
Abstract
Purpose: Direct primary care (DPC) critics are concerned that the periodic fee precludes participation from vulnerable populations. The purpose is to describe the demographics and appointments of a, now closed, academic DPC clinic and determine whether there are differences in vulnerability between census tracts with and without any clinic patients.
Methods: We linked geocoded data from the DPC’s electronic health record with the social vulnerability index (SVI). To characterize users, we described their age, sex, language, membership, diagnoses, and appointments. Descriptive statistics included frequencies, proportions or medians, and interquartile ranges. To determine differences in SVI, we calculated a localized SVI percentile within Harris County. A t test assuming equal variances and Mann-Whitney U Tests were used to assess differences in SVI and all other census variables, respectively, between those tracts with and without any clinic patients.
Results: We included 322 patients and 772 appointments. Patients were seen an average of 2.4 times and were predominantly female (58.4%). More than a third (37.3%) spoke Spanish. There was a mean of 3.68 ICD-10 codes per patient. Census tracts in which DPC patients lived had significantly higher SVI scores (ie, more vulnerable) than tracts where no DPC clinic patients resided (median, 0.60 vs 0.47, p-value < 0.05).
Conclusion: This academic DPC clinic cared for individuals living in vulnerable census tracts relative to those tracts without any clinic patients. The clinic, unfortunately, closed due to multiple obstacles. Nevertheless, this finding counters the perception that DPC clinics primarily draw from affluent neighborhoods.
Introduction
More than half of family physicians report at least 1 symptom of burnout.1,2 With administrative burdens, physicians have less time with patients, leading to a vicious cycle of exhaustion and depersonalization.3⇓–5 To combat these trends, physicians have embraced direct primary care (DPC), a model which charges a periodic fee, does not bill third parties, and includes per-visit charges that are less than the monthly periodic fee.6 As a result, DPC practices have smaller panels, lower overhead costs, and longer appointments.7,8 Working outside the insurance system, some clinics offer discounted labs and medications, making these services affordable.9 In theory, these modifications support the functions of primary care (first contact, coordination, comprehensiveness, and continuity), and limited evidence suggests the model improves access, promotes continuity, and reduces emergency department visits.8,10⇓–12
Despite these benefits, challenges impede greater adoption. For example, data regarding the model’s impact on quality are lacking.13 While advocates contend that longer appointments facilitate high-quality care, critics argue these practices have few incentives to track quality.13 Even though DPC practices do not accept insurance, patients may still need coverage for emergency and hospital care. Furthermore, DPC patients struggle to see specialists.10 The dramatically lower panel sizes (approximately 500) raise concerns about the impact of DPC on workforce shortages though some argue that the model will facilitate the recruitment and retention of primary care physicians.8,14 Finally, many worry that the periodic fee is a barrier to low-income patients.7,15 Some concerns result from the conflation between DPC and concierge medicine, the latter of which caters to high-income patients and accepts payments from insurance.16 While the vestiges of this confusion persist, there is evidence that DPC practices are a viable option for all, including low-income populations. For example, Qliance, a DPC practice in Seattle, included uninsured and unemployed individuals,17 and another DPC practice reported high rates of stress, isolation, unemployment, and uninsurance among their patients, countering the prevailing stereotype.18 Unfortunately, little is known about the sustainability of DPC practices, generally, and those that cater to the uninsured, specifically, highlighting the need for data.
Houston offers a unique backdrop for exploring the viability of DPC for low-income individuals. Houston is a majority-minority city, where nearly 1 in 4 are born outside the US.19 Access to health care is poor, in part, because the state did not expand Medicaid. In 2019, the uninsured rate in Harris County was 22.4%, higher than that for Texas and the US.20 Furthermore, Houston suffers from a primary care shortage, with the ratio of residents to primary care physicians (1709:1) exceeding the national average (1319:1).20 To address these challenges, the University of Houston (UH) launched the Tilman J. Fertitta Family College of Medicine (TJFFCOM), which has a mission to produce primary care physicians for the region.21 In support of that mission, TJFFCOM developed a DPC clinic, 1 of the few DPC clinics operated by an academic institution.22 Given concerns regarding the periodic fee, it is unclear whether low-income patients would join a DPC clinic, the clinic would serve vulnerable communities, and this model within this context would be financially viable. To that end, the objectives of this study are to describe the demographics of the patients (age, sex, language, and diagnoses) of the UH DPC clinic, describe the number, type, and length of appointments, and determine whether census tracts with at least 1 patient demonstrated greater vulnerability than those census tracts without any.
Method
This study provides a descriptive analysis of UH DPC patients. The analysis includes all patients seen in the clinic from its launch in November 2021 through June 2022 and is approved as nonhuman subjects research by the UH Institutional Review Board (#00003540).
Sample
The sample was identified by linking the individual- and appointment-level records in 2 tables stored in the clinic’s electronic health record (EHR) (Elation Health; San Francisco, CA). Individual-level descriptives of the clinic patient population were pulled from a cleaned, deduplicated version of the Demographics table in the EHR and further narrowed to remove sample patients and any entries without a corresponding appointment record. Analysis of clinic appointments included all entries in the Appointments table, excluding nonappointment events (eg, holds for breaks), canceled appointments, and no shows.
Measures
Patients were characterized using available demographic information: age, sex, language spoken, month of first enrollment, and diagnostic codes, both individually and grouped into the World Health Organization’s (WHO) ICD-10 block categories at the patient and appointment levels.23 Appointments were characterized using available information about the type of visit, scheduled visit duration, mode of visit (video telemedicine vs in-person), and month in which the appointment took place. We also calculated the number of active and canceled memberships by month. Members were defined as those who paid the periodic fee in a given month. Diagnostic codes were summarized both per clinic patient and at the WHO block category per appointment (Table 3). Social vulnerability (SVI) is a geographic index that summarizes multiple social dimensions including: 1) socioeconomic status, 2) household characteristics, 3) racial and ethnic minority statuses, and 4) housing type and transportation. SVI data are publicly available from the Centers for Disease Control and Prevention-Agency for Toxic Substances and Disease Registry.24 However, a modified, localized version of the SVI was developed for Harris County.
Statistical Analysis
Descriptive statistics, including frequencies and proportions or medians and interquartile ranges, were calculated to characterize the demographics, appointment features, and clinical characteristics. All analysis was conducted in STATA (v17, Stata Inc.; College Station, TX).
Mapping Patient Distribution and Vulnerability
To capture the difference in census tract SVIs at the county level, we calculated the SVIs for Harris County census tracts (786 tracts with majority of the area inside county borders using 2020 census data). Using a shapefile and the 2020 version of census-tract level SVI scores, statewide data were filtered for Harris County. Since the publicly available percentile scores for SVI are based on index scores compared against a national distribution, a localized SVI percentile was needed to order index scores within Harris County. Then, overall SVI was calculated as the overall percentile ranking within the county across the sums of item-percentile rankings within each SVI domain.24
Localized SVI values were linked to the patients’ census tracts and SVI data using a HIPAA-compliant geocoding API tool (Geocod.io, Dotsquare LLC; Norfolk, VA) to aggregate the addresses of patients into their associated census tract Federal Information Processing Standard (FIPS) codes. The census tract FIPS codes were then used to mark the tracts in Harris County with at least 1 patient and to match the calculated localized SVI values for them. Localized SVI values and presence or absence of DPC patients in each tract were exported to ArcGIS Pro (v3.1.0, Esri Inc; Redlands, CA) to generate maps. A t test assuming equal variances and Mann-Whitney U Tests were used to assess differences in SVI and all other census variables, respectively, between those tracts with and without any patients.
Results
Individual clinic patient data were pulled from a cleaned, deduplicated (n = 199 duplicates) version of the Demographics table (Appendix Figure 1). The data were further cleaned to remove demographic entries with no appointment record (n = 431) and sample patients (n = 1) to yield 322 unique patient records. Appointments were identified from the 1276 entries in the Appointments table occurring during the observation period. After all nonappointment events (n = 76), canceled appointments (n = 229), and no shows (n = 196) were excluded, there were 775 appointments completed. An additional 3 (3) appointments were documented in the DPC clinic EHR but flagged as occurring at another TJFFCOM clinic site, resulting in 772 DPC appointments for use in this analysis.
Patient Population and Appointments
Patients were seen in the clinic an average of 2.4 times. Females made up 58.4% of the patients and the median age was 45.5 (IQR = 35 to 55). The most frequent age-group was 40 to 49 (comprising 26.7% of patients) followed by 50 to 59 (25.2%). More than a third of the patients spoke Spanish as their first language (37.3%). Nearly 5% of visits were conducted via video and 15% of clinic visits were scheduled for a full hour, with approximately half (51.0%) scheduled for a more standard 20-minute visit (Table 1).
Demographic Characteristics of Users of the Direct Primary Care Clinic
Diagnoses
The mean number of ICD-10 codes assigned per visit was 1.08 (median = 1, standard deviation (SD) = 0.29; range = {1 to 3}) (Table 2). Across all visits, there was a mean of 3.68 (median = 3, SD = 2.28; range = {1 to 14}) unique ICD-10 codes assigned per patient. The 2 most frequent diagnoses were essential hypertension (I10) (39% of patients), and obesity (E66.0-0.9) (38%). This was followed by hyperlipidemia (E75.8) at 28% (Table 2). In examining the diagnoses by block category, 39% of all appointments were assigned codes for “Endocrine, nutritional, and metabolic diseases” (Table 3).
Summary of ICD-10 Diagnosis Code Descriptions (4% Prevalence or Higher)
Summary of ICD-10 Block Categories
Geographic Distribution
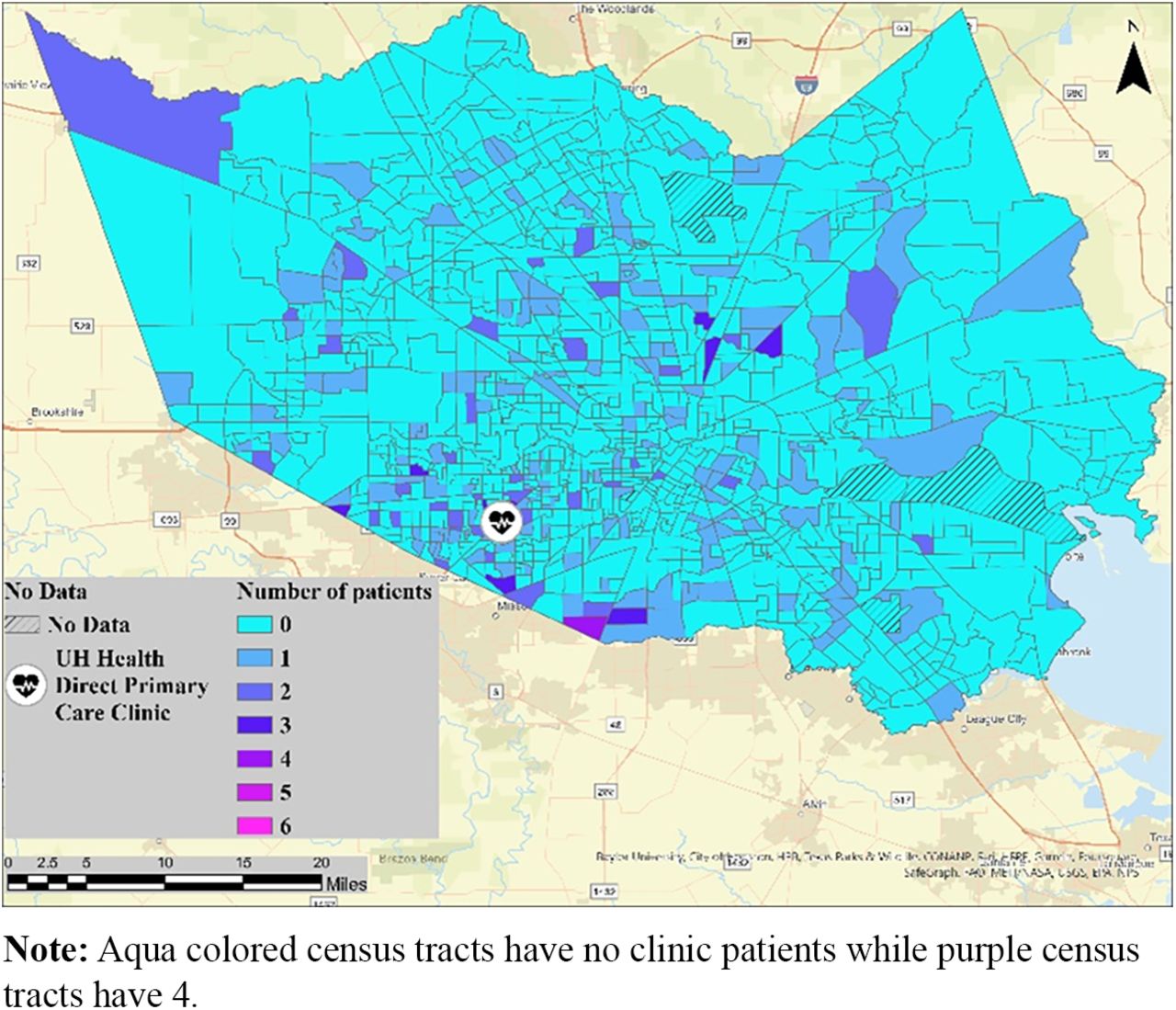
The clinic demonstrated a broad geographic (Figure 1) footprint, with patients residing in census tracts throughout Harris County (25% (200/786) of all census tracts). Furthermore, the census tracts in which DPC patients lived had significantly higher SVI scores (ie, more vulnerable) than tracts where no DPC clinic patients resided (P < .05; Table 4 and Figures 2 and 3). Figure 2 depicts the localized SVI overlayed with the tracts containing at least 1 patient to the clinic shaded. The majority of such tracts are located in areas with higher SVI values indicating the clinic provided care to more vulnerable census tracts. For further clarity of the correlation between SVI and memberships in the clinic, a bivariate visualization technique was used to show both the number of patients per census tract and the localized SVI values (Figure 2).

Count of patients across Harris County census tracts.

The calculated localized Social Vulnerability Index for Harris County census tracts overlayed with the tracts with at least 1 patient to the clinic.

Bivariate visualization of the number of patients per census tracts and the calculated localized Social Vulnerability Index values.
Social Vulnerability Index Components for Census Tracts With and Without Patients
Total Memberships through June 2022
By the end of June 2022, the total number of active memberships was 183 while the total canceled memberships were 123. The peak number of active memberships was 200 in April of 2022 (Table 5).
Memberships and Office Visits through June 2022
Discussion
We found that census tracts with at least 1 DPC clinic patient demonstrated greater vulnerability compared with those census tracts without any. This finding counters the prevailing belief that DPC practices cater exclusively to high-income patients. The patient base was diverse with over a third speaking Spanish, a finding that mirrors the rest of Harris County.25 This finding is important as this population has historically been difficult to reach due to structural barriers and discriminatory practices.26,27 Because of the model, physicians had more scheduled time with patients. Nearly half (49%) of the visits were scheduled for 30 minutes or longer, almost double the national average (18 minutes) for primary care.28 In cities with high uninsured rates, our data suggest that individuals from low-income neighborhoods will access care through this model. Furthermore, the census tracts were broadly distributed and accounted for 25% (200/786) of all census tracts within the county, with some traveling over 35 miles. For context, Harris County spans 1707 square miles, a total area that exceeds the state of Rhode Island. Census tracts with any patients demonstrated a higher percentage of households without vehicles compared with those census tracts without patients (Table 4). This highlights that uninsured individuals in Houston are willing to travel to access affordable primary care and suggests that more access points are needed. Once registered, patients demonstrated high utilization in the short-term, averaging 2.4 visits. Annualized, these figures translate to 3.6 visits per year. By comparison, older Americans average 2 to 3 primary care visits per year.29 Consistent with primary care nationally, patients sought care to address chronic diseases, indicating that the DPC was more than an urgent care center, but rather, a home where chronic conditions were managed.29
Lessons Learned
Unfortunately, in November of 2022, the DPC clinic closed after memberships fell, suffering the same fate as Qliance which closed in 2017.30 While the clinic attracted the target population, the model, as implemented, was not sustainable for several reasons. First, while the clinic attracted low-income individuals, it did not enroll enough to break even. There were contextual factors that affected the clinic’s financial status, including historic inflation, COVID-19, and the loss of the anchoring physician. Inflation, in particular, increased the cost of all goods and services, leaving patients with less money for health care. Anecdotally, our staff reported that nearly one-third of those cancelling memberships were unable to consistently afford the fees. While the clinic was unable to sign up enough patients, the break-even point, approximately 800 active memberships, was also influenced by the staffing model. To ensure the clinic had adequate staff, it hired 3 clinic staff, which is higher than the average (1 staff) for DPC clinics.8
Second, the amount and structure of the membership fee played a role in the clinic’s sustainability. While the amount ($60) is consistent with other DPC clinics (where fees range from $65 to $85 for adults), it may have been too high for low-income individuals.8 A lower monthly fee may have attracted more patients but would also have increased the panel size needed to break even. Because of the target population, the clinic was intentional about how the monthly fee was paid. For example, while patients agreed to pay the monthly fee for 12 months and had to provide a 30-day notice for termination, they could end the contract without penalty, and there was neither a waiting period to resume the subscription nor a re-enrollment fee. Internal records demonstrate that 17% canceled their subscriptions. By comparison, 74% of DPC practices report that less than 10% terminate their membership after a year.8 Those who lacked credit cards paid in cash, making it difficult to receive payments during the intervening months. Due to University policies regarding banking and security, the patient-facing functionality of the membership management platform could not be used; therefore, patients could not enroll in the program, make appointments, pay bills, or set up recurring payments online. The end result was that some patients paid only when they needed care. In contrast, DPC clinics rely on payments that are automatically received regardless of utilization.
Finally, effective partnerships are crucial and elusive. For example, employers can provide referrals and income. One study found that two-thirds of DPC practices have employer-based contracts.8 Despite considerable effort, the clinic was unable to secure these arrangements. Partners can also provide discounted services typically covered by insurance, including specialty care, labs, imaging, and prescription medications. The literature indicates that the cost of these services, in addition to the amount of the periodic fee, have a strong effect on the utilization, both appropriate and inappropriate.31,32 While the clinic acquired these partnerships, they were not implemented as envisioned, in part, because the partners were unable to adapt their work flows to the needs of uninsured patients. Taken together, all these factors contributed to the level of patient churn that made the clinic unsustainable.
Limitations
There are several limitations. First, the data on race is incomplete, which limits our ability to comprehensively describe our patients. While this field was available in the EHR, it was inconsistently captured, and patients could decline to answer. Second, we did not assess important other measures, including quality of life, disease control, access to care, and utilization. These measures could provide an alternative perspective on the impact of the DPC clinic. Third, we used ICD-10 codes that were assigned during visits. Because insurance is not billed, these codes may not reflect the breadth of issues discussed. Finally, for the geospatial analysis, we only included those census tracts in Harris County. While there were patients from adjacent counties, we chose to exclude them so that the comparison group (census tracts in Harris County without patients) would be more clearly defined.
Conclusion
An academic institution launched a DPC clinic to address the needs of low-income, uninsured individuals. Patients used the clinic frequently and sought care for chronic, and not just acute, conditions. The clinic ultimately closed because of external factors like inflation, COVID-19, and a failure to secure synergistic partnerships, like employer-based contracts. Nevertheless, we found that patients from vulnerable neighborhoods wanted to receive services from this model. If arranged differently, we hypothesize that other DPC clinics could successfully serve low-income populations. Specifically, these DPC clinics should monitor the amount and structure of the monthly fee, minimize staffing, and identify aligned partners that can provide a source of referrals or offer affordable services. To advance our knowledge in this field, DPC clinics that have already overcome these barriers should partner with researchers to measure the extent to which their practices are reaching low-income populations.
Appendix.

Patient and appointment flow diagram.
Acknowledgments
We would like to acknowledge Paule Anne Lewis who was instrumental in launching the clinic and providing data.
Notes
This article was externally peer reviewed.
Funding: This work is supported by the Cullen Foundation.
Conflict of interest: University of Houston contracted with Elation. Please note that the opinions of Dr. Olaisen do not reflect the opinion of his employer, the Agency for Healthcare Research and Quality.
To see this article online, please go to: http://jabfm.org/content/37/3/455.full.
- Received for publication September 21, 2023.
- Revision received December 10, 2023.
- Accepted for publication January 2, 2024.




{kind=link}
{kind=link}
{kind=link}
{kind=link}