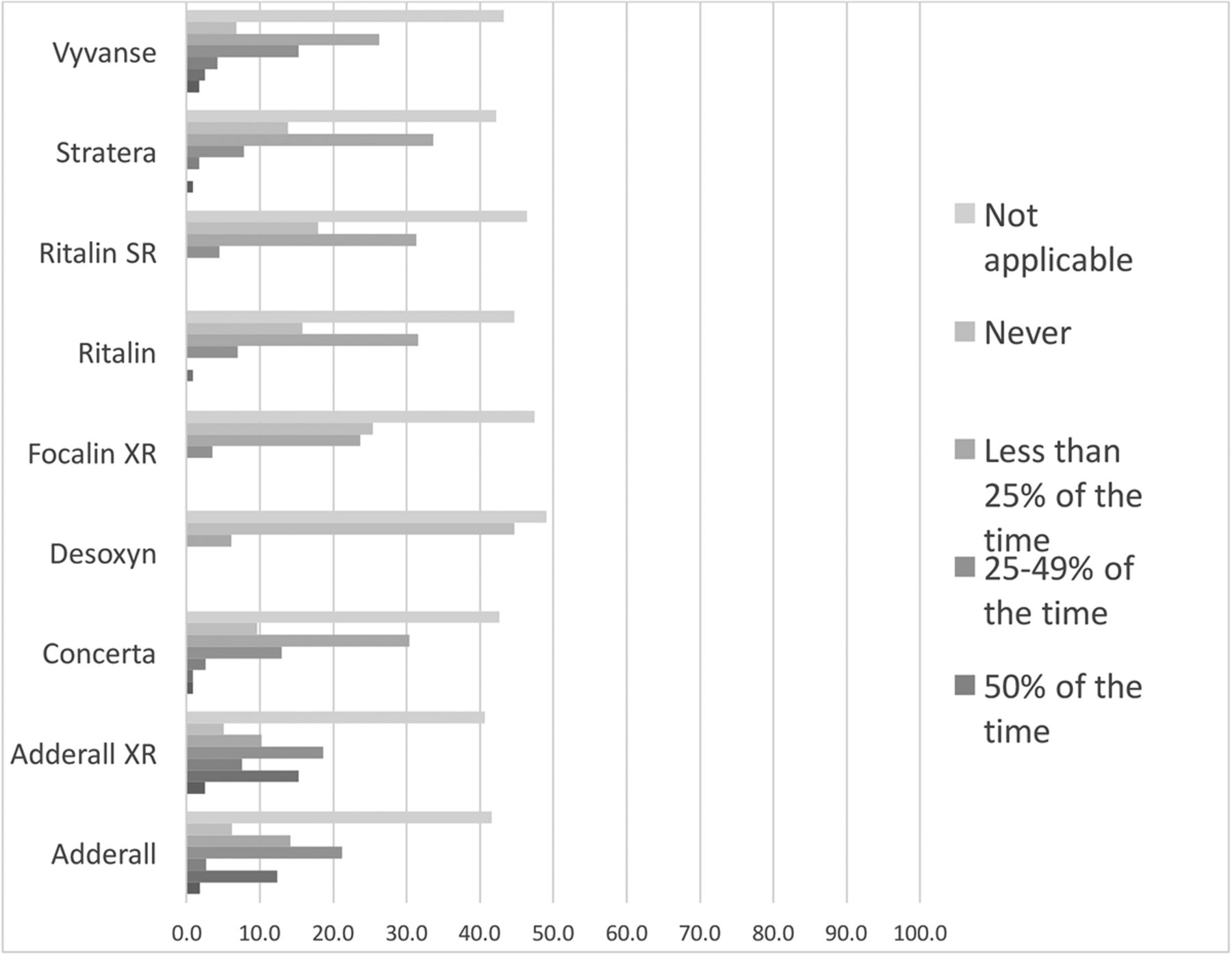
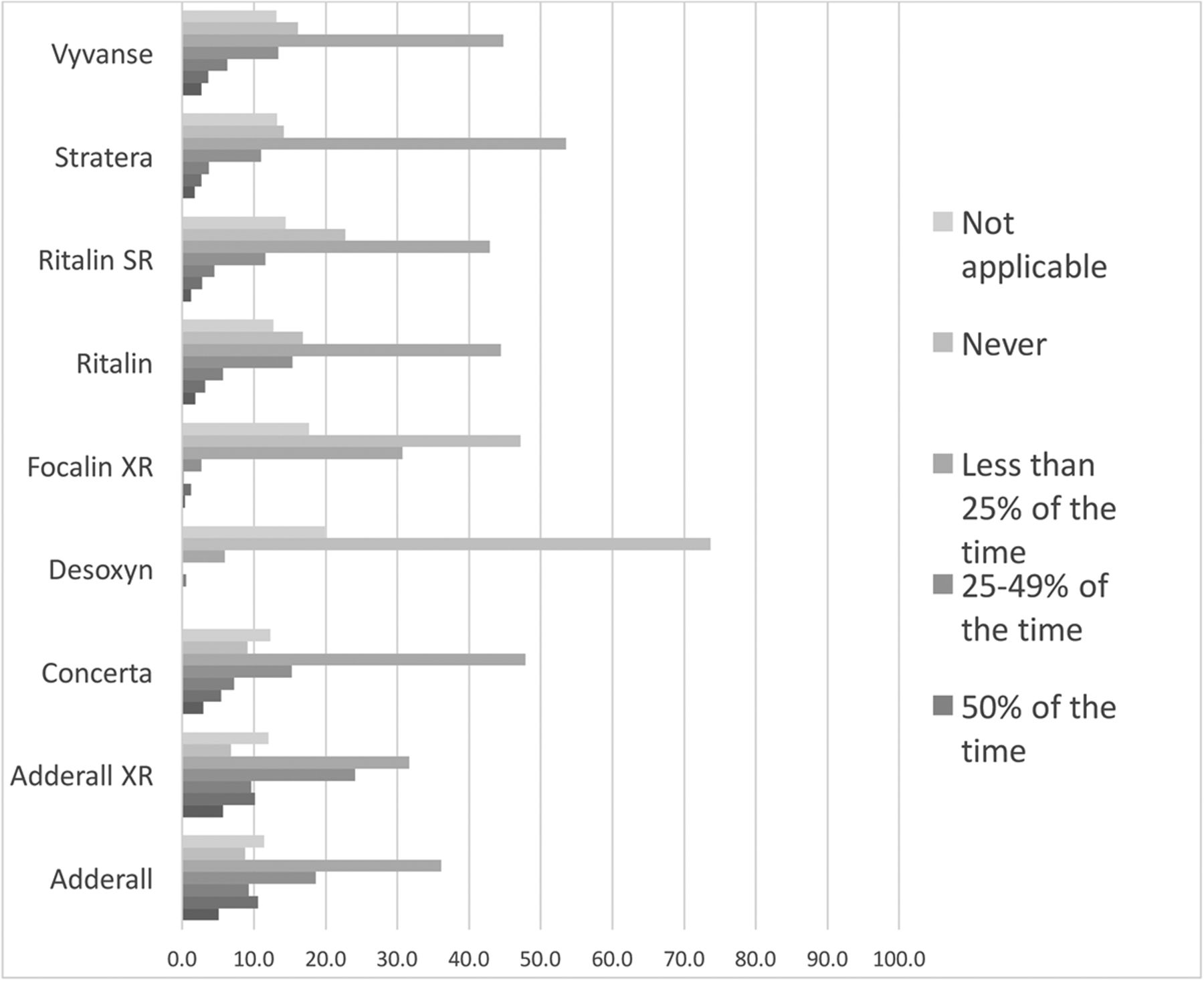
When asked about specific stimulant medications approved for treatment of ADHD in adults, for 9 medications (brand names) included in the survey, CHPs selected “not applicable” more frequently than FPs (44.2% vs 14.1%, P < .05). Top 2 medications prescribed by most FPs (Figure 1) versus most CHPs (Figure 2) more than 50% of the time were Adderall XR and Adderall (25% and 25% vs 25% and 16.9% respectively). Among FPs and CHPs, the most frequent factors associated with prescribing a certain medication were: previous success with the same medicine (75.2% vs 49.6%), comfort with medicine (74.4% vs 43.0%), insurance coverage or coverage restrictions (72.8% vs 42.1%), and cost of medication (62.7% vs 39.7%). More CHPs than FPs selected evidence-based guidelines (36.6% vs 31.8%) as 1 of the factors associated with prescribing a certain medication. More FPs than CHPs selected own experience (40.4% vs 20.7%) and patient preferences as important factors (36.8% vs 19.8%).

FPs' frequency in prescribing ADHD medications. Abbreviations: FPs, family physicians; ADHD, attention deficit hyperactivity disorder.
CHPs' frequency in prescribing ADHD medications. Abbreviations: CHPs, college health professionals; ADHD, attention deficit hyperactivity disorder.
Risk Management
When asked specifically about misuse and diversion risk management in college students, CHPs more often than FPs would ask about a patient's other substance use (1.86 ± 1.1 vs 2.16 ± 1.1; P < .05) and suggest available resources to their ADHD patients (2.04 ± 1.2 vs 2.55 ± 1.2; P < .05). In monitoring their patients' medication compliance, more FPs than CHPs indicated that they use a state medication registry (62.1% vs 40.2%, P < .05), random drug testing (42.3% vs 21.3% P < .05), and pill counts (18.6% vs 9.8%, P < .05, see Table 3).
Analysis Results of Binary Scale Questions
Most participants indicated that they feel responsible for educating patients with ADHD, with more FPs than CHPs agreeing with this responsibility (95.1% vs 90.4%; P = .04). The majority of participants agreed that they are responsible for educating about the legal, health, social, and physical risks of misuse and the mental effects of not using the medicine properly (see Table 3).
Strategies and Resources
Both FPs and CHPs indicated that the best way to educate patients was through education or counseling at the visits where the prescription was given (83.8%). More CHPs than FPs (16.1% vs 6.4%; P < .01) indicated social media was a way to educate patients about ADHD (see Table 3).
When asked about which aspects of patient education the respondents are more or less comfortable in providing, some FPs and CHPs reported they were well equipped to handle patient education on the nature of ADHD, effects and side effects of stimulants, and decisions about therapy choices. Compared with FPs, more CHPs indicated they are equipped to provide patient education on general expectations for college life and on risky behaviors, drug abuse, medication misuse, and prevention strategies (see Table 2). However, there were areas where the majority of FPs and CHPs feel they are somewhat unprepared to not prepared at all. For FPs, the majority indicated they are unprepared in the areas of:
Decisions about pharmacotherapy or behavioral therapy choices (52.9%)
Risky behaviors, drug abuse, medication misuse, and prevention strategies (52.4%)
Nature of ADHD (50.7%).
For CHPs, the majority indicated they are unprepared in the areas of:
Decisions about pharmacotherapy or behavioral therapy choices (59.5%)
Nature of ADHD (58.9%)
Effects and side effects of stimulant medications (50.4%).
When asked about provider education strategies, FPs and CHPs indicated that Continuing Medical Education (CME)/conferences (93.2%), journal articles (73.7%), other physicians/peer groups (58.7%), and professional associations (56.3%) would all have the potential to impact physicians' views on misuse prevention. Over one quarter of all respondents (27.0%) indicated that media (TV, Internet) may also influence physicians' views on abuse, misuse, and diversions issues.
Discussion
FPs and CHPs play an important role in the management of teens and young adults with ADHD and stimulant prescribing.13,14 Several qualitative studies reported on physicians' challenges related to adult ADHD diagnosis, management, and treatment, and some explored issues related to misuse, abuse, and diversion.15⇓–17 To our knowledge, this is the first US national and systematic description of FPs' and CHPs' self-reported perceptions and practice patterns focusing on pharmacological treatment and prevention of nonmedical use and diversion of stimulants among teens and young adults. This article presents and discusses the survey results and highlights selected findings and their implications while also presenting the detailed report of all collected data for further interpretations. The most significant key findings are highlighted below.
Similar to previous studies, we found that an overwhelming majority of surveyed FPs and CHPs whose patient populations include teens, young adults, and college students agree that untreated ADHD negatively affects quality of life.3,18,19 However, many FPs and CHPs in our study believe that some of their patients may have undiagnosed and untreated ADHD. These results suggest a continued need to support appropriate identification of untreated ADHD among adults and young adults. Effective detection of ADHD in adults needs to consider reported difficulties among many providers with identifying patients with ADHD who actually have symptoms and would benefit from treatment from those who may “fake” the symptoms to gain access to stimulants for nonmedical use.20,21 This difficulty expressed by the clinicians may be due to generally low to moderate levels of competence and comfort of primary care practitioners with assessment and diagnosis of ADHD in teens and adults.22⇓–24 Many participants reported they always refer out for diagnosis and seek expert consultation for treatment.
Most participants agree that diversion or abuse of stimulant medications is a problem and feel responsible for educating patients about legal, health, and physical risks of stimulant use and misuse. While half of participants believed that patients occasionally engaged in abuse, diversion and misuse of stimulants, FPs reported believing their patients engaged less frequently in nonmedical use than what CHPs believed. Unlike FPs, significantly more CHPs believe that patients with ADHD frequently or very frequently divert their medications by giving them to friends or selling them. Recent studies show that around 70% of college students who have a prescription for stimulants diverted medication at least once in their lifetime, mostly via sharing.25,26 Similar patterns have been reported for misuse; while most students do use their ADHD medication as prescribed, misuse and diversion is not uncommon.27 Even though only a very small percentage of prescription holders engages in frequent diversion, abuse, or misuse of their medications, nonmedical use-related behaviors should be identified, and prevention efforts aimed at reducing these behaviors should be considered.
The results of our study point to some potential areas where future initiatives for quality improvement, research, and education can be considered. For example, in describing their practices, only half of participants reported always discussing medication effects and side effects with their patients, and many do not feel well prepared in discussing all treatment options with the patients. Not many prescribers use drug compliance monitoring strategies such as state medical registries, urine drug tests, and pill counts. These observations provide an opportunity to support providers with tools and resources on responsible patient education, shared decision making, and risk reduction.
Overall, FPs and CHPs were similar in many aspects related to evaluation and management of ADHD. Noticeable differences were identified, however, with the FPs reporting using stimulants as first choice and feeling confident with stimulant prescribing more often than CHPs. It is important to note that while many CHPs see patients with ADHD, the majority reported that they do not prescribe stimulants or initiate any drug therapy for ADHD. Even though we have not explored the actual reasons in the survey, this may be due to limited prescription privileges to psychologists and other health professionals on campus. This finding highlights the need for further explorations and programs to support transition of care across services for young adults with ADHD via either accessible referral resources or alternative care transition models to address potential discontinuity of mental health care and gaps in treatment.28
Our results are consistent with other studies that identified physicians' low level of confidence in medication management of ADHD with high level of concerns about stimulant medications.29 Although more FPs than CHPs felt comfortable with prescribing stimulants, many FPs reported they prescribe based on their own success and comfort with medications and their own clinical judgment rather than evidence-based guidelines. These findings are not surprising, as there are no evidence-based primary care–focused US-specific treatment algorithms and practice guidelines for adult ADHD in the US. Moreover, only one third of prescribers reported they consider patient preferences when deciding on which medication to use. This points to the need to establish evidence-based practice guidelines and shared decision making guides that account for the balance of harms and benefits of all available treatment options.
In addition, due to the lack of treatment standards and adult ADHD quality metrics, the reported practices and resulting quality of care are difficult to assess.30 For instance, some of the reported practices are not supported by sufficient level of evidence. For example, “medication holidays” were approved/encouraged by the substantial number of the providers in our study, though there is a paucity of research on the benefits and potentials risks of “medication holidays” among adults.31
Overall, FPs and CHPs are concerned with stimulant abuse, misuse, and diversion, and would benefit from additional information, education, and practice support through Continuing Medical Education (CME) opportunities, journal publications, conferences, and professional associations. The results of this study suggest that education, research, quality improvement, and prevention initiatives need to continue to focus on nonmedical use reduction to ensure safe and appropriate use of stimulants among young adults.
This study has some limitations that may affect the generalizability of results. The sociodemographic and practice characteristics of the FPs sample are comparable to the AAFP membership. However, it is not possible to generalize these results to FPs who are not AAFP members or the CHPs who did not participate in the survey. Furthermore, our study only involved family practice physicians and college health professionals. Pediatricians and other physician specialties involved in treating teenagers and young adults of college age with ADHD were not included. Despite the relatively high response rate for physicians, there might still be a response bias; the physicians with higher interest in mental health might have chosen to participate, hence their statements possibly may not be reflective of those who have low interest in mental health and ADHD, in particular.
This study was based on clinicians' self reports and did not evaluate knowledge and clinical behavior by objective measures. The relationship between opinions/attitudes and clinical behavior is controversial.32,33 To that end, we do not know to what extent the self-reported practices correlate with the objective measures of clinicians' performance or quality of care, whether the occasional diversion or misuse of stimulant medications among young adults are viewed by physicians as benign, and what actions, if any, the clinicians actually choose when providing care to their actual patients. In addition, we did not guide our participants to think of specific patients or situations when answering questions and were limited in our ability to explore in depth factors that may have influenced the responses, including those related to the local ecosystems and infrastructure, the prescribing privileges, prioritizing treatment selection for specific subgroups of patients, local policies and mandates, and other factors related to participant's specific settings.
Finally, there are very few published reliable instruments assessing FPs' and CHPs' opinions, knowledge, and attitudes about ADHD and nonmedical use of stimulants. The survey instrument was developed and subsequently tested by the project team to include a limited number of questions related to only 4 constructs and to assure item relevance and comprehension. We did not evaluate the reliability and the validity of the survey instrument.
Conclusion
The results of this survey are an important step toward documenting knowledge on topics related to ADHD pharmacotherapy and nonmedical use of stimulants in young adults in family medicine and college health clinics. Additional resources and interventions are needed to address identified gaps for quality improvement related to medication management, misuse reduction, and interprofessional collaborations and continuation of care to ensure safe and appropriate use of stimulants. The result of this project will lead to better understanding of what strategies need to be implemented to improve ADHD care and to prevent and reduce issues related to inappropriate use of stimulants.
Acknowledgments
The authors thank all participants of this project. We would like to acknowledge the AAFP National Research Network for providing essential expertise, staff, and support.
Appendix
Detailed Survey Development and Administration Methodology
Construct Development (Key Issues)
The project team developed a survey with collaboration with 3 experts in treating ADHD (a family physician, a pediatrician, and an ADHD research expert). The survey was developed based on key themes derived from the literature review data (See below for search criteria). The literature review was conducted in March-June, 2015, and resulted in 668 initial articles. The research team assessed the article titles and abstracts for eligibility, and reviewed full texts of 36 to inform the contents of the survey. The articles were eligible if they included survey methodology and survey results on a topic of ADHD and medical and nonmedical use of stimulants. The reporting of results of the literature review is beyond the scope of this work. The survey included the following constructs: knowledge and belief; practice; risk management; strategies and resources.
Search Terms
(“attention deficit disorder with hyperactivity”[MeSH Terms] OR “attention deficit disorder with hyperactivity”[All Fields] OR “adhd”[All Fields] OR “Attention Deficit and Disruptive Behavior Disorders”[MeSH Terms] OR “Attention Deficit and Disruptive Behavior Disorders”[All Fields]) AND (“treatment”[All Fields] OR “guidelines”[All Fields] OR “treatment guidelines”[All Fields] OR “recommendation”[All Fields] OR “best practice”[All Fields] OR “current practice”[All Fields] OR “clinical decision algorithm”[All Fields]) AND “adult”[MeSH Terms] AND “2009/10/09”[PDAT] : “2014/10/07”[PDAT] AND English[lang].
Draft Survey Questions
Survey items under each construct were developed based on existing items extracted from the literature review and from information derived from an expert panel. The process resulted in 77 survey items plus a demographics section; these were further refined into a 43-item questionnaire.
Pilot and Refine the Questionnaire
We piloted the 43-item survey with 10 practicing physicians to evaluate their comprehension of the questions and answer choices. The pilot group also rated the quality of each question on a 5-point scale (excellent, very good, good, fair and poor) and provided suggestions for improvement. After revisions, the final survey consisted of 42 items including 9 items collecting respondents' demographic information and 1 open-ended question that asks respondents to share any thoughts about the topic of ADHD or stimulant misuse, abuse, or diversion among young adults.
We created 2 versions of the survey: article and on-line. The survey included a header with the AAFP brand, and was formatted to be compatible with the AAFP's optical scanner (Fujitsu fi-6670), the scanning software (ScandAll Pro, Fujitsu Computer Products of America, Inc., Sunnyvale, CA), and the data entry/reading software (ReMark, Remark, Malvern, PA). We also created an on-line version of the survey using Novi Survey. The on-line survey used the same question order, though formatting varied slightly to account for user-friendly experience on-line.
Survey Administration
Each survey was coded with the study identification number. The surveys were mailed with a formal AAFP cover letter and a prepaid return envelope. A 2-dollar bill was included with each survey.
An email, with a link to the survey, was sent just before the initial mailing on October 27, 2015, to those members with email addresses. The web link was offered as an alternative to completing the article form. An email reminder was sent to nonresponders 2 weeks following the initial mailing. A second article survey was mailed to nonresponders 5 weeks from the first mailing. The survey was closed on January 31, 2016. Completed surveys were sorted and scanned and manually corrected for mis-scanned responses and hand keyed for open ended answers.
Based on Your Understanding, How Prevalent is ADHD in Adults?
Based on Your Best Understanding, How Prevalent is ADHD Among College Students?
How Likely Is it That You Have Adult Patients with Undiagnosed ADHD in Your General Practice?
Please Select to What Extent You Agree or Disagree with the Following Statements
Please Select How Often You Offer or Perform Any of the Following with the Patients with ADHD in Your Practice
Please Select to What Extent You Agree or Disagree with the Following Statements
Based on Your Best Understanding, for Each Statement Below Please Select Whether the Definition is True or False
Please Select All That Apply When Evaluating a Patient Prior to Prescribing Medical Treatment for ADHD
When You Are Following a Patient for Their ADHD Medication, How Frequently Do You See Them for Follow-Up Monitoring?
How Do You Monitor Your ADHD Patient's Medication Compliance? (Please Select All That Apply)
How Do You Evaluate Whether Your Treatment Is Working? (Please Select All That Apply)
How Frequently Do You Reassess Your Patients with ADHD if They Are:
Based on Your Best Understanding, How Frequently Do Patients Engage in Any of the Following:
Why Do You Think People Misuse ADHD Medication? (Please Select All That Apply):
Based On Your Best Understanding, Please Select the Characteristics of Patients That Predict Abuse or Diversion? (Please Select All That Apply):
Please Select How Well Each of the Following Describes You:
Please Select How Likely or Unlikely Is Each of the Following Situations:
How Often Do You Prescribe Each of the Following Medications for Teenage and Young Adult Patients with ADHD?
Which Factors Contribute to Your Decisions on Which Stimulant Medication to Use (Can Choose More Than One Answer):
How Often Do You Use Any of the Following to Monitor for Possible Medication Abuse in Your ADHD Patients:
The Following Questions Pertain to the College Students 17 to 26 Years of Age. Please Select How Well Each of the Following Statements Describes You:
What Do You Feel Is the Best Way to Educate Patients about ADHD (Please Select All That Apply):
If Yes to Question 32, What Do You Feel You Are Responsible For (Please Select All That Apply):
If No to Question 32, Who Do You Feel Is Responsible (Please Select All That Apply):
Do You Feel it Is Your Responsibility to Prevent Misuse of ADHD Medications?
What Do You Feel You Personally Should Be Doing to Reduce the Misuse of ADHD Medications (Please Select All That Apply):
How Often Do You Feel Education about ADHD or ADHD Medication Should Occur?
Do You Think it's Important to Educate About the Legal Ramifications of Diversion?
How Well Do You Feel You Are Equipped to Provide Patient Education about Each of the Following:
Does Media Coverage Have the Potential to Affect Physician Views on Misuse Prevention?
Please Select from the List What Would Have the Potential to Affect Physician Views on Misuse Prevention (Please Select All That Apply):
Notes
This article was externally peer reviewed.
Funding: This study was supported by Shire US, Inc., through the Coalition to Prevent ADHD Medication Misuse (CPAMM). Shire US, Inc. was not involved in the study design, data analysis and interpretation, or reporting of this work.
Conflict of interest: none declared.
The authors have full control of all primary data and that they agree to allow the journal to review their data if requested.
Ethical approval: All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional AAFP IRB and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
To see this article online, please go to: http://jabfm.org/content/33/1/59.full.
- Received for publication February 26, 2019.
- Revision received July 23, 2019.
- Accepted for publication July 23, 2019.




{kind=link}
{kind=link}