
Article Figures & Data
Figures
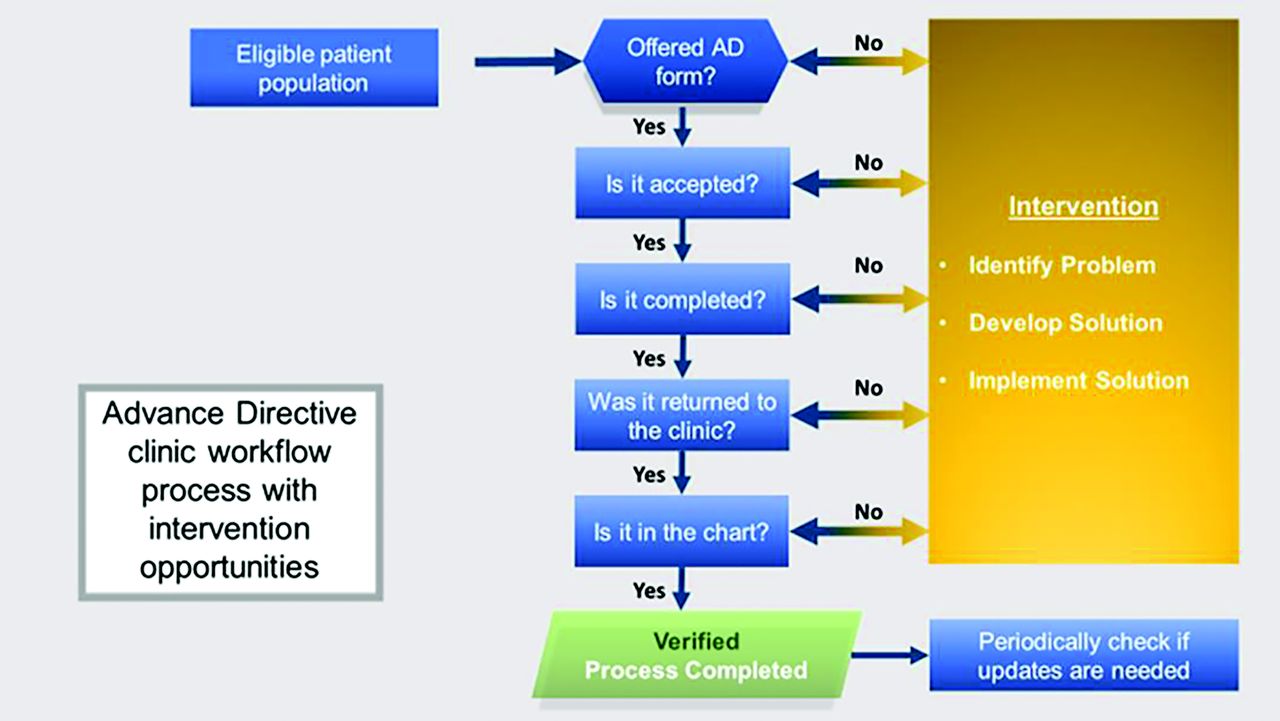
- Figure 1.
Workflow process for the distribution of advance directives in the clinics.
- Figure 2.
Age distribution pf participating patients in the study.


Tables
Pair Match Practice Type 2013 Locale Population Panel Size Pts/Day % Medicare Reg Use of AD Form % Discuss AD 1 FQHC 17,140 >2000 12 25 to 49 N 0 1 Independent 6,027 >3000 >40 50 to 74 N 1 to 24 2 Residency/Corporate 610,613 >3000 30 to 39 25 to 49 N × 2, Y × 1 1 to 24 2 Residency 610,613 >3000 40 25 to 74 Y × 1, N × 4 1 to 24 3 Independent 23,400 >3000 10 to 19 25 to 49 N 0 3 Independent 17,140 >3000 20 to 29 50 to 74 N 1 to 24 2013 Locale Population, based on 2013 data; % Discuss AD: Estimated percent of patients with whom the clinician believes they discuss ADs at baseline; FQHC, Federally Qualified Health Center; pts/day, estimated average number of patients seen per day; % Medicare, estimated percent Medicare-insured patients; Reg Use of AD Form, Does the clinician use an AD form on a regular basis? (Y, yes; N, no, ×# indicates how many clinicians gave this answer).
AD, Advance Directive.
Category Characteristic Count Percentage, % Gender Male 232 35 Female 440 65 Race/ethnicity White 337 73 Black 54 12 Hispanic/Latino 31 7 Native American/Alaskan 7 2 Asian/Pacific Islander 32 7 Count is limited to the number of patient participants for whom this information was recorded by the clinical staff.
Form Eligible Offered Offered/Eligible, % Accepted Accepted/Offered, % Accepted/Eligible, % OKAD 1494 493 33 266 54 18 Five Wishes 1254 450 36 369 82 29 OKAD, Oklahoma Advance Directive.
Form Practice Weeks in Study Eligible Offered O/E Accepted A/O A/E OKAD 1 17 816 288 35% 147 51% 18% 3* 17 134 68 51% 39 57% 29% 6* 14 544 137 25% 80 58% 15% Five Wishes 2* 22 413 163 39% 93 57% 23% 4 15 733 254 35% 252 99% 34% 5 16 108 33 31% 24 73% 22% Total 2748 943 34% 635 67% 23% ↵* Practices going through electronic health record transition during this study.
A, accepted; AD, Advance Directive; E, eligible; O, offered, OKAD, Oklahoma Advance Directive.
Qualitative Themes for Patients and Clinicians Theme Subtheme Representative Quotes OKAD Five Wishes Capturing wishes Clinicians • I tell the patients, ‘If it is not clear [the wording of the form], write it in [ie., patients write in their wishes on the form].’ Then it does fine. [This is a workaround this clinician devised for the OKAD]. • I think it captures their wishes very well and helps stimulate questions and other information or desires they had not thought of in the past. • I think it is good on that. I looked it over. [This clinician could not identify the details of the form to explain what he thought made it adequately designed.] • It's improved compared to the state-approved document. • Useful tool. • To me, the way it [The Five Wishes form] is developed makes it a very good document. Patients • Can't remember the form very well. • Quite well • They give you a chance to change anything you may want to change. • Very well • I would have to read it all over again. I don't think you want to spend the time on that again. • As I recall, my husband and I did them together… he's in healthcare so he was able to answer any questions I had. Reading level, language, and form design Clinicians • Pretty readable • I like it. It's worded in a way that people can understand it and what it is. • About what you would expect • They can understand how to word or communicate what they want out of it and it's not so scary-sounding in the way that it is worded. The way it is worded it is positive. • It might be a challenge for some people. • I have given the form out myself to patients who are not enrolled in the study as well. • In general, I think it is appropriate, but I probably tend to assume a level of comprehension that my patients may not possess, and I think they are often uncomfortable bringing that up and telling me, even if I ask if they understand it or not. Regarding form design: • I also realized the form itself is very complicated and it's hard to read at a different level • It's just laid out really simply. • It's almost like a conversation. Regarding form design: Asked about length: • It's OK. • I don't know how you can put in there [in the form] everything that has to be covered. So, there is a lot of stuff that goes into it, but it explains everything, so I think if you take that out it makes it to where they can't understand what you're asking of them. You can make it short and they're not going to answer it. • It requires some explanation, but it's OK. • Typically get zero positive input on the state form [from a clinician in the Five Wishes arm of the study]. Patients • Well, with all those extra pages [explanatory booklet] that they gave me, and I thought ‘Oh my word!’ … it just kept me putting it aside because I didn't want to mess with it. • I thought it was very informative, really, gave me a lot of ideas I wouldn't think of if I didn't have this form. • In fact, we had checked some stuff that we didn't understand until the RN told us, ‘now, do you understand that when you check off that they use all parts of your body, but if you just specify the ones that you want done, your body will only take 2 days but otherwise it will take 2 weeks.’ • … If you have seen the regular one [state form], then you know what a bunch of jumble mumble [it is]!… but this one is–I just don't see how it could be much simpler. • Very easy to understand. • It explains itself very well. • I have no qualms with it at all. I understood it. Family and cultural context Clinicians • Frequently people want to put more than one name on a line. • Health care proxy selection easier. • Allows discussion of cultural differences in a respectful and culturally-sensitive manner. • Several people really liked Wish 5. Patients • I had already [completed an AD], once I saw that Terri Schiavo mess and how they were recommending it. Plus, my mother died without one and they had to pull the plug … and that was like 10 years ago. So that is when we thought, ‘No. we need to make sure we have this.’ • The only problem I had with it is, I am sitting here looking at it right now, I had talked to my daughter it said first1st choice and second choice, but my two daughters felt like they should both be the person to help with my care, not the second choice Patients • I must say my son was really wigged out that he thought he was in charge of deciding whether to pull the plug or not. My daughter is a respiratory therapist and so she just told him to not worry about it–‘You won't be the only one there. I can make sure it's a hopeless kind of thing.’ [however, daughter lives out of state, so son is first on HCP form]. Implementation success Clinicians • I feel like I have a decent number of patients that have completed it but percentage wise, I don't know [answer to the question as to how successful the clinician thought they were with implementation]. • The Five Wishes form is more accessible [than the state form]. • Not good. • I know of a number of patients who have brought the [completed] form in to me [since the start of this study]. • [Our lack of success of implementation had nothing] to do with the form. It's just remembering to get that in. The form itself is fine. Patients • It's with all of those other pages they gave me and I thought, ‘Oh my word!’ … it just kept me putting it aside because I didn't want to mess with it. • I know I should have already had it turned back in. • I got everything on there. I just got to get it back to him [the doctor]. Facilitating EOL discussions Clinicians • I tell patients, ‘I know it is silly, but it is important for us to have these conversations … the state requires that I do … it's really just protecting your family when you are no longer able to state your wishes.’ • [this form] helps patients understand their responsibility (for the need to make end of life care decisions): ‘Who would speak for you [if you couldn't speak for yourself]?’ • I think it has been helpful. • Prior to this study I thought I was doing a pretty good job. During the study I realized that the form itself was important. • I haven't noticed that it has done much for that. • The [Five Wishes] form itself does facilitate the communication part at home more so than the others [other AD forms]. • More concrete. Takes the feeling out of it, the emotional component out of it. It's more cognitive. You know, 'Check, check, check.' • [The Five Wishes form] gets you to think about how you would want to get care if you were very sick. Patients • Right now, I am healthy. I am not giving it too much thought of what my end of life will be like, but if I was closer to death I would probably be a bit more [interested in this type of discussion.] • I don't know if I can tell you how she [the nurse] explained it to me, but she did explain it enough. AD, Advance Directive; EOL, end of life; HCP, healthcare Proxy; OKAD, Oklahoma Advance Directive; RN, registered nurse.
Qualitative Themes for Clinicians Subtheme Common barriers to implementation for both forms Time • Almost all clinicians in both study arms reference the extra time required, ranging from 30 seconds to 20 minutes, averaging approximately 3 to 5 minutes extra. • Several didn't mind finding the time because they felt it was important. Reimbursement codes help. Barriers and facilitators identified • Forgetting to offer forms, misunderstandings about how to address existing/multiple forms, pts forgetting to complete forms, pts forgetting to return forms, new EHR implementation, location and managing forms in EMR. Facilitators: involvement of nursing staff as part of the introduction, important to be part of the check-in flow/routine, offer to everyone, script cards for nursing staff. • Lack of sustainable reminders in place; numerous competing priorities; time pressures; EHR system change; Facilitators: systematic planning; effective teamwork; securing buy-in from entire clinic prior to implementation; professional experience with EOL conversations; “Bringing the attention.” EHR, electronic health record; EOL, end-of-life.





{kind=link}
{kind=link}