
Abstract
Direct Primary Care (DPC), where patients pay a fee to a primary care provider to obtain access to services, is a delivery model that has received notable attention and enthusiasm from some providers. Proponents of DPC believe that the model increases accessibility, reduces overhead, and ultimately improves care for patients; however, there is little evidence in the peer-reviewed literature to support these claims. The objective of this analysis was to apply Starfield's adaptation of Donabedian's Structure-Process-Outcome conceptual model to evaluate primary care to formally display the links between potential changes in clinical structure and processes from DPC adoption. Based on existing literature on the constructs in Starfield's model, expectations of DPC's impact at the patient, clinic, and system levels were defined. DPC uses changes to financing and the population eligible to trigger potential gains in continuity and accessibility to subsequently improve care processes. There is evidence to support DPC as a theoretically sound approach to improve attributes of primary care, such as first contact care and longitudinality at the clinic level for participating patients. At the health system level, DPC has low-construct validity that would suggest a positive impact on the potentially eligible population's health due to membership fees that exclude patients who are more likely to be vulnerable and complex than patients who are willing and able to stay in the practice. Descriptive and comparative research of included and excluded patients is needed to inform providers, patients, and policy makers of the DPC's ability to attain the attributes of primary care and ultimately achieve better outcomes over alternative primary care delivery and financing models. Meanwhile, theoretic application informed by years of research on primary care provide insight as to what changes to expect and to monitor as practices consider DPC adoption.
Direct Primary Care (DPC) is a model of primary care delivery that has been dubbed “membership medicine,” where patients pay a periodic membership fee to a primary care provider (PCP) to obtain access to services.1 A review of 116 DPC practices found that average fees were $77.38 per month.2 Although no definitive range of periodic-fee-covered services exists, it typically includes evaluations, check-ups, and basic services in the primary care office setting; however, some include office-based laboratory or radiology tests,3 whereas other DPC practices charge an additional per visit copay.2 In an effort to simplify their financing and administrative burden, DPCs do not bill third parties.
The DPC model and other forms of membership medicine can be traced back to pre–Civil War US medicine. At that time, some physicians were retained by a family or group of individuals to provide all necessary care.4 These arrangements were referred to as “contract practice,” but were disliked by doctors as they bore a considerable amount of risk (comparable to the role of modern health insurers) that patients would use their services beyond what was covered by the fixed fee.4 Today, it is dissatisfaction with the burden of working with insurers and the pressure to see a high volume of patients that has drawn the interest of primary care physicians to the DPC model.3,5 By one count, there are currently at least 723 DPC practice locations in 48 states.6 A survey conducted by the American Academy of Family Practice found that 2% of respondents reported practicing in a DPC model, with another 7% considering a move to DPC in the future.7
Although DPC has received increased attention and enthusiasm from some providers, only one descriptive analysis has been published in the peer-reviewed literature,2 resulting in a dearth of information to inform providers, patients, and policy makers on the effects of DPC adoption. Proponents of DPC hail a number of benefits for both providers and patients.5,8 Adoption of the DPC model typically involves a reduction in patient panel size, allowing for longer appointments. DPC providers are also able to reduce their administrative costs and burden by not working with health insurers.2 By pushing health insurance out of the relationship, any patient may seek care from the DPC provider, so long as they are willing to pay the membership fee. Finally, DPC providers tout that they offer enhanced access through more timely appointments, phone and email interaction, and home visits.
The empirical literature has yet to quantify these features at a broad level; however, a 2005 survey of 231 primary care retainer physicians found that they had significantly smaller panel sizes (898 versus 2303) and were more likely to offer each of 6 special services (accompanied specialist visits, house calls, 24-hour access, same-day appointments, coordinated hospital care, and private waiting rooms) compared with nonretainer physicians.9 In summary, our knowledge of the effects of DPC is based on provider surveys, case studies, and interviews, while robust evidence on access, use, quality, and outcomes are lacking to inform providers and stakeholders.
Researchers and primary care experts have done little to consider how the DPC model fits within existing theories of primary care and, thus, what can be expected to change under DPC in a clinic's structure, processes, and outcomes for various populations. In the absence of evidence, it is valuable to apply existing theories to models of care to potential outcomes, unintended consequences, and system-level implications. Barbara Starfield adapted Donabedian's “Structure-Process-Outcome” conceptual model to evaluate the attainment of the 4 attributes of primary care: first contact care, longitudinality, comprehensiveness, and coordination.10 By assessing each construct in Starfield's model for a given approach to primary care delivery, formal links between practice characteristics and outcomes can be inferred. I apply Starfield's model to DPC to formally display the links between structural and procedural changes in DPC, identify potential changes in outcomes and the attainment of the attributes of primary care, and place DPC within the context of the US health care system.
DPC Adoption and Changes to Structure, Process, and Outcomes
Structure
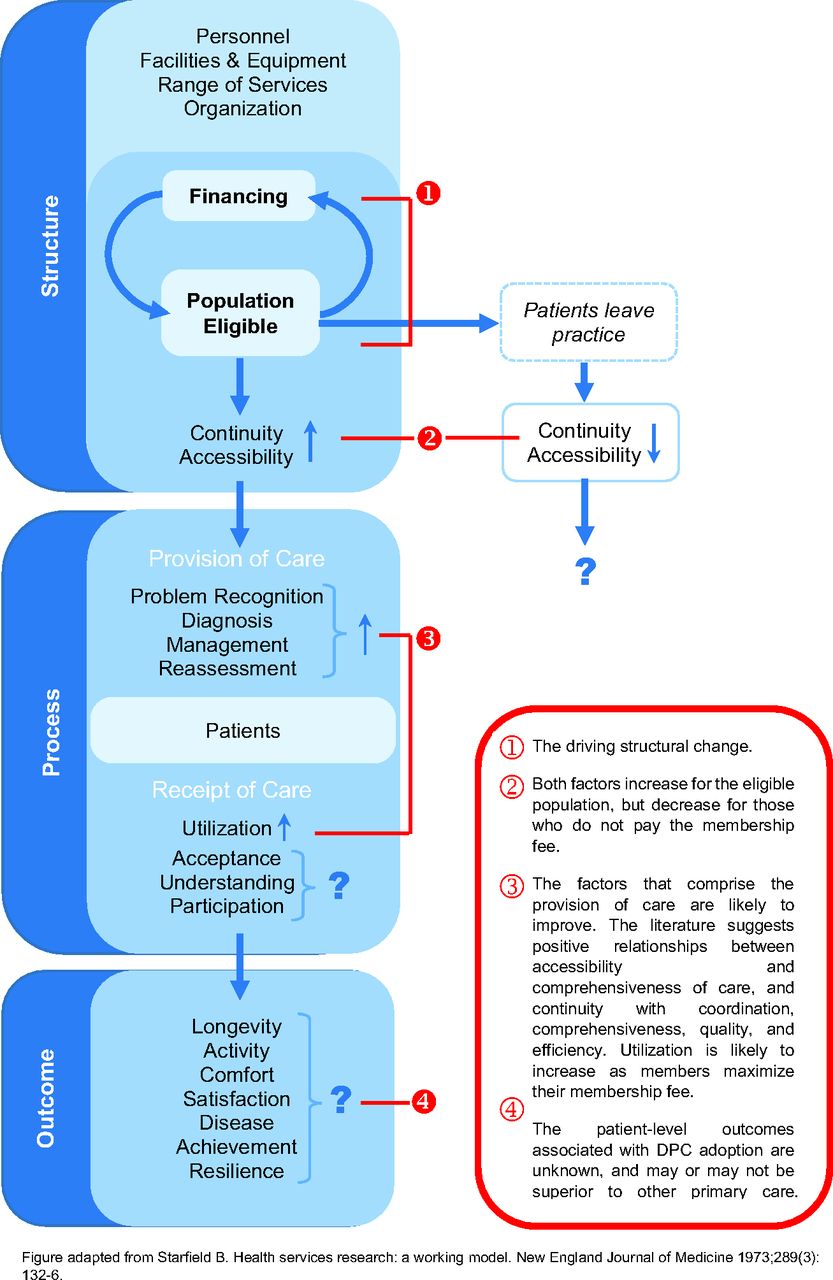
As illustrated in Figure 1, an adaptation of Starfield's model shows how DPC adoption may change structural characteristics of the practice to trigger process-based improvements. In Starfield's model, primary care structure includes the financing, population eligible to be served by the practice (ie, local patients in need of primary care), continuity, accessibility, personnel, facilities and equipment, range of services, and organization. DPC adoption directly modifies financing and the eligible population served by the practice and can be considered the driving structural change of the model (point 1 in Figure 1). This structural change consequently affects accessibility and continuity (point 2 in Figure 1). Adopters become less reliant on traditional fee-for-service financing through membership payments. This presents the physician with increased flexibility to provide services in ways that are desirable for patients but were not previously billable, such as phone consultations, email correspondence, and home visits, generally at no additional charge apart from the membership fee. This ultimately improves accessibility for the eligible population, while likely decreasing access for the potentially eligible population (ie, the local population in need of primary care who cannot/will not pay the membership fee). With the introduction of the membership fee, continuity will likely increase as patients seek to maximize the utility of their subscription and providers offer greater access, leaving patients little reason to receive care from multiple PCPs. The change in financing also detaches any influence insurers may have had on the practice through pay-for-performance, prior authorization, and value-based purchasing policies.

Effects of Direct Primary Care Adoption on Health Services System Components. DPC, Direct Primary Care.
The volume of the eligible population decreases in DPC practices and works as the other driving structural change with varying effects. Previous research suggests negative associations between large panel sizes or patient-load with access11, continuity,12 and quality, as measured by rates of recommended preventive screenings13 and patient perceptions of quality care14. Conversely, membership fees affect accessibility as a barrier to those unable or unwilling to make monthly payments for primary care. Many physicians who practice in DPC models have argued that it is incorrect to assume that the remaining eligible population is systematically less vulnerable both physically and financially5,15⇓⇓–18; however, the assertion that DPC patients are representative of the socioeconomic and health status of a given community has not been demonstrated. For example, Alexander and colleagues' survey9 found that retainer physicians reported an average panel proportion of Medicaid-enrolled patients of 5.0% compared with 15.3% among nonretainer physicians. Overall, the introduction of the membership fee financing mechanism changes the eligible population, and these 2 constructs (financing and the eligible population) together are used to increase continuity and accessibility for patients who pay the fee.
Process
Starfield categorized processes by the provision and receipt of care. Based on the structural changes discussed above, evidence suggests that all 4 provision of care constructs (problem recognition, diagnosis, management, and reassessment) could improve through better accessibility and continuity (point 3 in Figure 1). A literature review conducted by Kringos et al19 found a large field of research on access and its positive impact on processes of care, including continuity, comprehensiveness, and quality of care. The same review found evidence for a positive relationship between continuity and processes, such as coordination, comprehensiveness, quality, and efficiency.19 Another literature review also found access to primary care services to be associated with equity in health; however, in the presence of membership fees, it is questionable whether DPC would introduce the same effect.20 Although DPC may improve many care processes, provider methods for managing risk of overuse of their services (eg, referrals to specialists, limiting the volume of complex patients) must be monitored because of the inherent financial incentives of the model.
Given the potential improvements in access and continuity, it is plausible that the way participating patients receive care would change as well. Primary care use among the eligible population would likely increase relative to what it would have been without a membership fee, as patients seek to put their subscription to use. For example, retainer physicians have reported greater patient use of same-day appointments than nonretainer physicians offering the same service.9 Other forms of use may decrease, as continuity has been found to be associated with lower hospitalization rates21⇓–23 and emergency department visits24⇓–26. It is unclear whether the remaining 3 process constructs (acceptance, understanding, and participation) would change under DPC. Moreover, it would be valuable to determine if patients who pay the membership fee understand and participate in their care to a greater degree before being served by the DPC relative to those patients who do not participate in the model.
Outcome
A critical question is whether DPC improves outcomes relative to other models of primary care delivery (point 4 in Figure 1). Patient satisfaction is likely to be high within DPC practices, and high continuity has been found to be positively correlated with satisfaction23; however, measuring such a change in satisfaction among DPC adopters would be confounded as the membership fee effectively excludes patients who are less than highly satisfied with their care. Improved continuity and accessibility are associated with outcomes such as lower hospitalization rates and cost19, but whether these structural and procedural improvements under DPC are to the degree where measurable gains in outcomes are experienced is unknown. Other models of primary care delivery, such as the patient-centered medical home, involve forms of structural and procedural changes but have thus far resulted in a mix of positive, small, and no significant changes in outcomes, such as acute care use, quality metrics, and cost.27⇓⇓⇓⇓⇓⇓⇓–35 Given this, it should be expected that any significant and clinically meaningful improvements in outcomes delivered by DPC providers could be restricted to the attributes of longitudinality and first contact care and may be no better than existing alternatives of primary care delivery reform. Furthermore, a prepost analysis of DPC adoption may discover an overall negative impact on outcomes. If all patients are included at baseline (ie, pre–DPC adoption), it will include a number of patients who decide not to pay the membership fee and who will then need to change providers and experience a disruption in their continuity of care.
In summary, the constructs in Starfield's model with the best theoretic case for change under DPC are financing, the eligible population, improved continuity, and increased accessibility. As the model relates to the 4 attributes of primary care, it is theoretically sound to expect that DPC adoption is associated with greater attainment of first contact care and longitudinality for participating patients.
DPC within the Context of the US Health Care System
Adoption of the DPC model places providers in a unique position within the greater context of the US health care system. For those practices that do not bill third party payers, this transition seems to be one toward isolation from the health care system. By not engaging with insurers, these providers would not participate in pay-for-performance, accountable care organizations (ACO), or episode-based or global payments; some of the largest payer initiatives in the past 25 years. Whether the exclusion from these policies or the detachment from insurers decrease integration of care between DPC and other providers is unknown.
DPC providers attempt to improve the primary care they deliver through changes to access and financing that they apparently are otherwise unable to create. Whether this financing model is sustainable is unknown and dependent on the specific practice and patient panel. Recent research on primary care financing based on a survey of practice-level financial data has estimated the median gross annual revenue from fee-for-service payments at approximately $487,000 per full-time physician36; however, the confidence interval for this figure ranged from $205,231 to $955,765, demonstrating extensive variability among primary care practices. The impact of DPC adoption on practice structural and procedural expenses may be straightforward to estimate, whereas projecting a monthly membership fee that a sufficient number of patients would be willing to pay involves more uncertainty.
There are other financing policies that could improve access without excluding a portion of the patient population. Similar to membership fees, per member per month payments are used in Primary Care Case Management and patient-centered medical home programs, which both aim, in part, to improve primary care access. Mixed payment approaches that include a capitation and fee-for-service element may reduce the likelihood of under or over provision of services in primary care37 and have resulted in the delivery of fewer services than under fee-for-service in other health systems but with more time allotted per visit.38 Broader system initiatives such as ACO formation39,40 may also improve access and financing at the primary care level in various ways. The distinguishing characteristic between DPC and these other policies is the control the PCP maintains as payers and other providers do not impact the structure of DPC. Whether that characteristic results in better outcomes and greater efficiency compared with other reforms is of great interest.
A significant concern regarding the adoption of DPC is the impact on the potentially eligible population and, thus, the model's impact at the system level.41 Any improvements introduced by DPC adoption will only be experienced by patients who pay the membership fee. As shown in Figure 1, individuals in the potentially eligible population may be negatively affected through a disruption in continuity and accessibility if the patient was served by the DPC adopter and can/will not pay the membership fee. Because the barrier is financial, the concern is greatest for low-income populations, complicating the system-level effect of DPC adoption.
Conclusion
The need for rigorous research on the DPC model is great. The American College of Physicians has made such a call, beginning with the most basic descriptive patient and provider variables.41 Information on participating patient demographics before and after DPC adoption is required to understand the population that is served by DPC and the broader implications for excluded patients. Research on the patterns of DPC location and socioeconomic context would also provide a better understanding of DPC's niche. Following these descriptive analyses, the focus must shift toward outcomes and the attainment of the 4 attributes of primary care, with comparisons between DPCs and other models of primary care. Although this research will encounter obstacles, such as the absence of claims data for DPC practices, it is essential to guide providers, patients, and policy makers toward high-quality primary care.
Meanwhile, theoretic application informed by years of research on primary care provides insight as to what changes to expect and to monitor as practices consider DPC adoption. By applying Starfield's conceptual model, an understanding of the potential changes to structures, processes, and outcomes for the patient population can be achieved while policy makers and providers await rigorous research on DPC. Evidence exists to support DPC as a theoretically sound approach to attaining the attributes of first contact care and longitudinality for participating patients. DPC uses changes to financing and the population eligible to trigger these potential improvements. At the health system level, DPC has low-construct validity to support a positive impact on the potentially eligible population. By limiting access to those willing and able to pay the membership fee, a vulnerable population will almost certainly be excluded. A model that does not meet the needs of a vulnerable population is unlikely to have a significant impact on the overall costs and outcomes of the US health care system. Other policies and models to address primary care financing and accessibility that do not exclude groups of patients exist and may or may not be superior to DPC. DPC's distinguishing characteristic from these other models is that the control rests with the PCP and is not dependent on financing from third-party payers.
Acknowledgments
The author would like to acknowledge Megan C. Tulikangas, MPP, for her assistance in the visual presentation of Figure 1 in this article.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/31/4/605.full.
- Received for publication May 29, 2017.
- Revision received January 2, 2018.
- Accepted for publication January 5, 2018.




{kind=link}