
Article Figures & Data
Figures
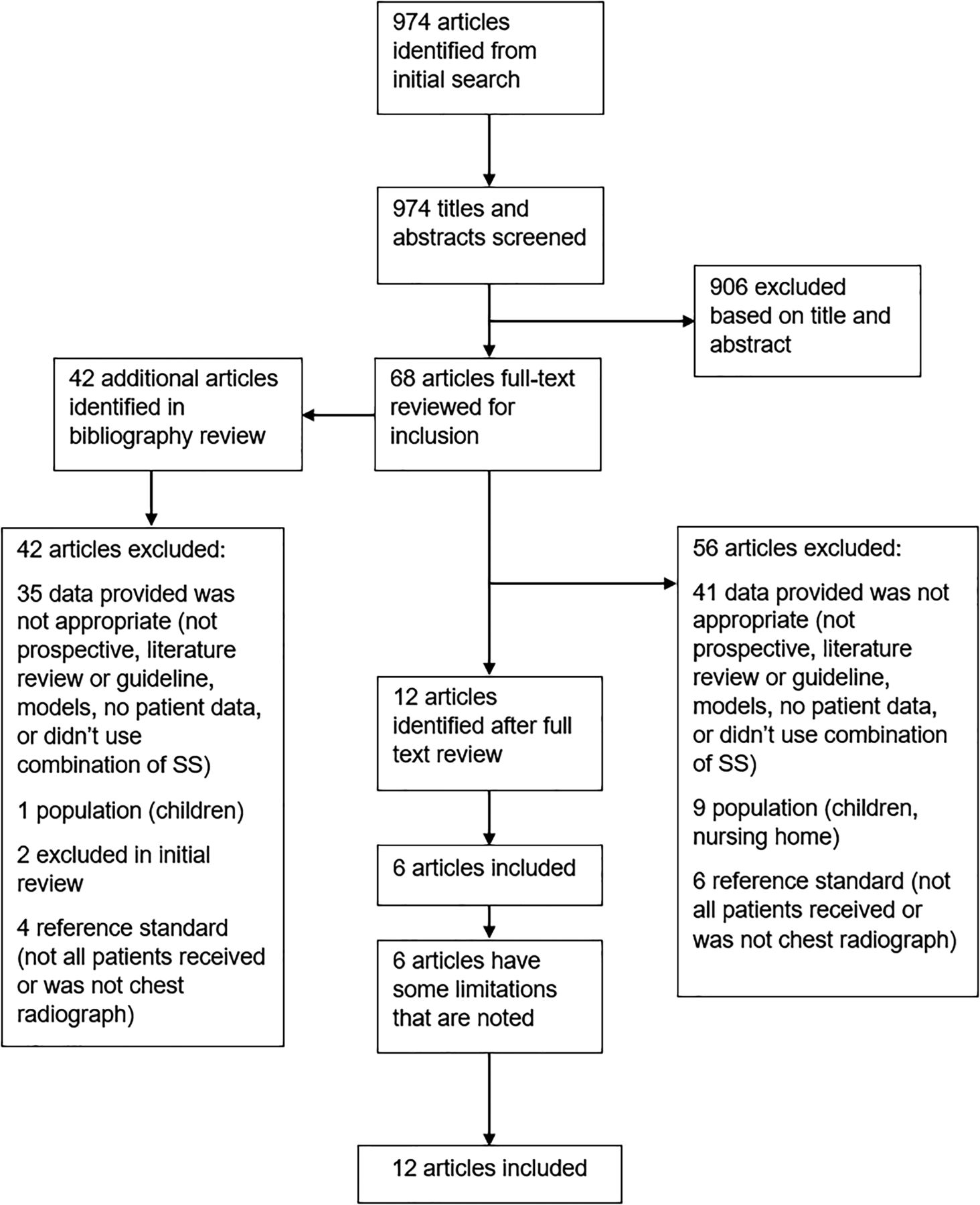
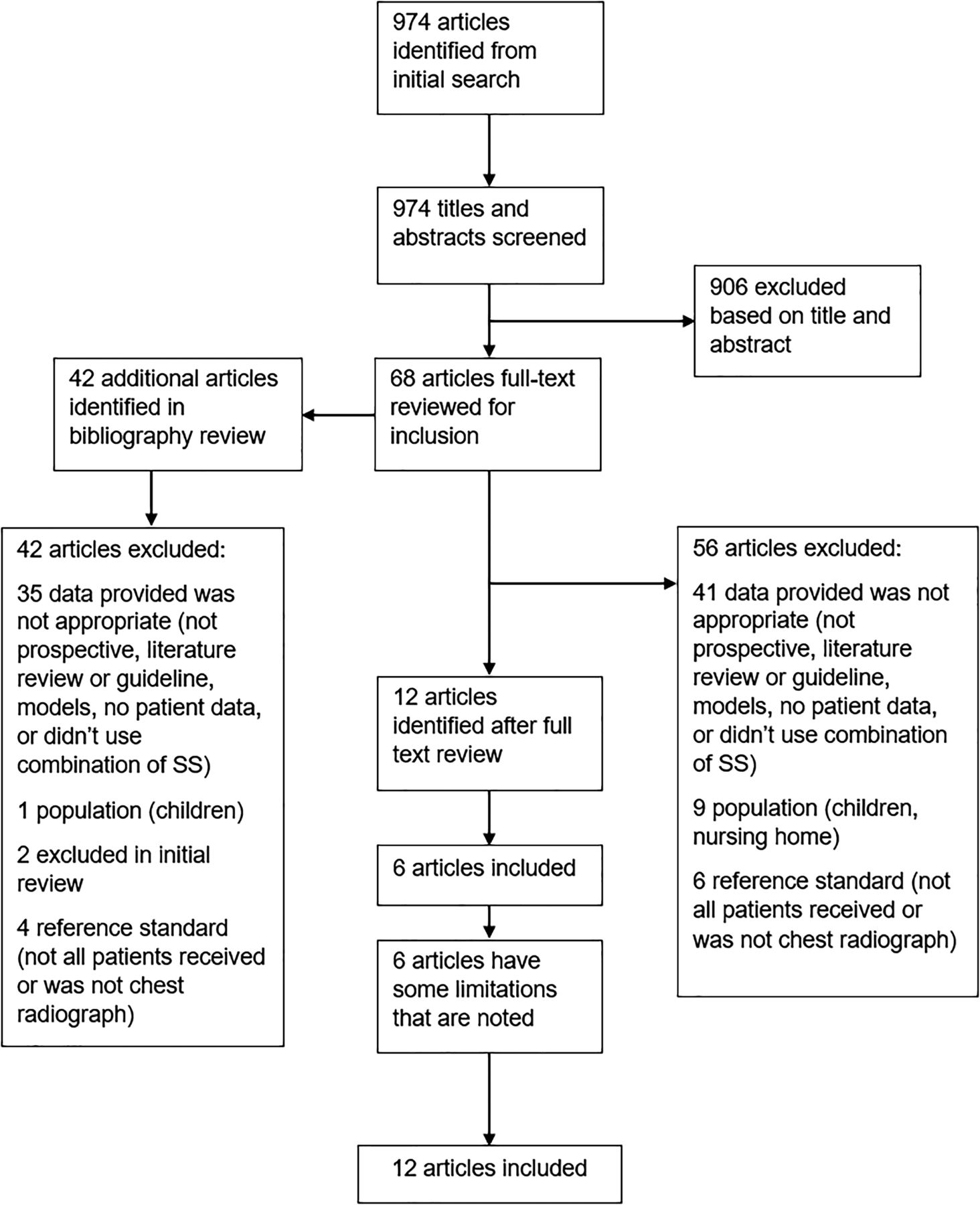
- Figure 1.
PRISMA flow diagram of search strategy and selection of articles.
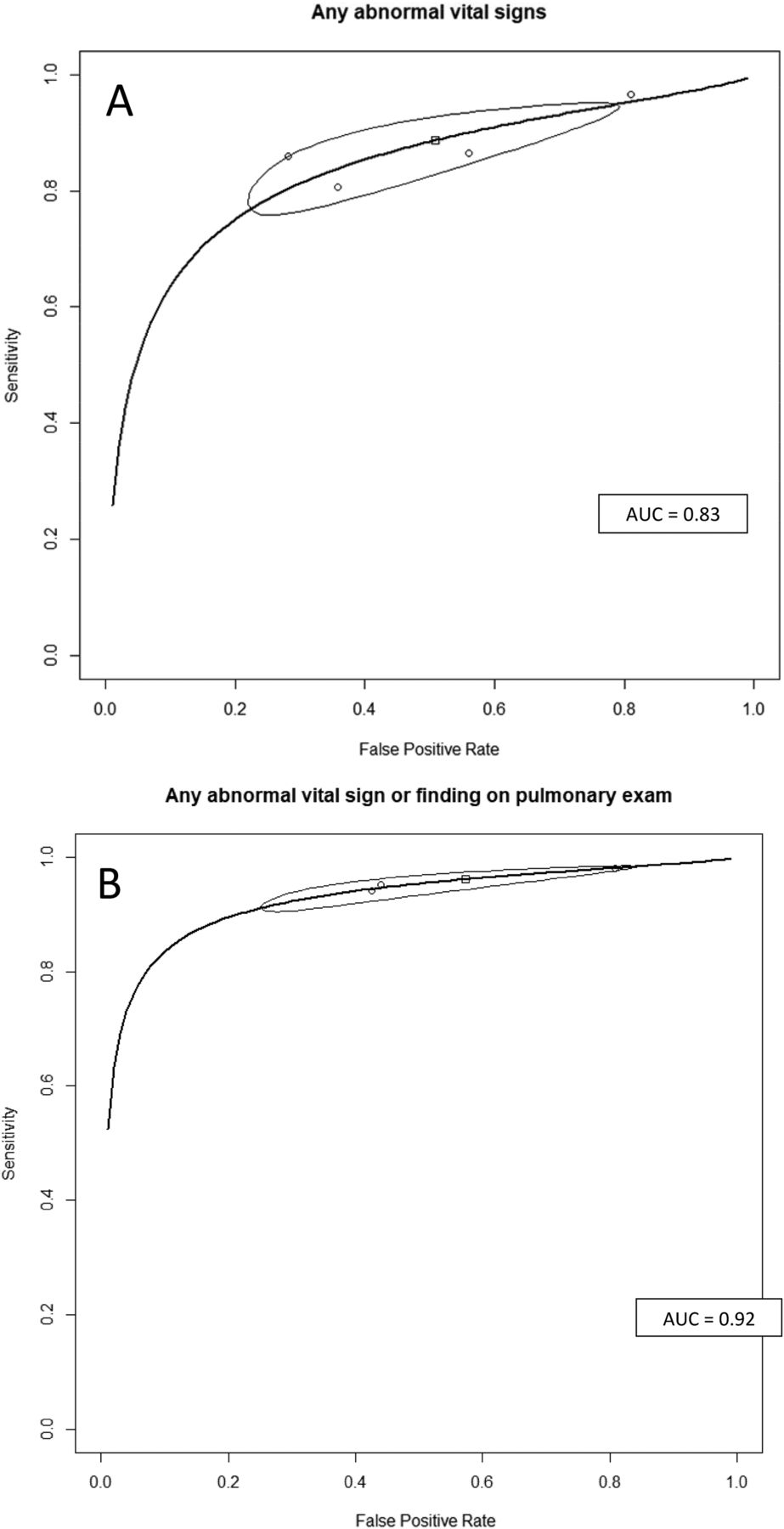
- Appendix B4.
Summary Receiver Operating Characteristic Curves for Clinical Decision Rules Using any Abnormal Vital Signs (A), and Any Abnormal Vital Sign and Abnormal Pulmonary Exam (B) to Diagnose (Rule in) Community Acquired Pneumonia.

Tables
Author, Year Country Design Setting Year Recruited Sample Size Inclusion Age Mean or Median Age Diehr, 19847 United States Prospective ED Not reported 1758 Adults Not reported Gennis, 198920 United States Prospective ED 1984 to 1985 308 ≥16 years 53.6 years (mean) Singal, 198914 United States Prospective ED 1986 to 1987 255 ≥18 years Not reported Heckerling, 19907 United States Prospective ED 1987 to 1988 1436 ≥16 years 45.4 years (mean): Illinois/Nebraska; 41.4 years (mean): Virginia Melbye, 199217 Norway Prospective ED 1988 to 1989 581 ≥18 years 32.1 (mean) Hopstaken, 200318 The Netherlands Cross-sectional/prospective Primary care 1998 to 1999 246 ≥18 years 52 years (mean) O'Brien, 200616 United States Case-control/prospective Outpatient/ED 2004 to 2005 700 ≥18 years 65 years (mean): cases; 66 years (mean): controls Holm, 200719 Denmark Prospective Primary care 2002 to 2003 364 ≥18 years 50 years (median) Saldias, 200715 Chile Prospective ED 2005 325 >15 years 53.4 years (mean) Steurer, 20118 Switzerland Prospective Primary care 2006 to 2009 621 ≥18 years 46.8 years (mean) van Vugt, 20139 12 European countries Prospective Primary care 2007 to 2010 2820 Adults 50 years (mean) Ebrahimzadeh, 201521 Iran Case-control/prospective Outpatient/ED 2008 to 2009 840 ≥18 years 60 years (mean): cases; 63 years (mean): controls ED, emergency department.
Author, Year (Signs, Symptoms, Tests Used in CDR) CDR Score CAP No CAP PV LR Diehr, 19847 −3 0 140 0.0% 0.00 (>37.8°C, −2 4 552 0.7% 0.27 >25 breath/min, −1 8 504 1.6% 0.59 myalgia, night 0 7 316 2.2% 0.82 sweats, sputum, 1 12 124 8.8% 3.60 sore throat, 2 6 52 10.3% 4.29 rhinorrhea) 3 4 12 25.0% 12.41 4 3 8 27.3% 13.96 5 1 4 20.0% 9.30 6 1 0 100.0% † Total 46 1712 Low: −3 to −2* 4 1512 0.3% 0.10 Mod: −1 to 1* 27 176 13.3% 5.7 High: 2 to 6* 15 24 38.5% 23.3 Heckerling, 19906 Derivation: Illinois (>37.8°C, 0 1 48 2.0% 0.12 HR >100/min, 1 11 316 3.4% 0.20 rales, absence of 2 28 232 10.8% 0.70 asthma, decrease 3 42 149 22.0% 1.64 breath sounds) 4 37 30 55.2% 7.18 5 15 5 75.0% 17.5 Total 134 780 Low: 0 to 1* 12 364 3.2% 0.19 Mod: 2 to 3* 70 381 15.5% 1.07 High: 4 to 5* 52 35 59.8% 8.6 Validation: Nebraska 0 0 5 0.0% 0.000 1 3 28 9.7% 0.20 2 11 26 29.7% 0.78 3 12 16 42.9% 1.38 4 11 2 84.6% 10.1 5 5 0 100.0% † Total 42 77 Low: 0 to 1* 3 33 8.3% 0.17 Mod: 2 to 3* 23 42 35.4% 1.00 High: 4 to 5* 16 2 88.9% 14.7 Validation: Virginia 0 1 7 12.5% 0.51 1 2 30 6.3% 0.24 2 8 44 15.4% 0.65 3 6 16 27.3% 1.35 4 11 8 57.9% 4.93 5 1 0 100.0% † Total 29 104 Low: 0 to 1* 3 37 7.5% 0.29 Mod: 2 to 3* 14 60 18.9% 0.84 High: 4 to 5* 12 8 60.0% 54 Pooled 0 2 60 3.2% 0.16 1 16 374 4.1% 0.20 2 47 302 13.5% 0.73 3 60 181 24.9% 1.55 4 59 40 59.6% 6.92 5 21 5 80.8% 19.7 Total 60 205 Low: 0 to 1* 18 434 4.0% 0.19 Mod: 2 to 3* 107 483 18.1% 1.04 High: 4 to 5* 80 45 64.0% 8.33 van Vugt, 20139 (decreased breath sounds, crackles, breathlessness, vesicular breath sounds, absence of runny nose, >37.8C, HR >100/min, CRP >30) CDR w/out CRP Low: <2.5% 11 654 1.7% 0.32 Mod: 2.5% to 20% 105 1987 5.0% 1.01 High: >20% 24 39 38.1% 11.8 Total 140 2680 CDR and CRP >30 Low: 0 4 568 0.7% 0.14 Mod: 1 to 2 73 1829 3.8% 0.76 High: ≥3 63 283 18.2% 4.26 Total 140 2680 - Table 3.
Summary Estimates of Meta-Analysis for the Diagnostic Accuracy of Clinical Decision Rules that Diagnose (Rule in) CAP
CDR Used to Diagnose CAP (Rule in) Sensitivity (95% CI) Specificity (95% CI) LR+ (95% CI) LR− (95% CI) AUROCC Any abnormal vital signs 0.89 (0.79 to 0.94) 0.49 (0.25 to 0.73) 1.84 (1.25 to 3.03) 0.24 (0.17 to 0.34) 0.83 Any abnormal signs or any abnormal pulmonary exam finding 0.96 (0.92 to 0.98) 0.43 (0.20 to 0.69) 1.79 (1.22 to 3.01) 0.10 (0.07 to 0.13) 0.92 AUROCC, area under the receiver operating characteristic curve; CAP, community-acquired pneumonia; CDR, clinical decision rule; CI, confidential interval; LR, likelihood ratio.
- Table 4.
Simulated Primary Care (4%) and Emergency Department (20%) Prevalence Rates for Selected CDRs
LR % CAP Given Baseline Prevalence of Score or CDR 4% 20% Normal signs and no pulmonary finding15,16,21 0.10 0.4% 2.4% Normal vital signs15,16,20,21 0.24 1.0% 5.7% Diehr, 19847 Low (−3 to −2)* 0.10 0.4% 2.4% Mod (−1 to 1)* 5.7 19.2% 58.8% High (2 to 6)* 23.3 49.2% 85.3% Heckerling, 19906 Pooled (all 3 states) Low (0 to 1)* 0.19 0.8% 4.6% Mod (2 to 3)* 1.04 4.1% 20.6% High (4 to 5)* 8.33 25.8% 67.6% van Vugt, 20139 Low (0) 0.14 0.6% 3.3% Interm (1 to 2) 0.76 3.1% 16.0% High (≥3) 4.26 15.1% 51.6% ↵* Risk groups calculated post hoc and were not in original publication.
CAP, community-acquired pneumonia; CDR, clinical decision rule.
- Appendix B1.
Assessment of Study Quality Using the Quality Assessment Tool for Diagnostic Accuracy Studies (QUADAS-2) Framework
Author, Year Consecutive or random sample enrolled? (Y/N/U) Case-control design avoided? (Y/N/U) Avoided inappropriate exclusion criteria? (Y/N/U) Likelihood that patient selection could have introduced bias? (H/L/U) Concerns that included patients and setting do not match the review question? (Y/N/U) CDR results interpreted without knowledge of reference standard? (Y/N/U) Likelihood that conduct or interpretation of the CDR have introduced bias? (H/L/U) Concerns that the CDR differs from the review question? (Y/N/U) Reference standard likely to correctly classify patients as pneumonia? (Y/N/U) Reference standard interpreted without knowledge of index test? (Y/N/U) Likelihood that conduct or interpretation of reference standard introduced bias? (H/L/U) Conditions defined by the reference standard do not match the review question? (Y/N/U) All patients receive a reference standard? (Y/N/U) Did all patients receive the same reference standard? (Y/N/U) Were all patients included in the analysis? (Y/N/U) Patient flow have introduced bias? (H/L/U) Overall assessment of risk of bias (H/M/L) Diehr, 1984 Y Y Y L N Y L N Y Y L N Y Y Y L L Ebrahimzadeh, 2015 U N Y H N Y L N Y Y L N Y Y Y L M Gennis, 1989 Y Y N H N Y L N Y Y L N Y Y Y L M Heckerling, 1990 Y Y N H N Y L N Y Y L N Y Y Y L M Holm, 2007 Y Y Y L N Y L N Y Y L N Y Y Y L L Hopstaken, 2003 Y Y Y L N Y L N Y Y L N Y Y Y L L Melbye, 1992 Y Y Y L N Y L N Y Y L N N Y Y H M Obrien, 2006 U N Y H N Y L N Y Y L N Y Y Y L M Saldias, 2007 Y Y Y L N Y L N Y Y L N Y Y Y L L Singal, 1989 Y Y N H N Y L N Y Y L N Y Y Y L M Steurer, 2011 Y Y Y L N Y L N Y Y L N Y Y Y L L van Vugt, 2013 Y Y Y L N Y L N Y Y L N Y Y Y L L Y: yes; N: No; U: unknown; H; high, M: moderate; L: low; CDR: clinical decision rule.
- Appendix B2.
Individual Signs, Symptoms, and Point Care Tests Used in Clinical Decision Rules (CDRs) to Diagnose or Rule Out Pneumonia
Author, Year Temp (C) Pulse (per min) Crackles Decreased breath sounds Resp (per min) Other signs, symptoms or point of care tests Diehr, 1984 >37.8 >25 sore throat night sweats myalgia rhinorrhea sputum Ebrahimzadeh, 2015 ≥38 ≥100 X X ≥20 CRP dullness on percussion rhonchi ESR WBC Gennis, 1989 >37.8 >100 X >20 rales wheezes rhonchi Heckerling, 1990 >37.8 >100 X rales absence of asthma Holm, 2007 CRP clinical pneumonia SATO2 Hopstaken, 2003 ≥38 CRP<20 diarrhea ESR <20 dry cough Melbye, 1992 X X pleural rubs dullness on percussion Obrien, 2006 ≥38 ≥100 X X >20 rhonchi dullness on percussion Saldias, 2007 ≥38 ≥100 X ≥20 orthopnea dullness on percussion abnormal auscultation Singal, 1989 X X cough Steurer, 2011 X CRP >11 dyspnea van Vugt, 2013 >37.8 >100 X X CRP >30 breathlessness Vesicular sounds absence of runny nose Boxes in gray indicate not used in study. X: used in study but did not give specific value; Temp: temperature in Celsius.
Resp: respiratory rate; CRP: c-reactive protein ESR: erythrocyte sedimentation rate; WBC: white blood cell count; SATO2: oxygen saturation.
- Appendix B3.
Diagnostic Accuracy of Clinical Decision Rules Using Signs, Symptoms, and Point of Care Tests to Diagnose (Rule In) Pneumonia
Author, Year CDR used to diagnose CAP (rule in) CDR expressed as low yield criteria (rule out) Sensitivity (TP/TP+FN) Specificity (TN/TN+FP) LR+ LR− Ebrahimzadeh, 2015 Any abnormal VS Normal VS 0.86 (361/420) 0.72 (302/420) 3.06 0.20 Any abnormal VS or PE finding Normal VS and no PE findings 0.94 (395/420) 0.57 (241/420) 2.21 0.10 Any abnormal lab (CRP, ESR, WBC) Normal labs 0.60 (254/420) 0.74 (310/420) 2.31 0.54 Gennis, 1989 Any abnormal VS Normal VS 0.97 (114/118) 0.19 (36/190) 1.19 0.18 Any abnormal auscultatory findings Normal auscultatory findings 0.78 (92/118) 0.38 (73/190) 1.27 0.57 Holm, 2007 GP diagnosis of CAP and CRP ≥ 20 GP diagnosis of CAP or CRP < 20 0.49 (23/47) 0.84 (249/297) 3.03 0.61 GP diagnosis of CAP and SATO2 ≤ 95% GP diagnosis of CAP or SATO2 > 95% 0.32 (15/47) 0.92 (268/291) 4.04 0.74 GP diagnosis of CAP or CRP ≥ 20 GP diagnosis of CAP and CRP < 20 0.83 (39/47) 0.48 (144/297) 1.61 0.35 GP diagnosis of CAP or SATO2 ≤ 95% GP diagnosis of CAP and SATO2 > 95% 0.79 (37/47) 0.56 (164/291) 1.80 0.38 Hopstaken, 2003 >1 (diarrhea, dry cough, ≥ 38C) or CRP ≥ 20 <=1 of 3 sign/symptom + CRP <20 0.91 (29/32) 0.49 (104/211) 1.79 0.19 >1 (diarrhea, dry cough, ≥ 38C) or ESR ≥ 20 <=1 of 3 sign/symptom + ESR <20 0.81 (26/32) 0.55 (115/211) 1.79 0.34 Melbye, 1992 Abnormal auscultatory signs Normal auscultatory signs 0.40 (8/12) 0.88 (336/382) 3.32 0.68 O'Brien, 2006 Any abnormal VS Normal VS 0.81 (282/350) 0.64 (225/350) 2.26 0.30 Any abnormal VS or PE finding Normal VS and no PE findings 0.95 (333/350) 0.56 (196/350) 2.16 0.09 Saldias, 2007 Any abnormal VS Normal VS 0.86 (89/103) 0.44 (85/193) 1.54 0.31 Abnormal VS or PE finding Normal VS and no PE findings 0.98 (101/103) 0.19 (37/193) 1.21 0.10 Singal, 1989 Fever, cough, crackles Absence of fever, cough, crackles 0.93 (37/40) 0.27 (57/215) 1.26 0.28 Steurer, 2011 CRP>50 or CRP 11–50 and dyspnea or daily fever CRP < 10 or CRP 11–50, no dyspnea, and no daily fever 1.00 (127/127) 0.38 (190/494) 1.63 0.00 CDR: clinical decision rule; CAP; community-acquired pneumonia; VS: vital signs; PE: pulmonary exam; GP: general practitioner; CRP: c-reactive protein; ESR: erythrocyte sedimentation rate; WBC: white blood cell count; SATO2: oxygen saturation; Sensitivity and specificity calculated using ruling in criteria.
Dier, 1984
Symptom Points/Score assigned Rhinorrhea −2 Sore throat −1 Night sweats 1 Myalgia 1 Sputum all day 1 Respiratory rate >25 2 Temp. 100F or more 2 Heckerling, 1990
Symptom Logistic coefficient Temp. > 37.8C 0.494 Pulse ?100 beats/min 0.428 Rales 0.658 Decreased breath sounds 0.638 Absence of asthma 0.691 Intercept −1.705 Van Vugt, 2013
Symptom Points/Score assigned Absence of running nose 1 Breathlessness 1 Crackles 1 Diminished vesicular breathing 1 Raised pulse (>100/min) 1 Fever (temp. >37.8C) 1 Raised CRP (>30 mg/L) 1 CRP, c-reactive protein.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnosing community-acquired pneumonia via a smartphone-based algorithm: a prospective cohort study in primary and acute-care consultations
- Diagnosing Community-Acquired Pneumonia: diagnostic accuracy study of a cough-centred algorithm for use in primary and acute-care consultations
- Challenges in the virtual assessment of COVID-19 infections in the community
- The Most Frequently Read Articles of 2019
- Response: Re: Signs and Symptoms That Rule Out Community-Acquired Pneumonia in Outpatient Adults: A Systematic Review and Meta-Analysis
- Multiple Research Methodologies Can Advance the Science of Family Medicine