
Abstract
Background: A recent regional study found lower burnout among primary care clinicians who perceived that their clinic had greater capacity to meet patients' social needs. We aimed to more comprehensively investigate the association between clinic capacity to address social needs and burnout by using national data that included a more representative sample of family physicians and a more comprehensive set of practice-level variables that are potential confounders of an association between clinic social needs capacity and burnout.
Methods: We conducted a cross-sectional analysis of 1298 family physicians in ambulatory primary care settings who applied to continue certification with the American Board of Family Medicine in 2016. Logistic regression was used to test associations between physician and clinic characteristics, perceived clinic social needs capacity, and burnout.
Results: A total of 27% of family physicians reported burnout. Physicians with a high perception of their clinic's ability to meet patients' social needs were less likely to report burnout (adjusted odds ratio [OR], 0.66; 95% confidence interval [CI], 0.47–0.91). Physicians who reported high clinic capacity to address patients' social needs were more likely to report having a social worker (adjusted OR, 2.16; 95% CI, 1.44–3.26) or pharmacist (adjusted OR, 1.73; 95% CI, 1.18–2.53) on their care team and working in a patient-centered medical home (adjusted OR, 1.65; 95% CI, 1.24–2.21).
Conclusion: Efforts to reduce primary care physician burnout may be furthered by addressing structural issues, such as improving capacity to respond to patients' social needs in addition to targeting other modifiable burnout risks.
In light of a growing recognition that clinician well-being is a foundational component of a high-functioning health care system,1,2 it is alarming that more than 60% of US family physicians report symptoms of burnout.3 A new body of research has emerged exploring both clinician- and practice-level risk factors for burnout as potential targets for intervention. Reported clinician-level burnout risk factors include being midcareer4, spending a higher percent time in clinical activities5,6, and being female.7,8 Reported practice-level burnout risk factors include electronic health record (EHR) burden9,10, work stress, poor team efficiency6,9,10⇓–12, and poor or misaligned clinical leadership.9,12,13
Burnout is of particular concern in United States safety-net practices, where the level of need frequently exceeds available resources.14⇓⇓–17 In these settings, one study with a relatively small sample size suggested that risk factors for burnout extend beyond common clinician and practice variables associated with burnout to include insufficient organizational resources to address patients' social needs.18 This association between clinic capacity to address social needs and clinician burnout has not been examined in large, representative samples of physicians.
The current study leverages survey data from a national sample of family physicians from diverse settings applying to the American Board of Family Medicine (ABFM) to continue their specialty certification. The study goals were to (1) better understand the associations between burnout, clinic capacity to address patients' social needs, and other burnout risk factors; and (2) to identify practice-level factors associated with clinic capacity to address patients' social needs. We hypothesized that physicians who did not perceive that their clinic was equipped to meet the social needs of their patients would have higher burnout and that the inverse relationship between social needs capacity and burnout would be stronger for physicians working in safety-net settings.
Methods
Survey data are from the 2016 ABFM Family Medicine Certification practice demographic questionnaire. The questionnaire is a mandatory component of examination registration, which occurs 3 to 4 months before the examination date. In the 2016 ABFM continuing certification process, all applicants completed a core set of questions, which included a measure of physicians' perception of their clinic's capacity to address patients' social needs. Applicants were also randomized to 1 of 5 modules, 1 of which included measures of burnout and burnout risk factors. The study was reviewed by the University of California San Francisco Institutional Review Board and deemed not human subjects research (15–18360).
Study Sample
Of the 9658 physicians applying to continue their certification (survey response rate 100%), 1925 were randomly administered the burnout module. We then excluded burnout module respondents if their primary worksite was not either a freestanding ambulatory care clinic or a hospital-based clinic (n = 542); if they reported having less than 1 year of clinical practice experience (n = 11); or if they reported not having an EHR and, therefore, were not offered the burnout module questions on EHR use (n = 74). After these exclusions, 1298 participants were included in the study sample.
Measures
Self-Reported Burnout
The primary burnout outcome was measured using a validated, single-item question asking physicians to rate their level of burnout (1 to 5 scale) (Table 1).19 As has been done in earlier studies,20 we dichotomized the burnout measure so that reporting no symptoms of burnout or stress was considered “not burned out” (score 1 or 2), whereas reporting greater than 1 symptom of burnout was considered “burned out” (score ≥3).
Single-Item Burnout Question and Response Options from the 2016 American Board of Family Medicine Certification Practice Demographic Questionnaire, Dichotomized to Indicate Primary Reported Outcome of Burnout Versus Not Burned Out
Perceived Clinic Capacity to Address Patients' Social Needs
The primary predictor variable was a single-item measure of physician-reported clinic capacity to address patients' social needs (clinic social determinants of health [SDH] capacity). This measure was used in a prior study of primary care clinicians and found to have both high face- and content-validity.18 The question read: “My clinic has the resources, such as dedicated staff, community programs, resources or tools to address patients' social needs,” with a Likert response scale ranging from strongly disagree to strongly agree (1 to 10). We dichotomized responses at the median for responses in this national sample (<6 = low perceived clinic capacity; ≥6 = high perceived clinic capacity).
Covariates
We included covariates that were both known to be associated with burnout and available in ABFM data, including patient-centered medical home (PCMH) status, percent vulnerable patient population (no definition was provided in the survey), race, ethnicity, gender, and years in practice; staffing support (having a social worker, pharmacist, behavior specialist, or psychiatrist); type of practice (“private practice,” “hospital- or health maintenance organization [HMO]-based,” or “federally qualified health center [FQHC] or similar”); practice size (“solo,” “small [2 to 5 clinicians],” “medium [6 to 20 clinicians],” or “large [20+ clinicians]”); type of employment (“employee,” “owner,” or “contractor”); and being medical school and/or residency faculty (“no,” “yes, part-time,” “yes, full-time”).
Statistical Analysis
Primary analyses focused on the association between perceived clinic SDH capacity and burnout, controlling for known burnout predictors. In a secondary analysis, we examined factors hypothesized to be associated with clinic SDH capacity and whether those factors mediated associations between clinic SDH capacity and burnout. Bivariate analyses between the covariates and the primary outcome (burnout) were performed to assess unadjusted associations (χ2 and bivariate logistic regression). Multivariable logistic regression analyses were performed to control for covariates based on physician burnout literature. Interaction terms between covariates and the clinic SDH capacity variable assessed for a possible buffering or exacerbation of the association with burnout.
To evaluate the individual- and clinic-level characteristics associated with clinic SDH capacity, we conducted bivariate and multivariable logistic regression analyses by using the predictor variables hypothesized to contribute to clinic SDH capacity. To evaluate whether the factors associated with clinic SDH capacity were driving the association between clinic SDH capacity and burnout, the original multivariable logistic regression analysis for the outcome of burnout was repeated, controlling for the factors hypothesized to contribute to clinic SDH capacity. Interaction terms between covariates found to have a significant association with clinic SDH capacity and burnout were evaluated for effect modification on clinic SDH capacity.
The study was powered 0.80 or greater (α = 0.05, 2 sided) to detect an absolute difference of 7% in the primary binary outcome of burnout between groups reporting high and not high clinic SDH capacity. All data analyses were conducted using Stata/SE 15.0.
Results
Of 1298 family physicians responding to the burnout module in our sample, the mean age was 56 years, 44% were male, 72% were white, and mean years in practice was 19 (Table 2). Close to 90% reported having more than 50% direct patient care time. Eighty-two percent of respondents reported working in freestanding ambulatory clinics (vs hospital-based clinics); 59% were in private practice, and 24% in hospital- or HMO-based clinics. Most worked in small (2 to 5 clinicians) or medium-sized (6 to 20 clinicians) practices (34% and 35%, respectively). Forty-three percent reported working in a recognized PCMH; 43% reported that more than 20% or more of their patients were members of vulnerable populations.
Respondent-Reported Physician and Practice Site Characteristics by Burnout and Perceived Clinic Social Determinants of Health Capacity Among 1298 Family Physicians Applying for Continuous Certification with the American Board of Family Medicine in 2016*
Internal ABFM analyses showed no differences in physician characteristics between the 5 modules. However, when comparing respondent characteristics for the full ABFM survey to only those included in our study sample, there were 2 differences. In the study sample, there was a higher percentage of males (44% vs 41%, P = .014) and fewer physicians caring for large numbers of vulnerable patient populations (43% with >20% vulnerable patients vs 51% with >20% vulnerable patients, P < .001).
Association between Perceived Clinic Capacity to Address Patients' Social Needs and Burnout
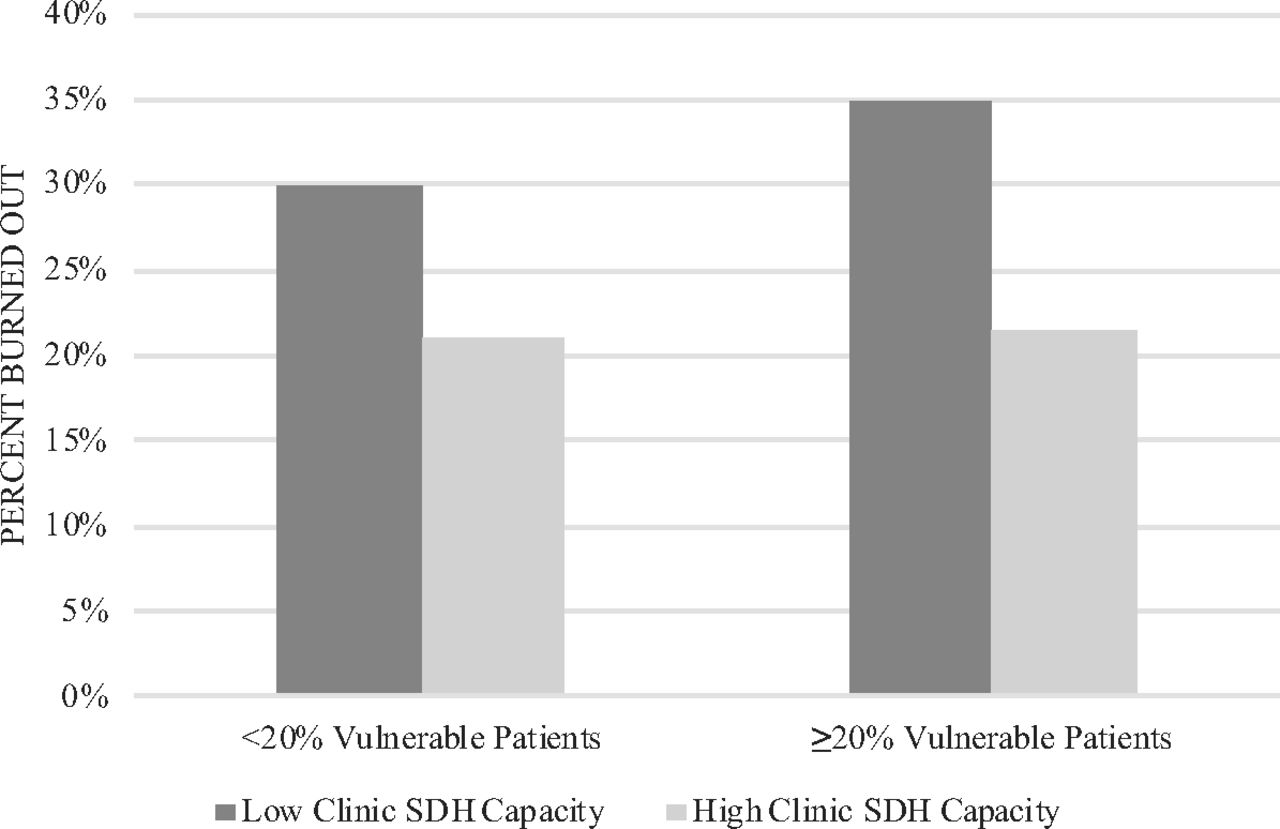
Twenty-seven percent of respondents reported burned out symptoms, similar to the 25% reported in a recent study using a less restricted sample of these same respondents.21 In unadjusted analyses, respondents who reported high clinic capacity to address patients' social needs had lower odds of burnout than those reporting lower capacity to address patients' social needs (odds ratio [OR], 0.58; 95% confidence interval [CI], 0.45–0.74) (Table 3). In multivariable analysis, the inverse association between clinic SDH capacity and burnout remained significant (OR, 0.71; 95% CI, 0.52–0.98). Among the covariates, high workload control, high team efficiency, and minimal time documenting in the EHR at home were also significant predictors of burnout in the multivariable model. In additional analyses conducted to account for factors hypothesized to contribute to clinic SDH capacity, the inverse association between burnout and clinic SDH capacity remained statistically significant (OR, 0.66; 95% CI, 0.47–0.91), as did inverse associations between burnout and high workload control, high team efficiency, and minimal time documenting in the EHR. There were no statistically significant interactions between perceived clinic SDH capacity and other covariates in predicting burnout, including no significant interaction between SDH capacity and proportion of vulnerable patients in the practice in predicting the outcome of burnout. Reported levels of burnout, by level of clinic SDH capacity and stratified by vulnerable patient population, were similar for respondents working in practices with less than 20% and 20% or higher vulnerable patients (P = .29), with a nonsignificant trend toward high clinic SDH capacity having a greater buffering effect on burnout for physicians working with a higher number of vulnerable patients [Insert Figure 1].
Unadjusted and Adjusted Association between Clinic Social Determinants of Health Capacity and Self-Reported Burnout among 1298 Family Physicians Applying for Continuous Certification with the American Board of Family Medicine in 2016*
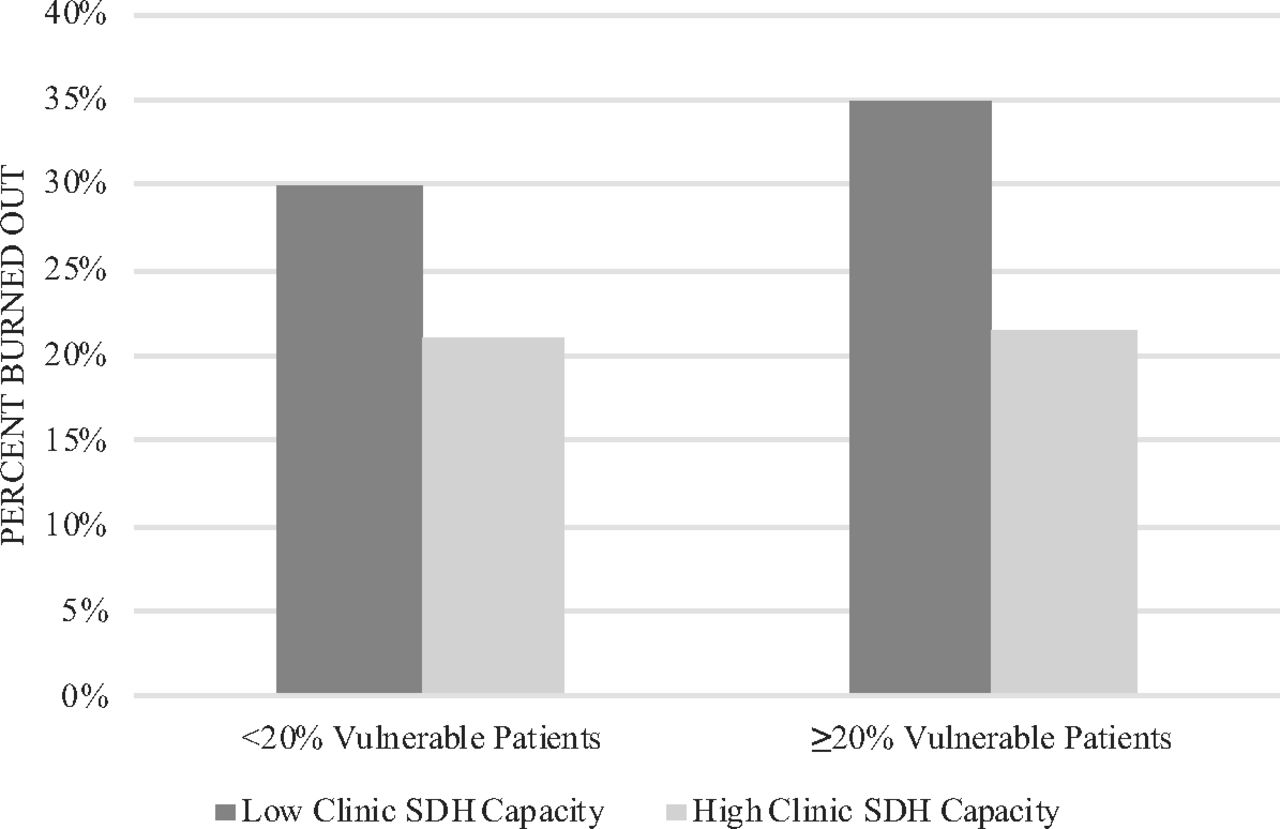
Percentage of family medicine physicians applying for continuous certification with the American Board of Family Medicine in 2016 reporting burn out (n = 351), by level of clinic capacity to address patient's social needs (clinic social determinants of health [SDH] capacity), stratified by vulnerable patient population (z statistic, −0.55, P = .29).
Factors Associated with Perceived Clinic Capacity to Address Patients' Social Needs
In unadjusted analyses, high clinic SDH capacity was more likely to be reported by respondents working at a recognized PCMH (OR, 1.86; 95% CI, 1.44–2.39), a clinic with 20 or more clinicians (OR, 2.03; 95% CI, 1.37–3.02), at an FQHC or similar type practice (OR, 2.24; 95% CI, 1.55–3.25), having over 20% vulnerable patients (OR, 1.39; 95% CI, 1.07–1.80), and by those working in clinics with a social worker (OR, 3.92; 95% CI, 2.89–5.33), a pharmacist (OR, 3.32; 95% CI, 2.48–4.45), behavior specialist (OR, 2.64; 95% CI, 2.02–3.45), or psychiatrist (OR, 3.25; 95% CI, 2.22–4.74). These associations remained statistically significant only for working at a recognized PCMH (OR, 1.65; 95% CI, 1.34–2.21) and working in clinics with a social worker (OR, 2.16; 95% CI, 1.44–3.26) or pharmacist (OR, 1.73; 95% CI, 1.18–2.53), when adjusted for other factors expected to increase clinic SDH capacity (Table 4). None of the factors associated with perceived clinic SDH capacity were themselves associated with burnout (Appendix Table 2). There were no statistically significant interactions between burnout and the factors with significant associations with clinic SDH capacity in predicting clinic SDH capacity.
Bivariate and Multivariable Logistic Analyses between Practice and Physician-Level Characteristics and Perceived Clinic Capacity to Address Patient's Social Needs Among 1298 Family Physicians Applying for Continuous Certification with the American Board of Family Medicine in 2016*
Discussion
This cross-sectional study is the first to include a national sample of family physicians to explore the relationship between physicians' perception of their clinic's ability to address patients' social needs and physician burnout. Given the rapidly expanding interest in ways that the health care sector can engage around SDH,22⇓⇓–25 this study provides important insights into how clinic resources to address social determinants may affect physician well-being.
We found a modest but statistically significant inverse association between perceived clinic capacity to address patients' social needs and burnout. Those reporting a high ability to meet patients' social needs had lower rates of burnout. The association remained significant when adjusting for other factors associated with both burnout and clinic SDH capacity and was true regardless of the percent vulnerable populations served. The inverse association between burnout and clinic SDH capacity was as strong as that between self-reported EHR proficiency and burnout. These findings are consistent with those found in an earlier study of primary care clinicians in San Francisco, CA,18 and with other work describing associations between physician stress and a lack of patient and organization resources.14 This study replicates that earlier work in a larger, national sample, and controls for a wider range of burnout risk factors.
Three practice-level factors were independently associated with physician perception of high clinic SDH capacity: reported presence of a social worker or pharmacist and working in a PCMH. Although these factors were not themselves significantly associated with burnout, association with clinic SDH capacity suggests that they likely influence physicians' work experiences. It is not surprising that physicians who reported having a social worker on staff would report higher capacity to assist patients with social needs. Having a pharmacist can also be instrumental in care coordination,26,27 medication refills and reconciliations, and patient education, all which may be particularly challenging for patients with social complexity. Alternatively, they may free up time for busy clinicians or other staff to more directly attend to patients' social needs. The association between PCMH status and clinic SDH capacity is consistent with PCMH criteria that recognize clinics that provide community resources and linkages to assist patients with health-related social needs.28 These 3 factors, social work and pharmacy availability and PCMH recognition, offer concrete policy or intervention targets for health systems seeking to increase clinic SDH capacity, which may, in turn, contribute to decreased burnout.
In contrast to our original hypothesis, the association between burnout and clinic capacity to address social needs was not limited to physicians working in safety-net practices and caring for relatively high proportions of vulnerable patients. Although there was a trend toward higher burnout in physicians reporting to work at clinics with lower clinic SDH capacity and higher numbers of vulnerable patients, and high clinic SDH capacity appeared to have a greater buffering effect on burnout for physicians working with higher numbers of vulnerable patients, and these findings were not significant. It may be that social needs are ubiquitous among many types of patients or that physicians experience stress from the demands of caring for socially complex patients even when relatively few patients have social needs. Alternatively, although patients seen in safety-net settings are likely to have higher social service needs, physicians working in those settings may have more training and awareness about how to address patients' social needs than physicians working in other settings.
Study Limitations
The study had 3 important limitations. First, the cross-sectional design cannot indicate causality or directionality between clinic SDH capacity and burnout. Greater clinic SDH capacity may protect against physician burnout, but it is also possible that burnout causes physicians to have negative subjective ratings of their workplace, including their perception of clinic SDH capacity. We did test for interactions between burnout and factors associated with clinic SDH capacity (such as availability of social work, onsite pharmacy, and PCMH status) in predicting perceptions of clinic SDH capacity and found none. We believe this finding decreases the possibility that burnout is driving clinicians' perception of clinic SDH capacity. Experimental and longitudinal studies that increase either clinic SDH capacity or burnout resources would provide stronger evidence on causal relationships.
Second, the study relied on data collected during the ABFM continuing certification process, where few questions were asked about clinic attributes and resources. As a result, we are unable to assess other clinic resources that may contribute to clinic SDH capacity. The framing for the survey question about perceived clinic SDH capacity included examples such as “dedicated staff, community programs, resources or tools,” to improve clarity, but the interpretation of social needs and clinic resources could have differed across respondents.29,30 The ability to compare reported responses to objectively measured clinic characteristics and resources would strengthen these findings.
Finally, the ABFM questionnaire did not define “vulnerable patients.” This may have influenced our ability to detect an association between this variable and burnout or perceived clinic SDH capacity. Despite these limitations, our findings provide new insights into potential strategies to reduce physician burnout that could involve augmenting a clinic's capacity to address patients' social needs.
In conclusion, this study, using a large national survey of a representative sample of family physicians, found that physicians who perceive that their clinic has a greater capacity to address patients' social needs are less likely to report burnout. There is still more to learn about what shapes physicians' perceptions of clinic SDH capacity, how that capacity can change over time, and whether addressing it will be an effective strategy to prevent or to decrease burnout. As upstream interventions, including those focused on legal needs, food and housing security, or social support, become more prevalent in the US health care system, it will be useful to assess not only how those programs influence patient health, cost, and utilization but how they may affect physician burnout and retention.
Acknowledgments
The authors would like to thank Bo Fang, PhD, for assisting with data extraction. An earlier version of this work was presented at the North American Primary Care Research Group, 45th Annual Meeting, on November 20th 2017, in Montreal, Quebec.
Appendix
Respondent-Reported Physician and Practice Site Characteristics by Burnout and Perceived Clinic Social Determinants of Health Capacity Among 1298 Family Physicians Applying for Continuous Certification with the American Board of Family Medicine in 2016
Self-Reported Burnout among 1298 Family Physicians Applying for Continuous Certification with the American Board of Family Medicine in 2016: Univariate, Bivariate, and Multivariable Analyses
Univariate, Bivariate, and Multivariable Logistic Analyses Perceived Clinic Capacity to Address Patient's Social Needs among 1298 Family Physicians Applying for Continuous Certification with the American Board of Family Medicine in 2016
Notes
This article was externally peer reviewed.
Funding: This publication was supported by the Hellman Family Foundation UCSF FY 2015–16 and a fellowship training grant by the National Research Service Award (NRSA) T32HP19025. Its contents are solely the responsibility of the authors and do not represent the official views of the Hellman Family Foundation or NRSA.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/32/1/69.full.
- Received for publication April 4, 2018.
- Revision received June 13, 2018.
- Accepted for publication June 15, 2018.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Scoping review of social workers professional roles in primary care
- Predictors of burnout among US healthcare providers: a systematic review
- Mise en œuvre dinterventions sociales en soins de sante primaires
- Implementing social interventions in primary care
- Lower Likelihood of Burnout Among Family Physicians From Underrepresented Racial-Ethnic Groups
- Provider Impacts of Socioeconomic Risk Screening and Referral Programs: A Scoping Review
- Team Configurations, Efficiency, and Family Physician Burnout
- Capacity to Address Social Needs Affects Primary Care Clinician Burnout
- Re: Physician Burnout and Higher Clinic Capacity to Address Patients' Social Needs
- A Longitudinal Study of Trends in Burnout During Primary Care Transformation
- Celebrating the exceptional potential of general practice
- Conversations, Communication and Counseling Are Key Family Medicine Tactics to Improve Patient Health
- The American Board of Family Medicine's Data Collection Method for Tracking Their Specialty