
Abstract
Background: The closure of obstetrics (OB) units at rural hospitals is thought to have implications for access to prenatal care (PNC) and infant mortality rate (IMR). The objective of this study was to determine whether local availability of PNC and OB services, specifically as provided by family physicians (FPs), would be associated with a lower IMR in 1 rural Alabama county.
Methods: Data from 1986 to 2013 from Pickens County was compared with data from 2 sets of control counties: Clarke/Monroe (full OB care) and Coosa/Conecuh (no local OB care).
Results: From 1986 to 1991 (no local OB services; period 1), Pickens County's IMR was 17.9, which fell to 7.2 from 1993 to 2001 (with local services; period 2). After the county's OB unit closed, IMR rose to 16.0 from 2005 to 2013 (period 3). In Clarke/Monroe (continuous OB service), the IMR fell from 14.5 to 9.9 from period 1 to period 3. Coosa/Conecuh (no OB service) exhibited a consistent IMR ranging from 10.9 to 14.4.
Conclusion: OB services provided by FPs in Pickens County resulted in improvement of the county's IMR. Local PNC was associated with a lower IMR.
Infant mortality rate (IMR), defined as the number of deaths among infants <1 year of age per 1000 live births in a given geographical area during a year (based on county of maternal residence), has been used as a sensitive proxy measure of population health. The correlation of IMR with the overall health of a given population suggests an association between various causes of infant mortality and other determinants of health, such as economic development, social well-being, and the overall quality of the environment.1
Despite a declining national IMR (from 6.9 in 2005 to 6.0 in 2013; a decline of 13.1%), Alabama's IMR has exhibited less improvement, down 9.3 to 8.7 (a decline of 7.5%).2 In 2013 Alabama was ranked 49th in the nation for infant mortality.2 Although many potentially unquantifiable factors contribute to poor perinatal outcomes, the closure of labor and delivery units at many rural hospitals in the United States is believed to have implications for access to prenatal care and infant mortality. A nationwide study found that 179 rural counties had lost hospital-based obstetrics (OB) services between 2004 and 2014, and this resulted in an increase in out-of-hospital births, births in a hospital without an OB unit, and preterm births during the year after loss of services.3
Because Alabama is largely rural, the closure of such units has particular implications for the state. Between 2010 to 2014, 7.2% of rural US hospitals surveyed had closed their OB units.4 These units were more likely to be small and located in communities with low family incomes. The pool of providers in a community influences a hospital's ability to provide OB services, and rural communities have few total providers as well as few providers of OB care. Although the reasons cited for OB unit closures include low birth volume and low reimbursement related to a high proportion of Medicaid-insured births, the most commonly cited reasons involve staffing difficulties, including recruitment and retention of obstetricians.4,5 In addition to the financial implications of low annual birth volume, several providers surveyed cited difficulty maintaining competencies among providers and staff given the low volume of in-hospital births.4,6
More than 28 million women of reproductive age (18 to 44 years) live in rural areas in the United States,7 though obstetricians/gynecologists (OB/GYNs) tend to practice in urban areas.5 In fact, in 2008, only 6.4% of OB/GYNs in the United States practiced in a rural setting. In many rural areas, family physicians (FPs) provide 100% of OB care.8
FPs have historically provided access to OB care for a disproportionate share of underserved communities, both rural and urban. Cohen and Coco9 assert that FPs are more likely than obstetricians to provide prenatal care to women who are younger, live in rural areas, or have Medicaid insurance. In communities where hospitals no longer operate OB units, FPs' broad scope of practice allows them to continue working within the community, potentially offering local prenatal care. Two studies have demonstrated a significant correlation between a lack of local FPs and OB unit closures.5,10
Despite the benefits of FPs providing OB services, the number of FPs incorporating OB into their practices has declined.6,9,10 The American Academy of Family Physicians reports that in 2016, only 19% of responding FPs performed deliveries, compared with roughly 40% in 1986.11,12 Likewise, the number of FPs who perform cesarean deliveries has decreased steadily, with only 9.3% performing cesarean deliveries either independently or in consultation with an OB/GYN.11
Previous studies have investigated the role of OB unit closures on perinatal outcomes.6,13⇓⇓⇓–17 Longer travel time to a delivery facility has repeatedly been associated with poor maternal and infant outcomes. Ravelli and associates14 demonstrated an increased risk of adverse outcomes for women living in the Netherlands when travel time from home to a hospital at the onset of labor met or exceeded just 20 minutes. In the United States, women living in rural communities lacking OB units need to travel an average of 29 miles to reach the nearest hospital that provides OB services.4 In Alabama, >30% of women live more than a 30-minute drive from the nearest hospital that provides maternity and nursery care.18 Prolonged travel times to hospitals with OB units can result in significant delays in presentation to the hospital following the onset of labor, preventing early intervention in the event of labor complications or increasing the risk of an unplanned out-of-hospital birth.6,19 In addition, travel to receive OB care is associated with greater risk of complications, higher costs, and longer length of hospital stay.8,15 In rural areas, which often have low mean household incomes, this travel burden falls disproportionately on socioeconomically vulnerable women and families. In such populations, lack of transportation, especially across long distances, further impedes access to care and subjects these women to high rates of induced labor, for logistical reasons.13
Other studies have attempted to examine the link between improved IMR in rural communities and OB care provided by FPs.9,20 These have suggested that such care can contribute to a significant reduction in IMR within a given community.
Pickens County, Alabama, is one such rural community, which has benefitted from OB care provided by FPs. From 1986 to 1991, OB services were unavailable in the county. In 1992, 2 family physicians—1 of whom was trained through an OB fellowship—established OB services in Pickens County, performing both cesarean and operative vaginal deliveries. The local hospital provided equipment and staffing for low-risk maternal and infant care, while a regional hospital, located 38 miles away, was available to care for mothers with high-risk pregnancies and infants, and to perform deliveries. Providers in Pickens County maintained a good working relationship with this regional medical center throughout the study period, and transports were easily arranged. From 1993 to 2001, Pickens County residents had local access to full-time prenatal care and local deliveries. In 2002 the local hospital suspended delivery services when the 2 providers left the area. Between 2002 and late 2004 limited prenatal services were provided by an outreach clinic staffed by physicians from the regional medical center.
In late 2004, following the completion of a 1-year OB fellowship, 1 family physician began practice in the community and from 2005 to 2013 provided local prenatal care while performing deliveries at the same regional hospital. No other OB providers, including midwives, operated within the county, and midwifery was not permissible by Alabama state law during any of the 3 study periods.
This study seeks to take advantage of a “natural experiment” that occurred in Pickens County involving varying states of availability of OB services to determine whether closure of the local OB unit would be associated with an increased IMR despite continued access to local, full-time prenatal care.
Methods
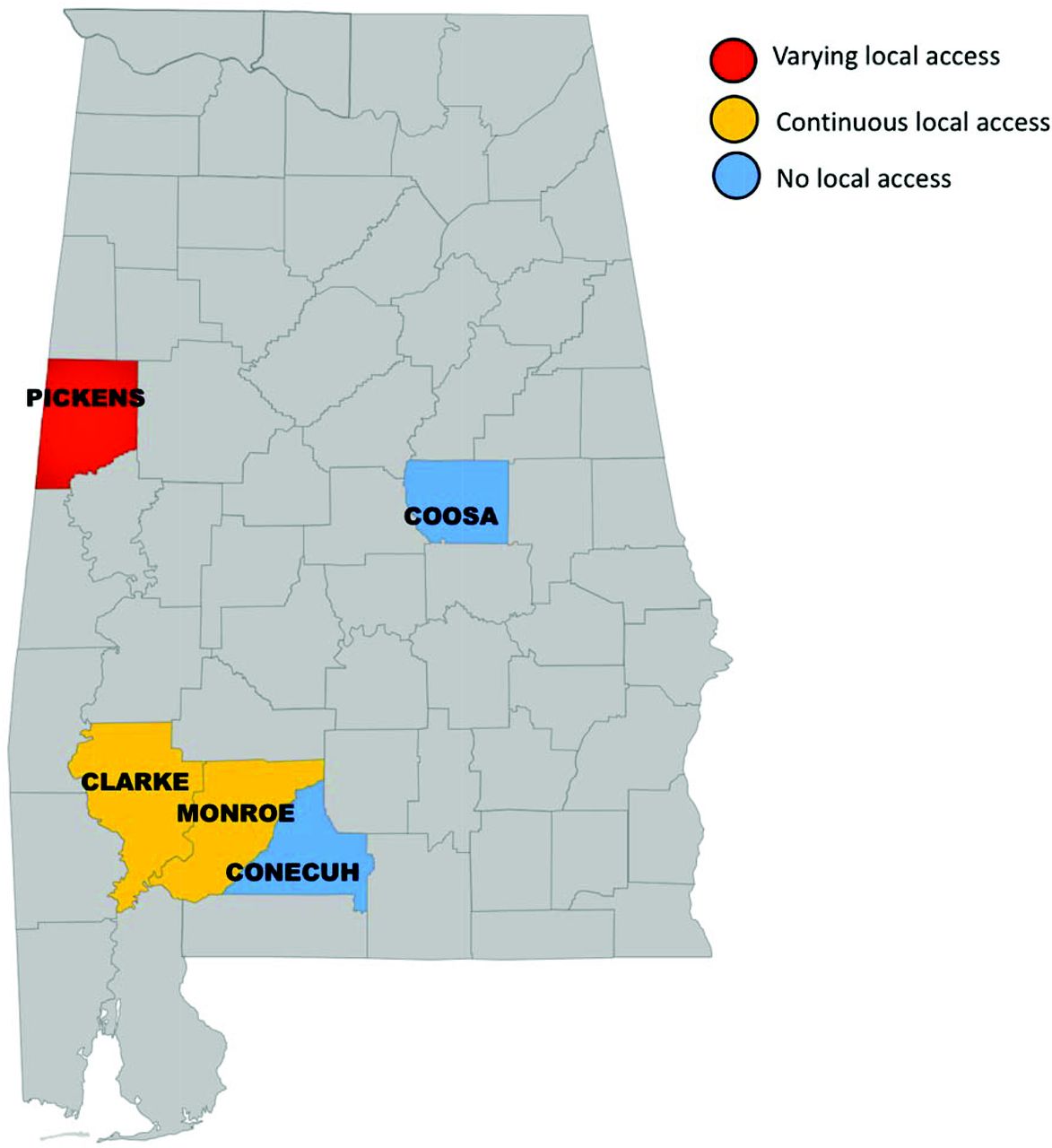
The main county of interest was Pickens County, Alabama. No OB services, including prenatal care, were available in the country from 1986 to 1991. Then, from 1993 to 2002, full OB services, including prenatal care and delivery services, were available. In 2002, the county lost labor and delivery services, and from 2005 to 2013, only (full-time) prenatal care was available. Because 1992 and the years from 2002 to 2004 were periods of transition in service availability, these years were excluded from the study. Rural counties in Alabama demographically most similar to Pickens County then were evaluated for comparison on the basis of models previously described in the literature.21⇓–23 Each of the counties was relatively similar with respect to rurality, percentage minority population, and poverty level, as indicated by the percentage of Medicaid-eligible residents.24 Availability of OB services in these counties was also contrasted. OB care was not provided in Coosa and Conecuh Counties from 1986 to 2013, whereas Clarke and Monroe Counties maintained OB services availability throughout the entire study period. These 2 pairs of counties were used as controls (see the map in Figure 1). For added context, corresponding data for the state of Alabama were also considered, and demographic data are presented in Table 1. For the purposes of this study, 3 sample periods were established based on the availability of OB services in Pickens County; these are detailed in Table 2.

Map of Alabama Counties.
Periods 1, 2, and 3 as Determined by Obstetrics Services Availability in Pickens County
Alabama Department of Public Health infant mortality data2 were used to compare the total death rates among infants in each county. Because of the known relation to infant mortality, rate of infants born with a low birth weight (LBW) and percentage of births to females aged 10 to 19 years were considered descriptively to determine their potential respective contributions to the change in IMR in each county throughout the study period.
Cumulative numbers of total births, infant deaths, LBW births, and births to women aged 10 to 19 years were determined for each county across time periods. After each county was studied individually, the data from Clarke and Monroe Counties were pooled, as were the data from Coosa and Conecuh Counties, to compare those counties with and without OB services, respectively. The χ2 test was used to determine statistical significance across time and across county (P < .05).
Results
Comparison of Periods 1 and 2
Pickens County experienced a significant (P = .001) decrease (60%) in IMR between periods 1 and 2 (Table 3). During period 1, no OB services were available in the county, and the IMR was 17.9. During period 2, however, because full prenatal care and delivery services were provided locally, the IMR dropped to 7.2. Because both the percentage of LBW births (Table 4) and births to females aged 10 to 19 years (Table 5) increased nonsignificantly from period 1 to period 2 (P = .07 and P = .12, respectively), neither of these factors are likely to have contributed to the observed drop in infant mortality. Furthermore, although both state and national IMRs declined from period 1 to period 2 (17.5% and 23.9%, respectively), the rate of decline for both is less than the rate of decline observed in Pickens County over the same periods (Table 3). Because Alabama currently and historically has exhibited a higher IMR than the United States overall, the relatively slower rate of decline observed for the state was not unexpected.
Cumulative Infant Mortality Rate of Selected Counties During Periods 1, 2, and 3
Cumulative Rate of Low Birth Weight in Selected Counties During Periods 1, 2, and 3
Cumulative Births to Females Aged 10 to 19 Years in Selected Counties for Periods 1, 2, and 3
Clarke and Monroe Counties experienced a steady decline (43%) in IMR over periods 1 and 2 (P = .001) (Table 3). These counties maintained OB services throughout the study periods, and therefore the decline that occurred in these counties could reflect the natural decline in IMR, especially because it more closely resembles the rate of decline experienced by the state overall. During period 1, the combined IMR was 14.5, dropping to 8.3 during period 2. The combined percentage of births to females aged 10 to 19 decreased slightly (P = .08) (Table 5), and the percentage of LBW births increased slightly (P = .13) from period 1 to period 2 (Table 4).
As for Coosa and Conecuh Counties, the combined IMR increased slightly (15%) from period 1 (IMR, 12.5%) to period 2 (IMR, 14.4%; P = .55) (Table 3). The counties' combined percentage of births to women aged 10 to 19 declined during that time: from 24.2% during period 1 to 19.2% during period 2 (P < .001) (Table 5). The percentage of infants with LBW increased: from 9.5% during period 1 to 12.4% during period 2 (P < .001)—a rate of increase that exceeds the observed rate of increase for the state of Alabama (Table 4).
Comparison of Periods 2 and 3
Coinciding with the discontinuation of delivery services between periods 2 and 3, the IMR in Pickens County more than doubled, from 7.2% to 16.0% (P = .02) (Table 3). This is in stark contrast to the declining IMR observed both at the state and national levels between the same periods of time (declines of 10% and 13.6%, respectively). Although the percentage of LBW increased slightly (from 11.5% to 11.8%; P = .75) (Table 4), the percentage of births to females aged 10 to 19 decreased by 44% from period 2 to period 3 (P < .001) (Table 5). Because these trends are consistent with births to women aged 10 to 19 and the percentage of LBW in Alabama overall, it is likely that other factors contributed to the increase in IMR in Pickens County between these 2 periods.
Clarke and Monroe Counties also experienced a 19.3% increase in their combined IMR from period 2 to period 3 (P = .36) and notably exhibited a 41% increase in percentage LBW (P < .001)—the largest increase in LBW of all the counties included in this study from period 2 to period 3 (Table 3 and 4). The percentage of births to females aged 10 to 19 decreased at a rate comparable to that statewide during this period (Table 5).
Coosa and Conecuh Counties experienced a nonsignificant decline (24.3%) in their IMR from period 2 to period 3 (P = .26) (Table 3). It is worth noting that while the percentage of births to females aged 10 to 19 declined in these counties, the percentage of infants with LBW remained stable (Tables 4 and 5).
Comparison of Periods 1 and 3
To investigate further the role that full-time availability of local prenatal care can have on perinatal outcomes—despite the loss of local delivery services—we compared data from periods 1 and 3. It is notable that although the IMR increased following the loss of the maternity unit at the local hospital, the IMR in Pickens County was still lower during period 3 than during period 1, during which no local prenatal or delivery services were available; this difference, however, was not statistically significant (P = .64) (Table 3). In fact, during period 3, the provision of prenatal services by 1 provider alone resulted in a 10.6% decline in IMR when compared with period 1. As expected, both the state and national IMRs during period 3 were significantly improved when compared with period 1 (declines of 25.8% and 34.2%, respectively). Clarke and Monroe Counties also exhibited a net improvement in IMR between periods 1 and 3 (P = .03), reflecting both the state and national trends. It is interesting, however, that the combined IMR observed in Coosa and Conecuh Counties declined nonsignificantly (by 12.8%) when period 1 is compared with period 3 (P = .62)—similar to the decline in Pickens County.
For all study counties and the state of Alabama, the percentage of births to females aged 10 to 19 was lower during period 3 than period 1. The percentage of infants with LBW was higher (Tables 4 and 5).
Discussion
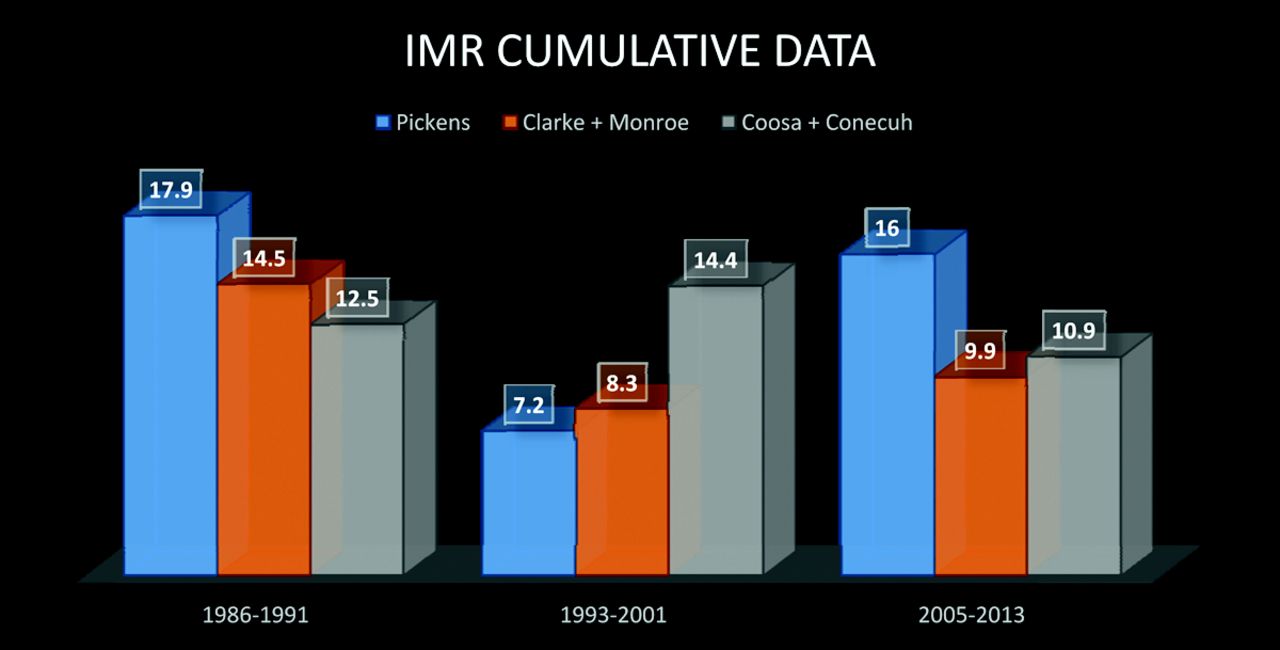
This study takes advantage of a “natural” experiment that occurred in a poor, rural Alabama county in order to study the association of IMR with the availability of prenatal and OB care, especially that provided by FPs. When both prenatal care and delivery services were available locally, Pickens County exhibited a 60% decrease in IMR. Pickens County achieved an IMR that was not only lower than that of any of the control counties but also lower than both the state and the national mean IMRs during the same period. Although the state and national mean IMRs declined from period 1 to period 2, as did that in Clarke and Monroe Counties, their respective rates of decline did not reach that in Pickens County (Figure 2).

Cumulative infant mortality rate (IMR) data (infant death per 1000 live births).
Furthermore, loss of the local maternity unit coincided with a more than doubling of the county's IMR during a period in which the state and national IMRs continued to decline steadily. The reasons for closing the unit cited by the hospital included loss of the providers, which is 1 of the most commonly cited reasons for closing OB units among US rural hospitals.3 This study serves to illustrate further the reliance of rural hospitals on FPs to provide OB care, as past studies have done.4,5,10 In light of this, the declining number of FPs who are trained in and choose to provide OB services becomes even more concerning.9,10,23
However, just as FPs benefit the health of the local population when they choose to provide maternity services, a benefit to the physicians themselves has also been documented. Avery and associates25 documented that FPs practicing OB earn more than those who do not, despite the modest increase in the cost of malpractice insurance. In addition, the annual economic impact to rural communities may total >$1.4 million per practicing FP providing OB services—a >40% increase in the economic benefit to the community—compared with those practicing family medicine without OB.26 Likewise, loss of rural OB units can result in economic losses to a community.15 Perhaps future efforts by rural hospitals to attract OB providers may involve targeting those physicians who are most likely to provide OB care in rural areas, especially properly trained FPs.
An additional challenge to operating a rural maternity unit involves maintaining a birth volume large enough to allow providers to maintain competencies.26,27 This can be difficult given that rural maternity units are often equipped to handle only low-risk deliveries, and patients may choose to bypass the local hospital in favor of larger regional hospitals offering more comprehensive services.26 It has also been suggested that providers who routinely practice low-risk OB may be at some disadvantage, as they are faced with emergencies much less frequently than high-risk practitioners.27 However, the Advanced Life Support in Obstetrics program was developed specifically for that scenario, enabling practitioners working in mainly low-risk situations to maintain competencies for OB emergencies. The course is designed to give providers the competence to practice in a setting in which they have limited backup.27
Perhaps another means to maintain such competencies would involve periodically sharing call duties within the nearest regional medical center, allowing the rural practitioner continued experience in managing high-risk deliveries. It should be noted that FPs providing OB services experience lower rates of cesarean deliveries, forceps deliveries, and labor inductions in low-risk pregnancies when compared with OB/GYNs.28 FPs providing OB services handle higher rates of spontaneous vaginal deliveries and vaginal deliveries after cesarean when compared with OB/GYNs, even when high-risk pregnancies are not referred.28 Furthermore, when cesarean deliveries are performed by FP providing OB services, patients experience no difference in the rate of intraoperative or infectious complications, and they develop fewer postoperative complications.29
Despite the loss of local delivery services, full-time prenatal care continued to be provided in Pickens County by an FP trained through an OB fellowship. Although the IMR did increase following the discontinuation of delivery services, access to prenatal care alone resulted in a 10.6% decline in IMR when compared with period 1, during which no OB services were available in the county. Concerns regarding continuity of care were raised previously when rural women received prenatal care locally and delivered at a regional center.4 It should be noted that the prenatal care provider in Pickens County shared call duties with the nearest university-associated OB practice but worked to perform deliveries for as many of her own patients as possible at the nearest regional medical center, reducing handoffs to other providers at the time of delivery.
Limitations
This study is limited in that it is an observational, correlational study and cannot be used to draw formal conclusions about causal relationships. Again, many socioeconomic and yet unknown variables, which are outside the scope of this study, are known to contribute to IMR. Many factors obviously influence changes in IMR, and any number of socioeconomic issues not addressed within the scope of this study may contribute.
Conclusions
This study took advantage of a natural experiment that occurred in several rural Alabama counties in order to isolate the effect of the provision of OB care in such areas, especially as provided by FPs. As was expected, Pickens County exhibited its lowest IMR when both prenatal care and delivery services were provided locally by 2 FPs, and during that period the county achieved an IMR that was lower than both the state and national IMRs during the same period. Closure of the local maternity unit coincided with a >50% increase in IMR. However, the provision of full-time prenatal care by an FP trained through an OB fellowship, even in the absence of local delivery services, was shown to provide benefit and contributed to the 11% decline in IMR when compared with a period of time in which no OB care was available locally.
This study provides evidence that properly trained FPs can have a profound impact on infant mortality in rural areas. As such, future efforts by rural hospitals to maintain operating maternity units should perhaps focus on recruiting providers who are most likely to provide OB services to rural and underserved populations, namely, properly trained FPs.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/31/4/542.full.
- Received for publication September 18, 2017.
- Revision received March 26, 2018.
- Accepted for publication March 27, 2018.




{kind=link}
{kind=link}