
Abstract
Background: Obesity is a serious and highly prevalent health problem. Behavioral modification for weight loss is effective, and physician nutrition counseling is encouraged. Nevertheless, several studies have reported that physicians provide nutrition counseling infrequently. Time constraints and lack of patient compliance are among frequently reported barriers.
Aim: In this pilot study, we aimed to examine physician weight loss nutrition counseling among family physicians in Huntington, West Virginia, an area with the highest obesity prevalence in the United States.
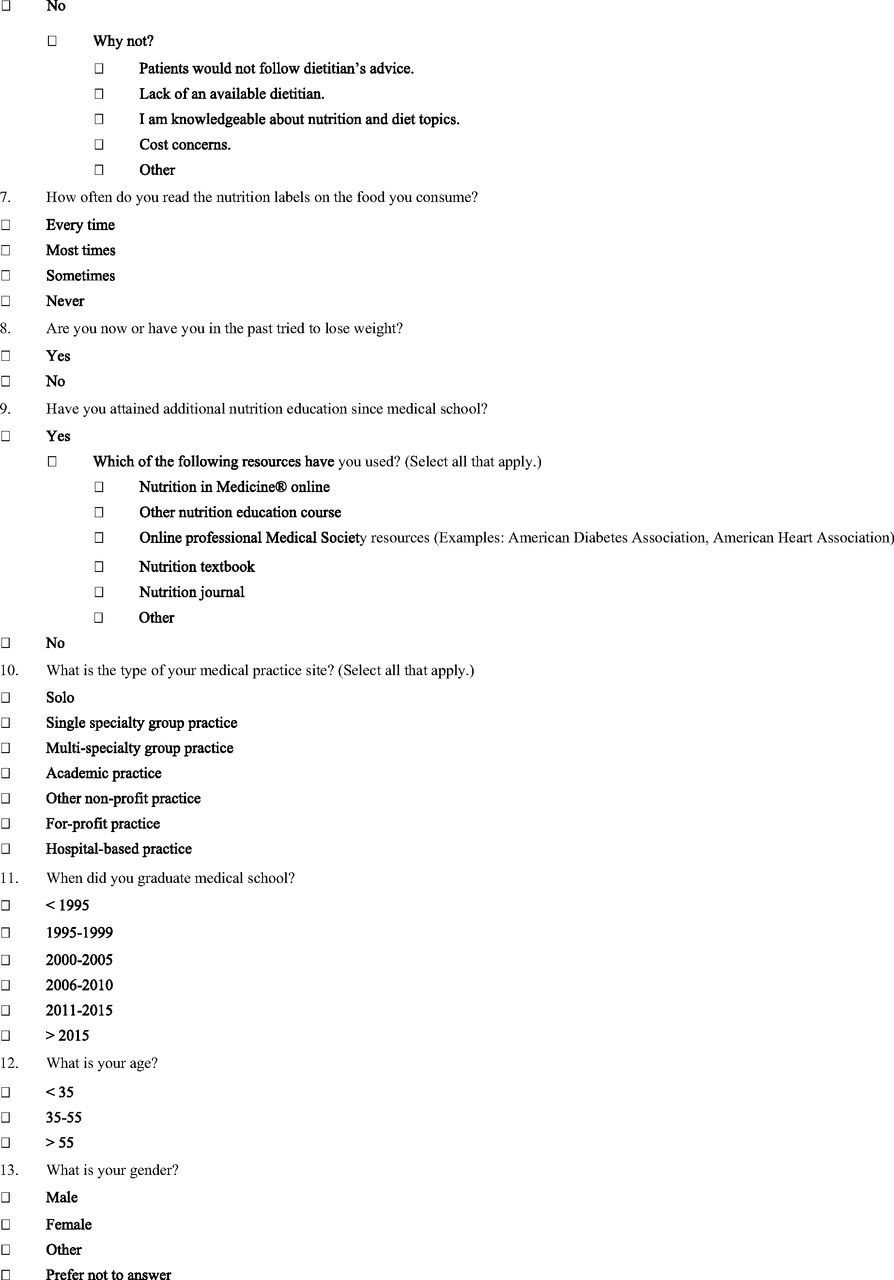
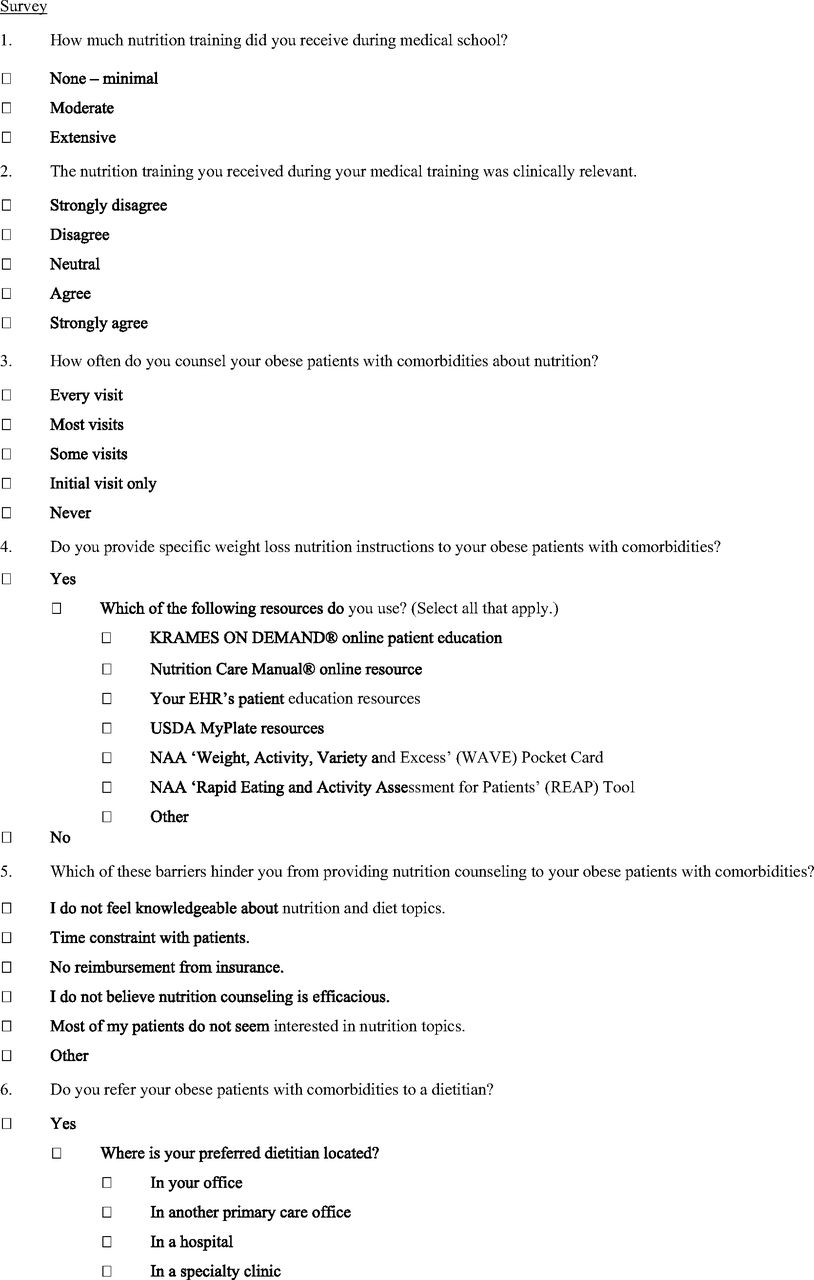
Methods: We administered an anonymous 13-question online survey designed for this study to all area family physicians in continuity ambulatory practice, asking about how often they provided nutrition counseling to their comorbidly obese patients, their nutrition education background, the counseling resources used, and the barriers they faced.
Results: Thirty-eight of the 47 invited physicians completed surveys. The 35 to 55 age group comprised 55% of the respondents. Men comprised 53% of our sample. Two-thirds of the physicians reported that they counseled at a high frequency. Twenty-six of the 38 physicians reported that their nutrition education in medical school was none to minimal. Of the rest, 47.2% viewed their education as clinically relevant. The most frequently-used specific patient education sources were those embedded in electronic health records, the US Department of Agriculture's MyPlate tool, and a variety of smartphone-based apps. Time constraints and lack of patient interest in nutrition topics were the leading barriers cited.
Conclusion: Family physicians practicing in the most obese population in the United States tend to be high-frequency obesity nutrition counselors who frequently use specific tools, consider their education lacking and face oft-cited barriers. Studies in other highly endemic areas are needed to confirm these findings.
Obesity is a serious and highly prevalent health problem, especially in West Virginia. Centers for Disease Control and Prevention data from 2016 show that although adult obesity rates exceed 20% in all 50 states, in 5 states, 1 of them being West Virginia, 35% or more of adults are obese.1 As of August 2017, West Virginia had the highest adult obesity rate in the nation (37.7%).2 Our region, the Huntington-Ashland, West Virginia-Kentucky-Ohio area, had the highest prevalence of obesity (37.1%) among the 145 metropolitan and micropolitan statistical areas across the United States surveyed in the 2013 Behavioral Risk Factor Surveillance System Survey.3 It has also been well established that obese persons have a higher prevalence of hypertension, hyperlipidemia, diabetes, and metabolic syndrome when compared with normal-weight individuals.4 Obesity reduction is therefore a pressing health care need, especially in high prevalence areas such as ours.
A 2014 systematic literature review cites 3 studies demonstrating the efficacy of face-to-face intensive behavioral counseling by primary care practitioners assisted by trained assistants.5 Monthly, brief, structured counseling sessions yielded significantly greater mean weight losses at 12 months to 24 months than usual care groups (1.6–2.9 kg compared with 0.6–1.7 kg).
Another 2014 systematic literature review and meta-analysis confirmed the utility of behavioral modification for maintaining weight loss for up to 24 months.6 The United States Preventative Services Task Force recommends multicomponent, recurrent behavioral interventions for patients with a body-mass index of 30 kg/m2 or higher.7 The American Academy of Family Physicians also recommends repeated behavioral interventions and counseling for obese patients.8 Joint guidelines from the American Heart Association, American College of Cardiology, and The Obesity Society recommend prescribing obese individuals a diet to reduce calorie intake as part of a comprehensive lifestyle intervention.9 Primary care practitioners are recommended to meet with patients for at least 14 sessions over 6 months (once a week for the first month and every other week for the remainder). Patients are to be encouraged to achieve a negative calorie balance of 500 kcal/d or more and to exercise 150 minutes or more a week. The role of physicians as providers of nutrition counseling is highlighted by the Healthy People 2020 objective: “to increase the proportion of physician office visits made by adult patients at which obese patients are counseled about weight reduction, nutrition, or physical activity.”10 Furthermore, since 2011, primary care providers can receive reimbursement by the Centers of Medicaid and Medicare Services (CMS) for providing multiple sessions of intensive behavioral therapy to Medicare beneficiaries with obesity.11
However, nutrition training in medical school curricula has long been considered inadequate. Recognizing this, in 1995, the Department of Nutrition of the University of North Carolina at Chapel Hill developed a nutrition curriculum designed for undergraduate medical education called Nutrition in Medicine (NIM).12 Unfortunately, Adams and colleagues13, in their annual survey of medical school nutrition education curricula, found that in the 2012 to 2013 academic year only 36% of the respondent medical schools were using NIM curriculum and that 71% of the 121 US medical schools surveyed failed to provide the 25 hours of nutrition education they considered a bare minimum.
Perhaps unsurprisingly, several studies have found low rates of physician nutrition counseling. In a 2009 to 2010 study of low-income obese adults in the United States, only 48% of 548 respondents reported receiving advice to lose weight from their health care provider in the previous 12 months.14 Another study using 2011 data from the National Health Interview Survey of US households found only 32.6% of the sample reported being counseled on diet from a physician in the previous 12 months.15 Wadden and colleagues,5 in their systematic review of the literature from 1980 to 2014, could not find any studies of acceptable quality documenting physicians providing obesity counseling according to CMS guidelines. We found no published studies of weight loss nutrition counseling by physicians in West Virginia.
In this study, we (a family physician and a medical student) aimed to document the perceptions of family physicians in Huntington, West Virginia and 2 smaller neighboring towns regarding the frequency and nature of their counseling patients on weight loss nutrition. We also sought to document selected characteristics of these physicians and their relationship to frequency of counseling. We intended for this project to ultimately guide further research aimed at increasing the frequency and efficacy with which primary care physicians provide obese patients with nutrition counseling.
Methods
We were granted expedited approval from our institution's Institutional Review Board. With our research goals in mind and using prior research findings, we designed a 13-question online survey that participants could take without needing to answer all the questions (Appendix). We estimated that it would take 5 minutes to 10 minutes to complete based on pilot testing on 3 physicians. The physicians were queried on the proportion of visits with comorbidly obese patients at which they provided nutrition counseling, the outcome variable in our study. The survey also collected the physicians' demographic information, their medical education in nutrition, and their perceptions and practices regarding patient nutrition counseling, including the resources they use in counseling.
The inclusion criterion for our study was physicians listed in the Family Medicine section of the Herald-Dispatch 2017 Health Source, which is a comprehensive Huntington, West Virginia, area physician directory that is updated annually.16 We excluded those physicians that were not listed as having at least one practice site in either Huntington, Barboursville, or Ceredo-Kenova, West Virginia. In a few cases, it became apparent during recruitment that the physicians were not actually practicing at the listed site. In addition, excluded physicians were those who were listed as not being in ambulatory family medicine practice.
Our recruitment methods depended on whether the physician was affiliated with our medical school family medicine department. For physicians so affiliated, we sent out an intramural e-mail invitation containing an online survey consent and a uniquely personalized embedded link to the survey. In addition, our physician investigator made a verbal announcement regarding this e-mail at a department faculty meeting. For physicians not affiliated with our department, our physician investigator called the physicians to personally give a verbal invitation and to obtain a preferred e-mail address. If preferred, he arranged a follow-up phone appointment during which the student investigator administered the survey verbally and entered participants' responses directly and confidentially into the online survey instrument on their behalf. One week after all the invitees received the initial survey by e-mail, a duplicate e-mail was sent out to those who had not completed the survey. Finally, 3 days to 5 days after the second e-mail, the physician investigator personally contacted any remaining nonrespondents.
The survey and the responses were managed confidentially solely by a research coordinator using REDCap, a secure web-based survey and data storage resource.17 The research coordinator only provided the investigators deidentified data. He also periodically provided the investigators with a list of the names of those who had accessed the online survey for purposes of follow up.
We used the Herald-Dispatch Health Source 2017 directory to identify the medical school at which each participant obtained their medical degree. We determined the group of participants exposed to NIM as follows. First, we excluded those who graduated from medical school before 1995 when NIM was first implemented. We then contacted the relevant administrator at the medical schools of the remaining physicians to inquire if the school had used NIM and, if so, when. In the cases of those medical schools which had used NIM, we excluded physicians based on their graduation year by using 2 assumptions: that NIM curriculum was used in the first 2 years of medical school and that the physician had matriculated to the same school from which they graduated.
For statistical analysis, we grouped the respondents into 2 categories based on how frequently they reported counseling, designating “higher frequency counselors” as those physicians who reported providing nutrition counseling at every visit or most visits. “Lower frequency counselors” were those who reported they counseled at some visits, at the initial visit only, or never. We examined the data for correlations between this outcome variable and other physician characteristics by using Fisher's exact test. We used Stata 14.0 (College Station, TX) for all statistical analyses.
Results
Out of an initial list of 89 family physicians in the physician directory, we sent e-mails to the 47 physicians who met our study participation criteria. Thirty-eight surveys were completed, for a response rate of 80.9%. One survey was completed via phone interview, whereas the other 37 were completed online directly by the participants.
Twenty-four physicians (63%) were high frequency counselors by report. The physicians' characteristics are displayed in Table 1. Over half of the physicians who completed the survey were aged 35 to 55 (55%). Our sample was evenly divided between men and women, with males making up 53% of the physicians. Thirty-two physicians (84%) acknowledged having tried to lose weight and 60% reported reading nutrition labels most or every time. Three-quarters (74%) of the surveyed physicians graduated from Marshall University's Joan C. Edwards School of Medicine, the only medical school in the Huntington area. The highest proportion of respondents (34%) graduated before 1995. Less than a third (32%) of the sample reported having at least a moderate amount of nutrition education in their medical school curricula. Less than half (47%) of the 36 who commented felt that their medical school nutrition curricula was clinically relevant. Over half (55%) of our sample reported having obtained additional nutrition education since medical school, most often in the form of nutrition education courses and online professional Medical Society resources (such as American Diabetes Association and American Heart Association).
Prevalence of Physician Characteristics by Frequency of Counseling
The nature of the physicians' counseling can be characterized in several ways. Three-quarters (74%) reported that they referred to a dietitian. Those who reported that they did not refer patients to a dietitian cited either the lack of availability of a dietitian (13%) or cost concerns (11%). Most (89%) of the physicians in our sample reported providing specific nutritional information. Resources most often used were those embedded in electronic health record systems, the US Department of Agriculture's MyPlate tool, and smartphone apps (Table 2). Barriers to counseling were cited by almost all (97.4%) participants (Table 3).
Frequency of Selection of Specific Nutrition Patient Education Resources
Frequency of Selection of Specific Barriers to the Provision of Nutrition Counseling
Discussion
Our sample of family physicians reported a considerably higher frequency of nutrition counseling than might be expected considering previously published estimates of the frequency of physician nutrition counseling.5,14,15,18 This discrepancy might be a result of these studies being based on patients' reports, whereas we queried physicians. In addition, it is probable that physicians would counsel their patients more frequently in a region in which obesity and its comorbidities are highly “endemic” than in regions of lower prevalence.
We explored a variety of factors that might affect the frequency of weight loss counseling by physicians, which can be grouped into 3 categories: physicians' professional education, their clinical practice, and their personal characteristics. Given the results of national surveys of nutrition education in US medical school curricula, it is not surprising that two-thirds of the sample reported minimal to no nutrition training. Although the majority of our respondents used specific patient education tools, none mentioned Rapid Eating and Activity Assessment for Patients or Weight, Activity, Variety, and Excess. This is notable because these resources were specifically developed for use by physicians as part of the National Institutes of Health's Nutrition Academic Award program; one goal of this program being to develop medical school curricula to equip physicians to deliver effective nutrition counseling.19,20 Previous studies surveying physicians about their perceived barriers to nutrition counseling have cited lack of time during appointments, inadequate reimbursement, lack of patient compliance, and physicians' low self-efficacy or lack of knowledge.21,22 Our findings were consistent with these studies. Finally, obesity among physicians themselves has been recognized as a significant problem.23,24 In fact, there is some recent evidence to suggest that physicians' own poor health behaviors and obesity status have a negative impact on their propensity to counsel their obese patients regarding weight loss and on their self-efficacy in doing so.25 There was a greater proportion of higher frequency counselors (71.4%) among those reported reading nutrition labels frequently than among those who reported rarely reading nutrition labels (64.3%). In addition, over half of physicians who had attempted weight loss were also high-frequency counselors. However, neither these physician characteristics nor any of the others were statistically significantly associated with being a higher frequency counselor. Moreover, we did not ask our respondents whether or not they were obese.
The major limitation of our investigation was the size of our sample. We achieved a substantial response rate, but the total number of family physicians practicing primary care in our study region was small. We elected to confine our survey to family physicians because they are well positioned to provide their patients with nutrition counseling because of their biopsychosocial or holistic model of care. That this model of care is greatly important is evidenced by CMS's reimbursement requirement that physicians use behavioral techniques to “aid the patient in achieving agreed-on goals by acquiring the skills, confidence, and social/environmental supports for behavior change.”11 In addition, family physicians are particularly able to engage the family in which context nutrition decisions are often made.
Another limitation to the validity of our findings is the homogeneity of our sample's medical education background. The majority of our respondents (74%) were graduates of one medical school. Furthermore, all but 4 participating physicians (89.5%) were graduates of the same institution's family medicine residency program. However, although a more educationally diverse group would have allowed us more robust statistical data analysis, the fact is that family medicine residency graduates tend to practice within 100 miles of their residency program.26 Therefore, it would have been difficult to achieve a more heterogeneous sample without widening our study region outside of our area of interest.
Thirdly, despite the high response rate, our sample might suffer from some degree of sampling bias. Of the 9 invitees who did not complete the survey, 8 were physicians in a single, large, private medical group. In fact, we only received 1 survey from all the family physicians in the group. Because 7 of the 8 nonrespondents were neither graduates of our local medical school nor of its family residency program, their participation would have substantially diversified the sample.
Fourthly, verbally completing the questionnaire introduces a potential bias by removing anonymity in the data collection process. However, since only one participant took this option, this bias is unlikely to be significant.
Finally, for at least two reasons, the results of our survey are limited by our reliance on physician self-reporting. Although this is an appropriate strategy in studying physicians' perceptions, it is only an approximation of the actual physician counseling frequency. At the very least, there is a well-recognized discrepancy between patients' and physicians' perceptions of what transpires during an office visit.27 However, other methods such as patient chart review for documentation of such counseling or patient surveys are also fraught with potential inaccuracy. Even direct observation of the office visit would have to account for the potential that the observation or knowledge of its possibility might alter the physician's behavior, the Hawthorne effect. In addition, a survey calling for graded responses based on subjective perception is vulnerable to inter-rater discrepancy. Therefore, it is important to recognize that although the responses we elicited are indicative of physicians' perceptions, they are not reliable objective measures.
What this study has achieved is to document that the majority of family physicians in a portion of one high-obesity prevalence area report that they counsel their comorbidly obese patients at least during most visits by using specific patient education tools. We have also shown that the majority of these physicians consider their medical school nutrition education to be inadequate and that they are particularly aware of the barriers of time constraints and patients' lack of interest.
Further research should seek to further investigate these findings, paying particular attention to the physicians' perceptions of their educational preparedness as well as to their specific counseling methods by using the CMS model as a benchmark.11 For instance, it would be helpful to know to what extent and how often physicians use the recommended “5 A's” strategy (Ask, Advise, Assess, Assist, Arrange).28 In addition, with the proliferation of the patient-centered medical home model, the role of dietitians in the medical team has been highlighted.29 To what extent dietitians play a collaborative, in-practice role with physicians and what influence their interaction has on physicians' counseling practices are other areas of study to emphasize. The prerequisite next step, however, is to study larger samples of primary care physicians both in our area and in other “highly endemic” areas.
Acknowledgments
Todd Gress, MD, Appalachian Clinical and Translational Science Institute, Marshall University for statistical analysis Richard Sutphin, BS, MPH., Research Coordinator, Department of Family and Community Health, Joan C. Edwards School of Medicine at Marshall University.

Notes
This article was externally peer reviewed.
Funding: This project was partially funded by a Student Externship Matching Grant from the American Academy of Family Physicians Foundation.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/31/4/522.full.
- Received for publication December 19, 2017.
- Revision received March 10, 2018.
- Accepted for publication March 24, 2018.




{kind=link}
{kind=link}