
Abstract
Introduction: It is unknown what patients in primary care with mild-to-moderate chronic kidney disease (CKD) know, think, and feel about their diagnoses and how they value the information provided. The aim of the study was to explore their knowledge, thoughts, and experiences concerning their CKD and the information given to them.
Method: Qualitative interview study with patients with mild-to-moderate CKD who know their diagnoses and are treated mainly by family physicians.
Results: Four themes arose: CKD literacy, coping with anxiety, prerequisites for self-management, and reciprocity in information provision. The participants filled deficiencies in their CKD knowledge with misconceptions and half-truth about causes, symptoms, and treatment. The anxiety about CKD at the time of diagnosis versus the feeling of irrelevance later on was due to the absence of CKD symptoms and their physicians' minimization of the seriousness of CKD. Participants failed to connect lifestyle and cardiovascular disease with CKD. Not all participants were well informed about the consequences that CKD might have. CKD literacy and willingness to change were both necessary to accept lifestyle changes. Further, the participants felt that it would be helpful when information comes with empathy and is tailored to patients' personal needs.
Conclusions: Patients have various perceptions about their CKD. Exploring these perceptions could help match their needs with better-tailored information. Doctors should be aware that they can deliver inaccurate signals about CKD severity, so that patients fail to realize the potential impact of CKD. This makes them less open to lifestyle changes and improving their self-management.
- Chronic Kidney Diseases
- Family Physicians
- Life Style
- Primary Health Care
- Qualitative Research
- Self-Management
Most patients with chronic kidney disease (CKD) in stages 1 to 3 are treated in primary care.1 The prevalence of CKD is 10% to 12% and is expected to increase due to aging and rising incidences of hypertension and diabetes.2 Nearly all interventions for patients with CKD in primary care aim to prevent cardiovascular complications and progression to end-stage renal disease. Not only the treatment of hypertension and diabetes, but also lifestyle changes such as smoking cessation, exercise, weight loss, low salt intake, and medication management are important. These measures rely extensively on patient self-management. The prerequisites for self-management are patient awareness of the diagnosis and education, and the firm belief that the patient's role and willingness to make lifestyle changes is important.3 Tailored education in primary care is the key to achieving self-management. However, previous research shows that family physicians and practice nurses encounter barriers when informing patients about the diagnosis of CKD,4 and quantitative studies confirm the low awareness of the diagnosis among patients with mild-to-moderate CKD.5,6 Patients have little specific knowledge about causes, kidney function, treatment, and nephrotoxic medication.7,8 Despite research into the information and educational needs of patients with severe CKD, research relating to patients with mild-to-moderate CKD is scarce.9,10 To enhance self-management and knowledge, we must first explore what patients know, think, and feel about their disease and about the provided information. Therefore, the aim of this study was to explore patients' knowledge, thoughts, and feelings about CKD, as well as their experiences with the information provision for patients with mild-to-moderate CKD in primary care.
Method
Study Design
We conducted in-depth interviews with patients with CKD. We considered this design appropriate for our exploratory research question. We used the consolidated criteria for reporting qualitative health research checklist as a reporting structure.11
Participant Selection
Physicians from 8 practices, associated with the primary care network of practice-based research in Nijmegen, the Netherlands12,13, recruited patients by phone or e-mail, based on recent consultation or on a sampling from the problem lists, pointing at kidney failure. The inclusion criteria were CKD stages 1 to 3, being informed about the CKD diagnosis, speaking the Dutch language, and CKD management based mainly in primary care. We used a purposive strategy for sampling. After the first 10 patients, we asked the physicians to recruit patients with specific characteristics, characteristics that were not yet represented in the participants who had already been interviewed. We aimed for variety in the categories: age, sex, CKD cause, estimated glomerular filtration rate, duration of the diagnosis, and education level. The participant sampling, data collection, and analysis were organized in an iterative process. The physicians asked 25 patients to participate. Two patients were excluded because they had been diagnosed with severe CKD (stages 4 and 5). One married couple was recruited. We decided to interview only 1 of them because they likely shared the same knowledge and ideas. One patient refused to participate because he felt misinformed about the type of research. The study population comprised 21 patients (see Table 1 for participants characteristics). Patients were first informed by their family physician by a letter. Further information was provided by the researcher (CvD) before the participants signed for informed consent. The interviews were conducted between December 2015 and August 2016.
Demographic Information about the Participants
Data Collection
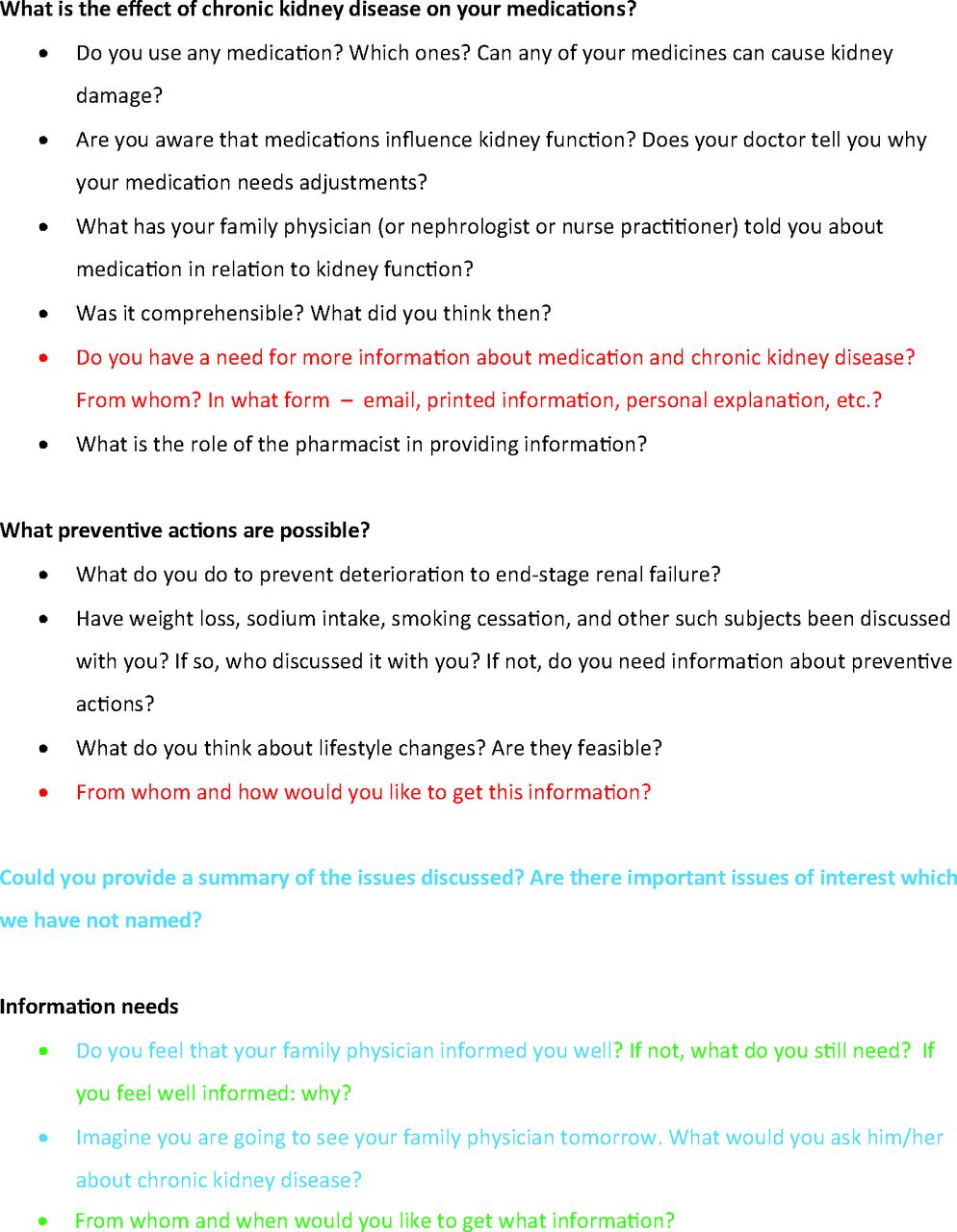
We developed an interview guide (Appendix A) based on the literature. This interview guide was pilot-tested on 2 participants who were members of the Dutch Kidney Patient Association. The guide was adjusted after each 3 to 7 interviews, with the use of new insights from the previous interviews and discussion in the research team (for adjustments, see Appendix A). The interviews with the participants took place at their homes or in the practices. The interviewer was an MD and PhD student and trained in qualitative research (CvD, female). She had no connection with the participants. The interviews lasted 30 to 80 minutes. All interviews were audiotaped and transcribed verbatim. The transcripts were returned to the participants for a member check. Three participants reported corrections in the transcripts: 2 nuanced their statements and 1 reported grammatical errors. The analysis of the 21st interview produced no new codes or concepts. We concluded that saturation had been reached.
Data Analysis
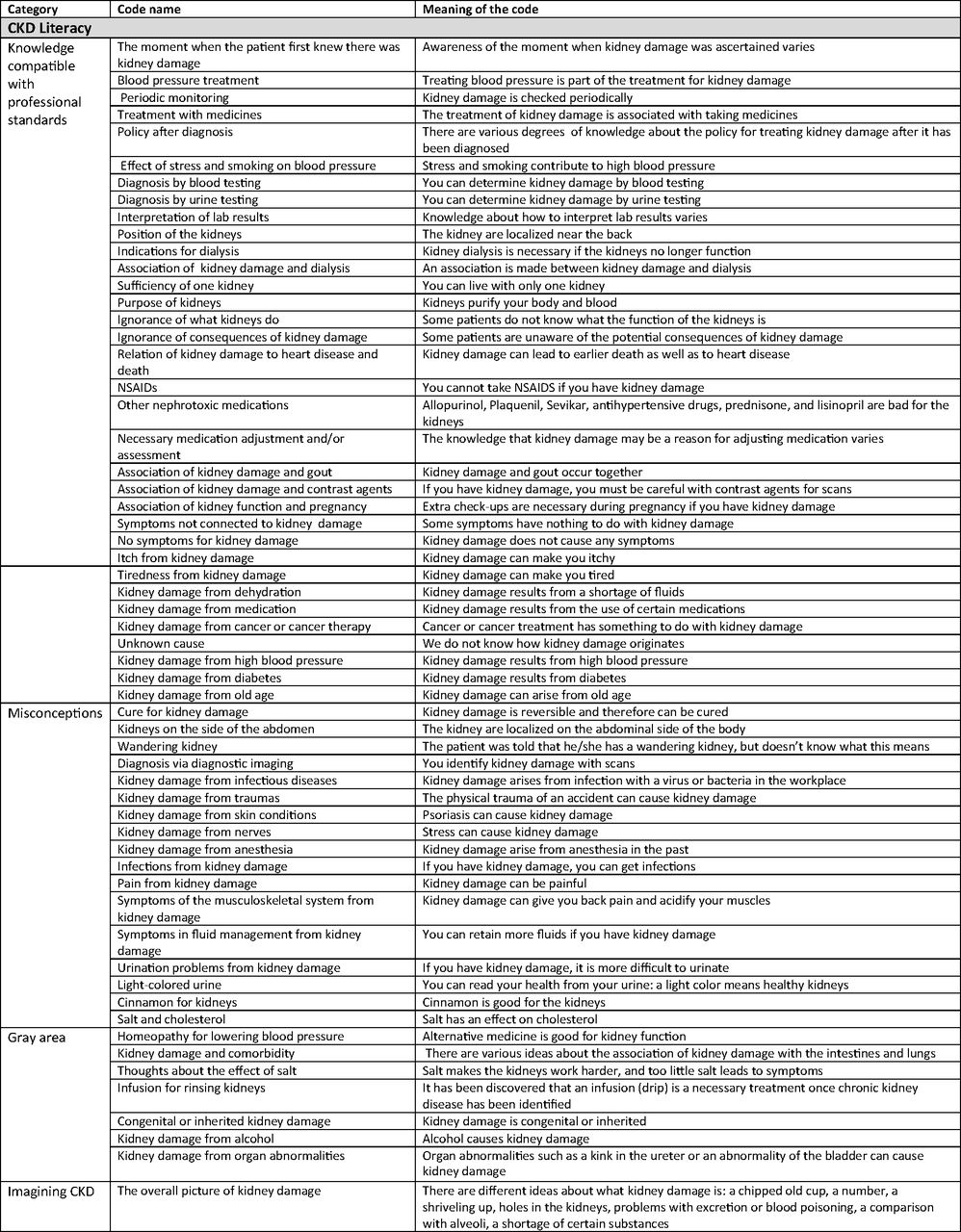
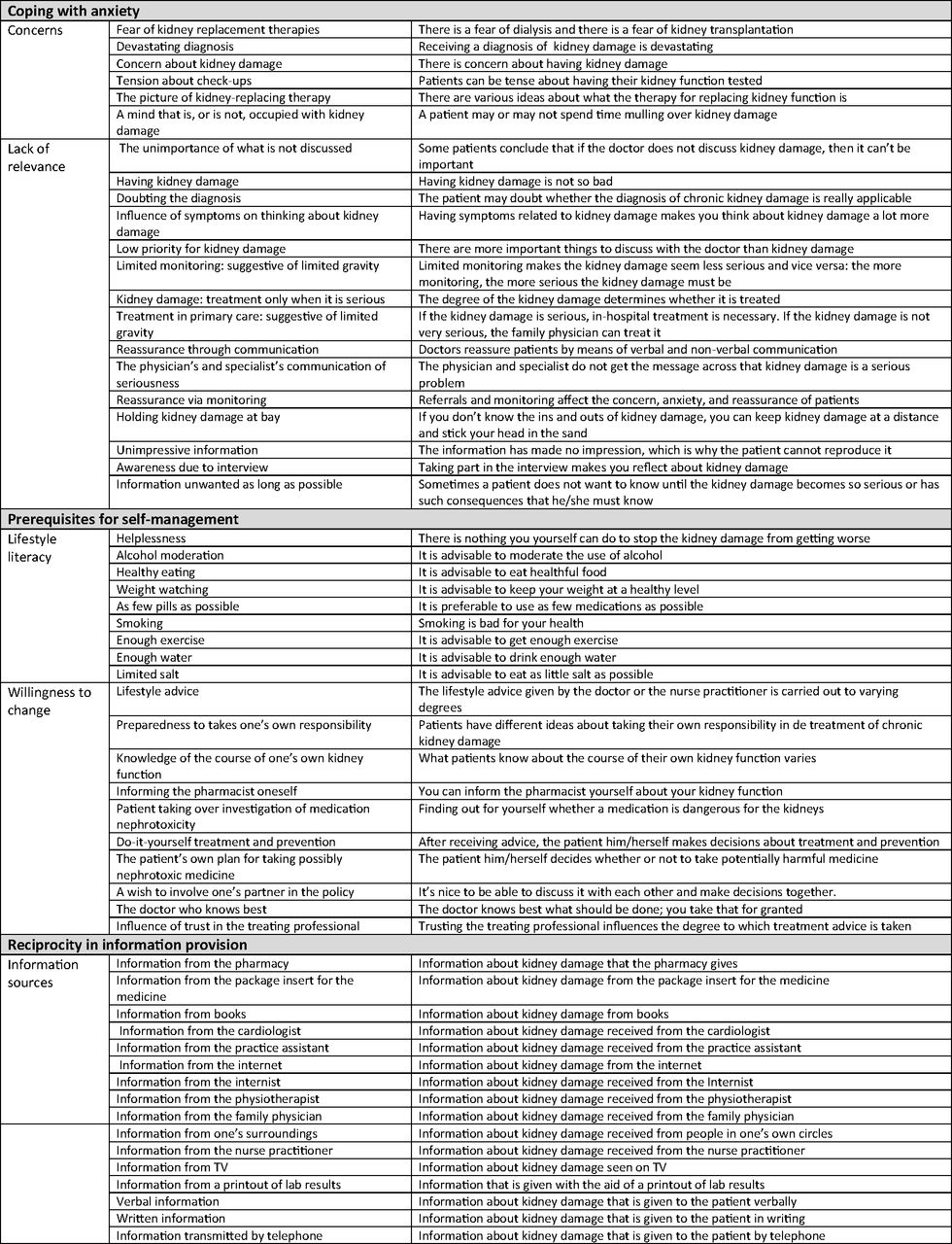
We used the technique of constant comparative analysis. This approach is part of the grounded theory in which concepts emerge as theory is formed.14 Analysis started after the first interview. The analysts (CvD and MD) coded inductively and independently by using Atlas.ti (version 7.1.5). They discussed, merged, and renamed codes after the 3rd, 10th, 16th, and 21st interviews. CD and MD sorted the preliminary findings into categories and themes. The codes, categories, and themes were constantly compared with the transcripts.15 After saturation, the research team (CvD, MD, WdG, and NS) discussed all codes, categories, and themes. Five consensus meetings were needed to construct the final thematic map (Appendix B). A native-English speaker translated the illustrative quotes.
Results
Overview
Four main themes emerged from the interviews: CKD literacy, coping with anxiety, prerequisites for self-management, and reciprocity in information provision. All themes are illustrated by multiple categories and quotes.
CKD Literacy
We found that patients complete their knowledge gaps with misconceptions, half-truths, and distortion of facts to create their own image about CKD and all what comes with CKD.
Imagining CKD
The information obtained from the interviews showed that CKD is an unclear concept. A broad spectrum of ideas and views appeared when the interviewees were asked for a definition: a shriveled kidney, a number in the computer, blood poisoning, or a shortage of blood substances.
“… that I had a kidney that you could compare with a pottery cup with all kinds of cracks in it. Say just an old cup. That is what my kidney was like.” (participant 5 [P5])
Knowledge Compatible with Professional Standards
Knowledge that corresponded with professional knowledge varied among the interviewed patients. Most patients knew that the kidneys are located in the abdomen and have something to do with the purification of blood. It was less commonly known that CKD is associated with cardiovascular disease. A variety of CKD causes were mentioned: aging, medication, dehydration, and chemotherapy, but despite that, most participants did not link CKD to their hypertension or diabetes. If they knew hypertension or diabetes causes CKD, it was still difficult to imagine how CKD related to vascular damage.
“But at my doctor's, there was the idea that high blood pressure has an influence, that high blood pressure attacks the organs.” (P6)
The participants rightly linked CKD to pregnancy issues, gout, and problems with contrast agents. Fatigue and itch were mentioned as symptoms. Others experienced no symptoms or were not sure whether their symptoms were related to CKD. It was clear that CKD needs periodic follow-up, including blood and urine examination, to monitor kidney function. Treatment was mainly associated with taking medication. It proved difficult to say which drugs are involved in CKD management and what the effects of the medication should be. However, there was an awareness of medication warnings in case of renal impairment, for example, for nonsteroidal anti-inflammatory drugs, gout medication, and antihypertensive agents.
Misconceptions
Many misconceptions came forward, probably as a result of lack of knowledge. Could kidney damage be caused by stress, narcosis, car accidents, viruses, and bacteria, or was it a side-effect of psoriasis?
“I have an idea that it has something to do with this.” (Points to a psoriasis spot) (P3)
Another source of misconception was speculation about symptoms. Pain, edema, myalgia, infections, and urinary symptoms were considered symptoms of CKD.
“Yes, I know that it can be very painful if something's wrong with your kidneys; my father had that too. And then it is difficult to urinate, and so on.” (P14)
There were various thoughts about diagnostics. There was the conviction that CKD can only be made visible by a body scan, because a scan was made at diagnosis. Furthermore, there was the idea that the color of the urine reflects health.
“You can see your health in your urine. You just see it yourself – then you have much darker urine.” (P6)
It was reported that cinnamon affects CKD positively. Others were convinced that CKD does not require treatment at all. The patients did not always realize that CKD is a life-long illness, and they thought that CKD was curable.
Gray Area
Some notions were difficult to categorize as true or false. For example, the role of genetics in kidney damage: there might be a genetic predisposition, but that probably did not affect the pathogenesis.
“… and then I have to say that my mother also had a weak kidney. So it is also in the genes.” (P6)
Other unclear items were whether kidney damage is caused by alcohol and organ abnormalities.
“I have always taken a stiff drink, and that can cause kidney damage.” (P23)
Treatment with an infusion of water to flush the kidneys is unnecessary for CKD, but is very important for acute prerenal failure and protection against contrast agents.
Coping with Anxiety
A first reaction of patients being labeled with CKD was fear and doom-thinking about the future. To cope with fear, the participants gathered several signals to minimize seriousness.
Concerns
Some participants were shocked when they received the results of their blood tests. They worried and imagined dialysis or kidney transplantation. Follow-up was stressful to them.
“My kidney function was not good. It was only 60% or so. So yes, that was certainly scary, and I did worry about it for a while.” (P10)
Lack of Relevance
The anxiety at the time of diagnosis contrasted sharply with the perception that CKD is not a serious condition. Doubts about the importance of the diagnosis increased over time. One patient even refused to be labeled as having CKD. Other participants had no symptoms related to the decline of renal function, so it was difficult to imagine that the CKD was serious.
“Yes, I have no trouble with it, so I will not worry about it.” (P11)
The participants' perceptions were influenced by the fact that the physicians seemed unconcerned about the diagnosis: they trivialized patients' concerns verbally, judged a referral to a nephrologist unnecessary, or did not explicitly treat the CKD.
“You think that it is not that important. It is stable, so that is good, and now and then it must be checked. Something like that.” (P9)
The interviewees paid little attention to CKD and the physicians' explanation about it. This led to thoughts of a lack of relevance and priority.
“So then I saw another doctor, who did not talk about kidneys at all. So I assume that they are okay.” (P25)
Some participants recognized their own responsibility regarding CKD. They admitted that they neglected their CKD by not seeking further information.
“And I did not ask anything else about it, because, well, if it does not yet exist, I do not have to know about it!” (P19)
Prerequisites for Self-Management
Participants mentioned 2 factors that are important for living a healthier life: knowledge about the potential effects of lifestyle on CKD and willingness to change. These factors are strongly connected to each other and both are required to actually change lifestyle.
Lifestyle Literacy
Various lifestyle interventions for preventing cardiovascular events and kidney deterioration were mentioned during the interviews: weight control, smoking cessation, sodium restriction, physical exercise, and preventing dehydration. The participants knew about lifestyle in relation to their hypertension or diabetes, but did not realize the positive effects of lifestyle changes on kidney function.
“I do realize that my blood pressure is too high, that I haven't got my cholesterol right, that I am overweight, that I have to keep working on it and pay attention to it all. But I never made the connection that it affects the kidneys.” (P17)
Willingness to Change
Notions about lifestyle changes differed among the participants. Most were motivated to adjust their lifestyle, but 1 patient argued:
“… it is all very well for them to say that it is this way and you must do such and such. But people do not do it. And I do not either. And that is why I say it does not help.” (P23)
A proactive attitude toward renal decline and medication problems was also discussed. Behavior varied from taking total control to waiting for the doctor to come along.
“As soon as it is under 40 again, I will make it clear that something's wrong or ask for a consultation.” (P19)
Reciprocity in Information Provision
Patients gathered CKD knowledge from various professionals and had different views on the tasks of professionals involved in CKD care. Patients indicated that it helps when information comes with empathy and is tailored to patients' personal needs.
Information Sources
Many medical coworkers were involved in informing patients: physicians, their assistants, practice nurses, nephrologists, cardiologists, pharmacists, and even a physiotherapist. Most information was given verbally, although some participants received written information. The internet was the source that was preferred.
Views on Professional Tasks
There was a general satisfaction about the care received from the physicians and nurse practitioners, although doubts about their knowledge were reported.
Empathy
Empathy from the physicians was important. The participants judged a friendly approach as very important. They wanted the physicians to accept their treatment preferences and provide timely information. One patient did not feel free to ask questions:
“I myself know nothing and it scares me a little. He told me that my kidney function was not all that great. Then I am someone who does not open his mouth, yes. ” (P10)
Tailored Information
The participants reported knowledge deficits. Not all felt well informed and reported that physicians did not spend enough time on detailed explanation. Other participants could not remember the information.
“The doctor has neither the time nor the energy to explain it that way.” (P16)
“I was informed, but not well informed.” (P20)
A number of questions remained. For example, it was confusing for patients to find that CKD has several synonyms that were used interchangeably: “renal impairment” and “kidney failure.” The interviewees wondered about the difference. Patients expected their physicians to tailor the information.
“We do not want too many medical terms because we do not understand them. It is never been my field of work.” (P1)
Discussion
Summary of Main Findings
Four main themes emerged from the interviews: CKD literacy, coping with anxiety, prerequisites for self-management, and reciprocity in information provision. Patients had deficiencies in their CKD knowledge so that misconceptions arose about causes, symptoms, and prognosis. There was a discrepancy between the anxiety at diagnosis and the later feeling of irrelevance of CKD. Lack of CKD symptoms and physicians' attitudes reduced the sense of seriousness. The patients failed to associate lifestyle and cardiovascular disease with CKD. Some were willing to make lifestyle changes. Not all were well informed about the consequences that CKD might have. The participants express the need for tailored information.
Comparison with Existing Literature
Several qualitative and quantitative studies6,12,13 found that patients have little objective and perceived knowledge in all stages of CKD. This is in line with our study. We were surprised that there were so many misconceptions about CKD—why and when do misconceptions arise? Some studies show the health care professionals' difficulties with CKD management and education.16,17 Limited professional knowledge and lack of prioritization18 may contribute to knowledge gaps and misconceptions. Furthermore, our study uncovered problems at the level of the doctor-patient communication. The information physicians provide needs improvement. The current literature shows a low baseline understanding of kidneys and CKD19 among patients. The lack of understandable and uniform CKD information may be a contributing factor.20 Other studies report that patients remember little of what they have been told.21
It is questionable whether patients are ready to learn when they receive signals that make them doubt the severity of CKD. The participants stated that physicians not talking much about CKD is one such signal. Other signals were judging a referral to a nephrologist unnecessary and seeming not to actually treat the CKD. The lack of symptoms is another signal for patients that CKD is not a serious condition. These signals form what we call the “relevance discrepancy.” The participants were worried at time of diagnosis, but later they trivialized their disease. Anxious patients avoid information gathering, consciously or unconsciously. Another study described this same phenomenon among patients with progressive renal failure in regard to education about transplantation and donation.22
Other researchers have identified themes that should be assessed in self-management interventions.23 We confirm that, from the patients' perspectives, disease-specific knowledge is one of the crucial themes. Contantini and colleagues24 describe the need for disease-specific information, tailored and focused on the situation of the individual patient. Our findings are consistent with this research. It seems obvious, but given the findings in our study, disease-specific information remains an important point that demands attention.
Strengths and Limitations
It is a strength that CvD and MD established internal validity with independent coding, used Atlas.ti, and conducted mind-mapping sessions with the research team in which additional perspectives and interpretation of analysis and findings were discussed. The iterative approach of the interviews and the interim data analysis assured the rigor of the data. Another strength is that we included patients with heterogeneous characteristics to collect a broad range of knowledge, feelings, and experiences. These broad outcomes enabled us to take conclusions for this specific population. A limitation is that we did not interview patients with African, Asian, or Latin origin. We cannot comment on how patients with non-white origin experience and understand CKD and the impact on lifestyle. Given the clear outcomes in our white population, we cannot exclude that the problems we found also occur in the non-white population. It is important to do additional research on this. All interviews took place in Dutch. We tried to limit the loss of nuance by having a native-English speaker translate representative quotations. One interviewer did all the interviews; we tried to lower the risk of interview bias by providing feedback on the interview style. We asked physicians to recruit informed patients. The study could be biased toward inclusion of better-informed patients, but the results show that these potentially well-informed patients also have knowledge caps, misconceptions, or are not able to link CKD to lifestyle changes.
Implications for Practice
The patients lack information about the cause, symptoms, and treatment of CKD. Clear information can reduce the occurrence of misconceptions. The patients do not recognize the link between CKD and cardiovascular risk and lifestyle. It is important to include CKD in cardiovascular information and link lifestyle changes to their positive effects on both cardiovascular disease and CKD. This link might increase patient willingness to make lifestyle changes. Practice nurses can provide important help in this process.25 Repeating the message without dilution helps encourage a healthier lifestyle and makes patients realize how to influence CKD. Patients want tailored information. To deliver tailored information, there is a need for providers to be aware of patients' perspectives about CKD first, not only at diagnosis, but also during treatment. Uniform patient information on the internet or in an article is helpful and useful.
Conclusion
Patients' knowledge of CKD is deficient. There is a discrepancy between the patients' concerned attitude at time of diagnosis and their sense of irrelevance later in the disease. Physicians should be aware that they, often unknowingly, deliver the wrong signals about the severity of CKD, which influences patient behavior toward lifestyle and willingness to enhance self-management. If physicians want to provide tailored and patient-centered information, they need to be aware that misconceptions and perceptions of CKD should be actively identified and addressed.
Acknowledgments
We thank all the participating CKD patients for their contribution.


Appendix B. Final thematic map



Notes
This article was externally peer reviewed.
Funding: The Dutch Kidney Foundation funded the study, grant 13A4D302.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/31/4/570.full.
- Received for publication December 13, 2017.
- Revision received March 29, 2018.
- Accepted for publication March 30, 2018.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}