
Article Figures & Data
Figures
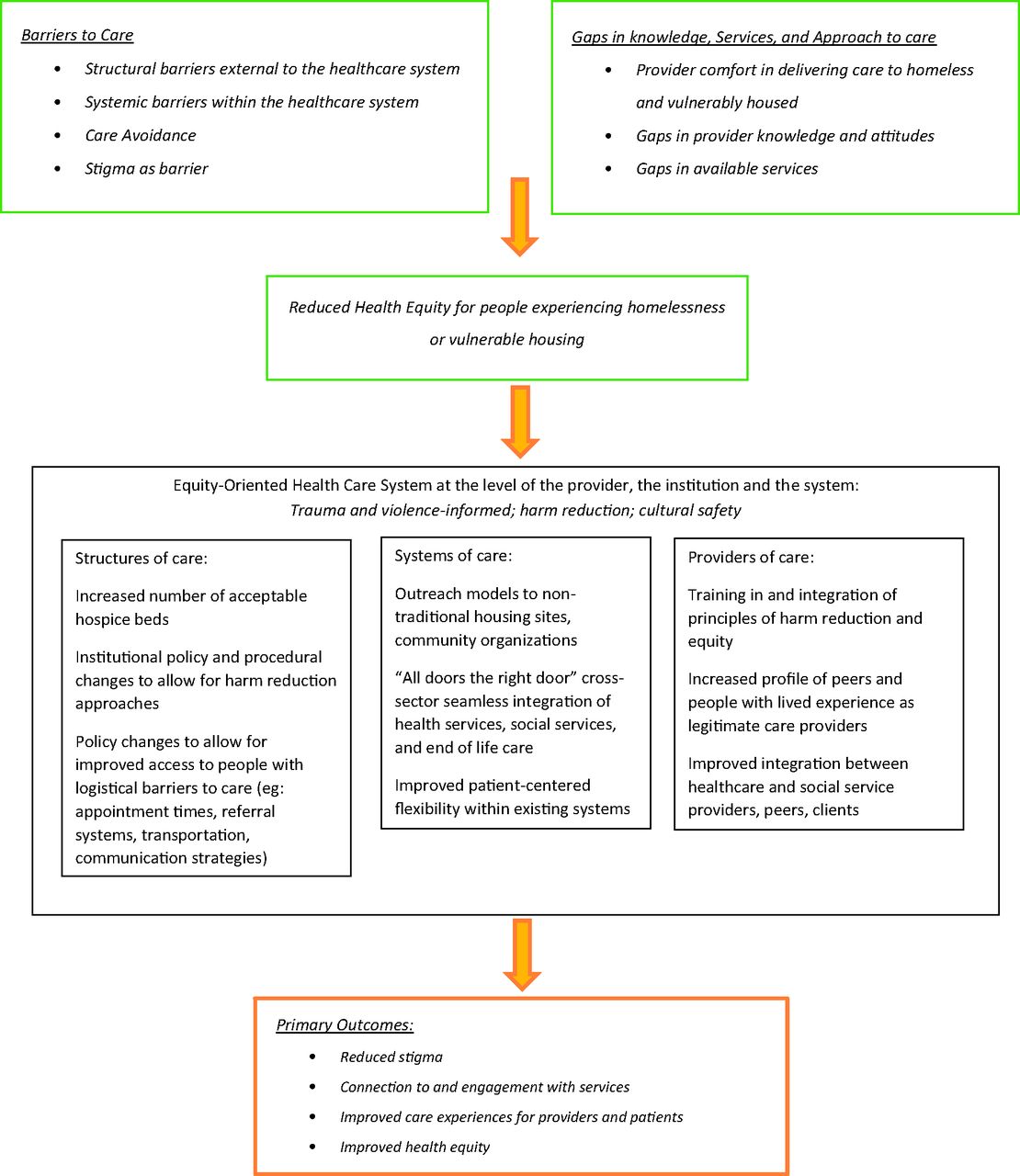
- Figure 1.
Logic model for improving end of life care for the homeless and vulnerably housed.

Tables
- Table 1.
Demographic and Organizational Characteristics with Respect to Provision of Palliative Care
Characteristics Responses, % (n = 136) Type of Community Urban 57.35 Rural 24.26 Semirural 18.38 Organizational sector (check all that apply) Health Care 74.26 Public Health 11.03 Harm reduction 20.59 Food assistance 10.29 Housing assistance 13.24 Social services 19.12 Family and child services 4.41 Community development 8.09 Populations served Homeless 74.07 Persons with substance use disorders 88.89 Indigenous people 82.22 Veterans 68.15 Other—Including living with HIV; MSM, LGBTQ2SI+, refugees, newcomers, recently released from incarceration, developmental disabilities, seniors 28.15 Frequency of personal interaction with people experiencing homelessness Never 8.15 Daily 16.30 Weekly 15.56 Monthly 14.81 Yearly 10.37 I don't know 13.33 Palliative care services available in your community Home visits 73.53 Hospital inpatient 72.79 Hospital outpatient 47.79 Residential hospice 29.41 Respite 45.59 I don't know 15.44 Other—Medical aid in dying, nursing support, equipment loan 23.53 Palliative care provided by target organization Yes 59.56 No 37.50 I don't know 2.94 Population served by palliative care services in target organization Homeless 55.56 Persons with substance use disorder 79.17 Indigenous persons 81.94 Veterans 72.22 Others—Living with HIV, seniors, recently released from incarceration 27.78 Palliative care services provided by target organizations Advanced care planning 75.00 Caregiver support 61.84 Case management/patient navigator 61.84 Emotional/psychosocial 81.57 Medical management 81.57 Spiritual support 44.74 Other—Hospitalization, primary care, bereavement support, equipment loan, physiotherapy, occupational therapy, respite care, pharmacy 22.37 Locations of palliative care provided by target organizations Home 84.42 Hospital inpatient 48.05 Hospital outpatient 28.57 Residential hospice 22.08 Respite 19.48 Clinic/office 51.95 Other—Long-term care facility, shelter 20.78 Number of palliative care or end of life consults completed in 2017 0 to 5 34.92 6 to 10 11.11 11 to 20 6.35 21 to 30 6.35 30+ 41.27 HIV, human immunodeficiency virus; LGBTQ2SI+, lesbian, gay, bi-sexual, transgender, queer, intersex, two-spirited; MSM, men who have sex with men.
Theme Quote Theme 1: Structural barriers to care outside of the healthcare system The government initiated preference seems to be in home services. However, the in-home service hours allotted to a dying individual seems to be a few hours per day; thus, putting the onus on family members. Unfortunately, homeless people do not have a home and they often lack family members who can help them. Also, homeless people may not know how to access end-of-life services and they may not have a primary health practitioner. (SR) [the shelter system is] phenomenal and by no means am I saying that they're not doing great work. But the first thing that the case worker said to me when I was talking about this medical bed and would it be available for someone who was dying. They specifically said like yeah but we don't want them dying here. (KI 6) I have a gentleman who has cancer and was told that he can't get treatment until he gets housing. So, how is that helpful? What if he was an individual that didn't want housing? So, you're never going to get treatment just because you choose that you don't want housing. That's not OK. (KI 2) Her being in a hospital would mean her friends really couldn't come and stay because they would act inappropriately. There'd be a security person called. They'd be removed. I mean, this is the difficulty. So, she would really be cutting herself off, I think, from that sense of “I'm around the people who I love”. (KI 4) Theme 2: Systemic barriers to care within the healthcare system He was lonely. People that would ah that were kind of familiar with him, that would check on him and stuff for people, that kind of were part of that community and lived in the area, so it was easier for them, you know, with the lack of transportation to go and check up on him at his home. But then being transferred to [institution]—nobody could really access it or people that wanted to, had had such a negative experiences with main stream health care in the first place didn't want to be in that environment. (KI 1) Depending on situation and substance used by specific patient and history of said use. If patient is actively using illicit substances and is regularly intoxicated during clinical encounters, there may be challenges related to communication, compliance, and arranging appropriate follow-up, along with financial challenges related to access, transportation, equipment, and medication costs (SR) Many community programs are “home care” programs—meaning you require a “home” to receive care. (SR) Theme 3: Care avoidance Ah I think there's also, the other problem being the trust. They don't really trust the health care system because they haven't had best dealings for the most part with them, either hospital staff or physicians, and aren't as willing to follow through. (KI 7) A person who is marginalized or substance using or are homeless just may not be able to focus on managing their illness because they're too busy focusing on the day to day stuff. Where they're going to stay. What they're going to eat. What they do for funding. That sort of thing. Being able to kind of see the long term is sometimes difficult and palliative care is partly about planning for that. […] So, you know, I think generally what happens is they get sick to the point that they can't manage and then they end up in hospital and that's when they'll receive their palliative care support. (KI 1) Addiction usually takes precedence over all other life choices. Acknowledging and incorporating drug use into end-of-life care in my opinion would increase engagement of these services. Banning drug use as a requirement for participation in these services would be a huge barrier to engagement. (SR) Theme 4: Stigma as a barrier I had a client that was palliative that would call every day crying saying that he could hear the staff talking about him (KI 1) We're actually supporting a very young individual who is dying currently with very limited palliative resources that he is comfortable accessing. So it's not necessarily that they're not there, but when you use [substances] several times a day, you go to the hospital and they're not giving you the proper medication to keep you comfortable because your tolerance is so high. So you leave the hospital, but then they discharge you because you left against medical advice. So then they don't want to go back. It's kind of the cycle that that we've seen um with other clients in the past (KI 6) We have heard of tenants who have gone, you know, into the hospital for tests and have been refused service because they were told they smelled. (KI 5) I can't fathom how difficult it must be to be trying to do your triage work in emergency. Already demanding and then throw somebody who comes in, you know, high on crystal meth. I make no criticism; however, I think that's a big problem. I'll share a story that was shared with me. [This woman] had suffered a brutal rape. Horrific. Absolutely horrific. She was a woman in her late 40s. Lived on the street throughout her whole life, back and forth. She was telling me her story. She needed to share it […] and she didn't cry. Not one tear when she talked about the abuse that she endured [..]. She wept when she talked about how she got treated at the hospital because she was bleeding so profusely and she flinched at a needle and the comment from the nurse was made to her: “Well look at your arms, as if you have a problem with needles”. That weighed so heavily and this is when the woman broke down. The abuse was horrific but she had almost been marinating in that level of violence and abuse all her life. The devastating part of it all was the shame she felt from the hospital. I just I remember thinking: Holy smokes. Do we ever have a problem here? If what this man did to her- horrify and it's certainly impactful on her but that's not what broke her. What broke her was being so dismissed in hospital because of her I.V. drug use. Yeah. So, you know that's an example of an off the cuff remark made by somebody who I guarantee you had no intention of hurting a woman. (KI 4) So it starts off a negative experience right from the get-go. And generally people don't even stay. I had a client years ago that ended up ah being very unwell. I took him to the hospital. I stayed with him which was fine. People generally are nicer if you have somebody to advocate for them. But as soon as he was admitted into the hospital he ah was treated very poorly by staff. He ended up leaving and he ended up dying in [name of] park by himself. (KI 10) KI, key informant; SR, survey respondent.
- Table 3.
Category Two: Unmet Needs: Gaps in Knowledge, Services and Approaches needed to Enhance End-of-Life Care
Theme Quote Theme 5: Comfort with providing care to those experiencing homelessness Like if you don't think that you can set your judgements aside then you shouldn't be working with these individuals, right? […] And if you're going to cause more harm than good for the individual because you can't set your judgements aside and understand that you took an oath to provide care, then you need not to be working with those individuals. That to me is so so so important. (KI 10) They're invisible. So, for me it's an exciting place to work because these rough looking people but these beautiful spirits come out and their ability to survive. [..] You know it's all those kids we think about when we hear these horrific news stories of abuse. They went into the foster care system and then we don't think of them again but that little kid ends up being the 30-year-old with a criminal record and that little kid ends up being a woman who's prostituted for the last 10 years. (KI 4) Theme 6: Gaps in healthcare provider knowledge and/or attitudes I believe that staff and volunteers would benefit from specified training and development—substance dependency, trauma, other mental health issues, etc. (SR) Compassion training, substance abuse training, harm-reduction training. More of an intensive like mental health training, um, de-escalation—lots of things, you know. Lots of things. (KI 10) Oh we have to start changing the social construct of how we view individuals who use substances, who are homeless, who are suffering with mental health issues. If we don't change our views on how we see these individuals—that they are the root cause of all their problems—then I don't think anything will change. (KI 10) Probably just having a list of services available in the city that you can give them. Like that we can jot down on a piece of paper for them or numbers that we can give them for them to get in contact with the proper people if the hospital doesn't um provide it. And if we had a bit of an idea of what was available I'm sure most of us would at least talk to them about it. (KI 7) Theme 7: Gaps in available services and possible solutions It would be nice to have a space that we could provide for individuals that are palliative that is staffed and supported by individuals who have worked with people with chronic substance use, chronic mental health, the homeless, transient population—that have an understanding and can provide respectful, dignified care (KI 10) We operate out of fixed locations or we operate, you know, at fixed addresses and I think that needs to change. I think, you know, we have a very high percentage of homelessness. And I feel that we need to maybe change some of the ways we're doing things to accommodate people who are unstably housed or living on the street or living at tent city or. I think we should have more outreach, palliative outreach. (KI 6) I could envision an opportunity to even have some of our clients, who were maybe more leaders in this community, getting some training and being able to provide that themselves. [..] Peer support. I think that can be really powerful because there is this kind of kickback against anything they view as authoritative. (KI 4) A harm reduction approach will always provide more options for an individual using illicit substances. If they know that care will still be provided to them in a nonjudgmental way, and in an environment that will address and support them with this issue, they are much more likely to access these services. (SR) KI, key informant; SR, survey respondent.




{kind=link}