
Article Figures & Data
Figures
- Figure 1.
Antihyperglycemia Therapy in Type 2 Diabetes: Consensus of the American Diabetes Association and European Association for the Study of Diabetes.38 ASCVD, atherosclerotic cardiovascular disease; CKD, chronic kidney disease; CVD, cardiovascular disease; CVOT, cardiovascular outcomes trials; DPP-4, dipeptidyl peptidase-4; eGFR, estimated glomerular filtration rate; GLP-1 RA, glucagon-like peptide-1; HbA1C, glycohemoglobin; HF, heart failure; SGLT2i, SGLT2 inhibitor; SU, sulfonylurea; TZD, thiazolidinedione.
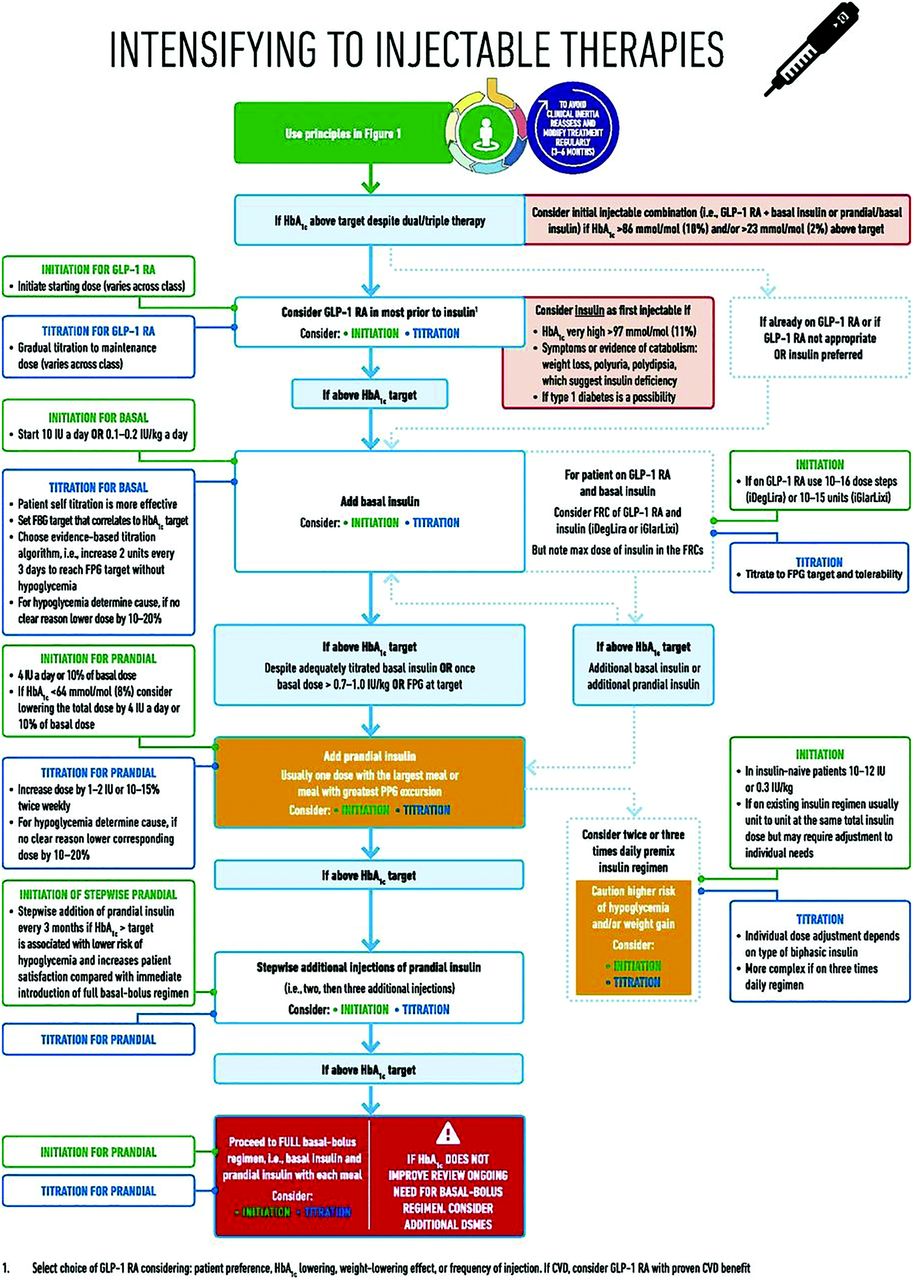
- Figure 2.
Intensification to Injectable Therapies (GLP-1 RAs and Basal Insulin): Consensus of the American Diabetes Association and European Association for the Study of Diabetes.38 FBP, fasting blood glucose; FPG, fasting plasma glucose; FRC, fixed-ratio combination; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HbA1C, glycohemoglobin; IU, insulin units; PPG, postprandial glucose.


Tables
- Table 1.
Summary of Guidelines for Initiation and Titration of Basal Insulin in Patients With Type 2 Diabetes8,39,56,71
Body A1C Target Initiate with Initial Dose of Basal Insulin Titrate to* Titration Instructions Considerations American Diabetes Association/ European Association for the Study of Diabetes 7.0% Basal insulin 10 U or 0.1 to 0.2 U/kg per day FPG <130 mg/dL 2 to 4 U once or twice weekly Target A1C (to be individualized): <7.0% Consider individual patient factors when setting A1C target (health status, concomitant illness, etc.) An algorithm for self titration of insulin doses improves glycemic control International Diabetes Federation <7.0% Basal or premix insulin — FPG <115 mg/dL Dose increases of 2 U every 3 days Explain at diagnosis that because of disease progression, insulin eventually may be the best option for glycemic control Do not unduly delay the commencement of insulin Initiate insulin using a self-titration regimen Explain that starting doses of insulin are low, for safety reasons, but that eventual dose requirement is expected to be 30 to 100 U/day American Association of Clinical Endocrinologists/American College of Endocrinology ≤6.5% Basal insulin If A1C <8.0%: 0.1–0.2 U/kg FPG <110 mg/dL Dose increases of 2 U every 3 days Target A1C for patients without serious concurrent illness and low hypoglycemia risk: ≤6.5% If A1C >8.0%: 0.2–0.3 U/kg A1C target must be individualized Minimizing risk of hypoglycemia is a priority Minimizing risk of weight gain is a priority ↵* Generally a range from ≥80 mg/dL to upper limit shown here.
A1C, glycated hemoglobin A1C; FPG, fasting plasma glucose.
- Table 2.
Manufacturer's Recommended Starting Dose and Conversion to Longer-Acting Basal Insulins from Other Basal Insulin Treatments for Patients with Type 2 Diabetes93–97
Basal Insulin Patient Is Converting to Insulin Glargine 100 U/mL Insulin Detemir LY2963016 (Insulin Glargine 100 U/mL Alternative) Insulin Glargine 300 U/mL Insulin Degludec 100 U/mL or 200 U/mL Starting dose for insulin-naïve patients with T2D 10 units (or 0.2 units per kg body weight) once daily 10 units (or 0.1 to 0.2 units per kg body weight) once daily in the evening or twice daily 0.2 units per kg body weight or up to 10 units once daily 0.2 units per kg body weight 10 units once daily Conversion ratio from other basal insulin treatments 1:1 for once daily NPH 1:1 for NPH or insulin glargine 1:1 for insulin glargine 100 units/mL 1:1 for once daily, long- or intermediate-acting basal insulin 1:1 for once daily basal insulin 80% for twice daily NPH 80% for insulin glargine 300 units/mL or twice daily NPH 80% of daily NPH Titration recommendations* Adjustments should be made according to blood glucose measurements Adjustments should be made according to blood glucose measurements Titrate based on metabolic needs, blood glucose measurements, and glycemic control goal 3 to 4 days between dose increases Adjust and titrate over 3 to 4 days Decrease 2 units if below FPG goal, 0 units if within FPG goal, and increase 2 units if above FPG goal Should be individualized to patient needs and FPG goals ↵* These should be individualized to patient needs.
FPG, fasting plasma glucose; T2D, type 2 diabetes.
Barrier Strategies Complexity of insulin regimens Introduce easy-to-use insulin pens Demonstrate use of pen or watch injection-pen training video with patients Explain that for many people a single daily injection of basal insulin is sufficient to regain and maintain glycemic control for many years Introduce simple titration algorithms and explain that education is available Suggest the use of FDA-approved mobile applications Self blame and feelings of failure Explain that as T2D is highly influenced by age and genetics, insulin is required by approximately 30% of patients as part of the natural course of the disease, not patient behavior Remind patients that insulin is indicated as first- and second-line therapy for T2D and therefore is not a “last resort” Explain that all patients experience β-cell failure but at different rates Introduce the possibility of insulin use at diagnosis Do not use insulin as a “threat” or “punishment” for not dieting, exercising, or taking oral agents Hypoglycemia Give a realistic description of the potential harm and life-threatening potential Explain that incidence of serious hypoglycemia is rare, and give patients estimates of how frequently less serious hypoglycemia occurs Explain that long-acting, once-daily formulations cause less hypoglycemia Give patients advice on how low is “low”, and how to prevent hypoglycemia Express conviction that prophylaxis and treatment of hypoglycemia can be learned Weight gain Explain that once-daily formulations are associated with less weight gain than split-dose regimens Give patients information on how much weight gain is normally observed (<2.5 kg) Provide information on healthy eating and low carbohydrate diets, including dietician advice Reassert that daily exercise can minimize weight gain and improve glycemic control; suggest exercise programs Patient misconceptions regarding insulin Explain that T2D is serious from the beginning, not because insulin is initiated Explore any influential negative experiences the patient may have had Explain that insulin helps to reduce the likelihood of complications and does not cause complications such as amputations or dialysis, etc. Reassure patients who drive for a living that it possible to apply for an exemption to the rule preventing interstate commercial driving Social concerns Explain that basal insulins allow control with a single daily injection which can be administered in private Introduce pen technology, which allows fast convenient administration Let the patient define their special situations Respect the courage needed in the beginning to inject in public Introduce ultra-long-acting insulin, which may allow flexible any-time daily dosing Suggest group classes to discuss social concerns and solutions with peers Injection pain Show that needles are small and very fine Explain injection technique Introduce insulin pens and let the patient touch the device Carry out an initial injection without insulin Explain that pain is often ower with insulin injection than finger-stick glucose measurement Suggest breathing techniques (deep breathing, forceful exhalation) to control anxiety FDA, US Food and Drug Administration; T2D, type 2 diabetes.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Post Hoc Analysis Evaluating the Impact of Antihyperglycemic Background Therapies on Attainment of A1C Targets Without Hypoglycemia in the ACHIEVE Control Pragmatic, Real-Life Study
- Evaluation of Clinical Outcomes With the V-Go Wearable Insulin Delivery Device in Patients With Type 2 Diabetes
- The Most Frequently Read Articles of 2019
- Family Medicine: Data Driven Practice with Emphasis on Underserved Patients