
Article Figures & Data
Figures
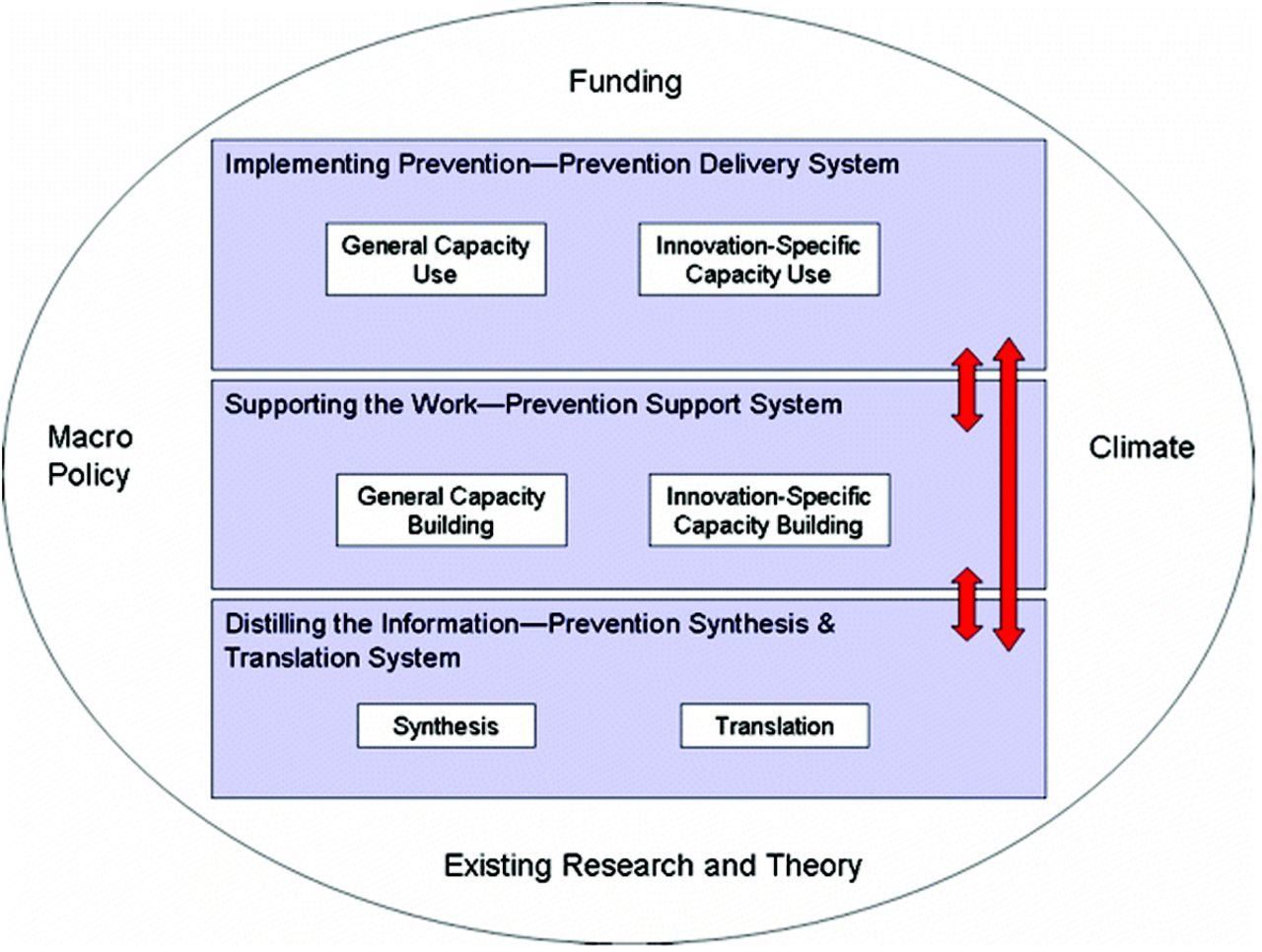
- Figure 1.
The Interactive systems framework for dissemination and implementation.8 Used with permission from Springer.
- Figure 2.
Interactive “process” framework for the implementation of complex interventions.

Tables
- Table 1.
The 5As Team (5AsT) Implementation Strategies, Methods, and Actors Structured According to the Interactive Process Framework (Figure 2)
5AsT Strategy Methods Team Members and Actors Flexible Intervention with Fixed Core Elements and Adaptable Periphery Needs assessment Participants self-identified learning needs Research team and clinical champion Expert speaker Interdisciplinary experts addressed learning gaps Research team arranged expert speakers Up to date research and practice implications Learning collaboratives Sharing of experiences, ideas, discussing needs, group activities, interactive activities Coordinated by clinical champion, facilitated by clinical champion, and PCN clinician trained in practice facilitation Co-creation of tools In response to identified needs search for existing tools, creation of tools, iterative with providers and graphic designers Facilitated research team and graphic designer, and cocreated by participants Supporting learning resources Podcasts, tools online, and emailed one week after session Compiled by research team, topic experts, with input from clinicians and participants Summaries of session materials emailed after session Flexible Intervention Adaptation Change of session topics Clinical champion and research team Change of learning collaborative groups Addition of team relationship–enhancing activities Iterative Qualitative Evaluation Clinical champion and researchers Ongoing feedback between participants, PCN management, and research team. Clinical champion kept logbook of encounters with researchers and detailed record of all project materials and communications Clinical champion and research team Qualitative evaluation Guided field notes on intervention sessions, interviews parallel to ongoing intervention, evaluation workshops [at 6 and 12 months] Researchers and clinical champion Collective Sense-Making Learning collaboratives Sharing of experiences, ideas, discussing needs Coordinated by clinical champion, facilitated by clinical champion, and PCN clinician trained in practice facilitation Group activities, interactive activities Team meetings Troubleshooting emerging barriers Research team, feedback from clinical champion Goal setting in learning collaboratives Making explicit the implications of knowledge for practice and practicable strategies for putting them into action Learning collaborative facilitators and clinician participants Engagement Research partnership PCN management as co-investigator, collaborative grant writing and intervention design, PCN in-kind contributions [dedicated time of clinical champion] PCN administrative and senior clinical leadership Practice facilitators Clinical champion and anthropologist from the research team keep logs of their encounters and detailed record of all project materials and communications 5AsT practice facilitators were the clinical champion and research team anthropologist Clinical champion Research team meetings, logistics, communication. Consulted on interviews, tools, problem solving, and review of codes and themes Clinical champion (a frontline PCN dietician) Team meetings Implementation evaluation update, interview and analysis update, peer coding, troubleshooting emerging barriers, reviewing results papers [dissemination] Research team, clinical champion, and PCN administrative and senior clinical leadership Transparency Open communication about intervention intent, encouragement of participant input Research team, clinical champion, and PCN administrative and senior clinical leadership Organizational Context Partnership 5AsT as part of PCN business plan, PCN in-kind contributions [dedicated time of clinical champion] Research team and PCN administrative and senior clinical management Clinical champion Navigated logistics, recruitment, arranged for spaces, time, food; introduced team to organizational culture Clinical champion (a frontline PCN dietician) Research and Theory Knowledge synthesis and transformation Expertise on 5As of obesity management and on obesity topics, snowball sampling of existing tools, and cocreation and publishing of new and adapted tools Research team, topic experts, participants, graphic designer Implementation framework/theory Selection of framework for project design based on focus on context, after project revision of lessons learned, and refinement of theoretical approach Research team Policy and Funding PCN partnership Using the PCN structure and autonomy to partner in research PCN leadership Grant application Leveraging grant funding with PCN in-kind contributions Research team and PCN administrative and clinical management PCN, Primary Care Network.
- Table 2.
Supporting Data on 5As Team Implementation Process from Participant Interviews and Field Notes
Finding Representative Quotes, Field Notes, and Examples Knowledge (synthesis and transformation) A2: I really liked it. It was really just kind of asking us what we want to learn and what we find we can use to help patients so it's really, I like that it's focused on us and what we want to learn. A11: I like that you guys ask us what our needs are and, and, and that kind of helps bring in what, what's relevant to us Practice support (team and individual capacity building) C6: I was feeling positive about my knowledge and my beliefs in it but I wasn't very good at sharing them to other people so there's been a little bit more of that since I've done it, I can talk more comfortably and not be so afraid to kind of challenge some of the physician's statements and opinions so that's been helpful to feel a little bit more, more assertive I guess in that and have something to back it up with so. A3: I was really excited. I'm going, actually the first morning back I went around to all the doctors and gave them a copy of each of the, the tear offs saying you know this is, you know this is finally actually on one piece of paper, the approach we've been using with weight. A14: I will see someone and then or X will see somebody, our dietician and say you know what, you need to go see X, … , you know you're not ready to deal with any of these, we have to deal with this first and so I think we've really been more conscious and doing that more even since we were all involved with this research so and we work together, you know … will meet with some patients together and come from two perspectives and then say you know what, I think you need to see X. Field notes from learning collaboratives: ∙ Laughter and joking were not uncommon and they increased as the sessions went on. This is evidence of a friendly atmosphere. ∙ Likewise discussion around tools, particularly the physical activity guidelines tool, which was critiqued quite a bit, is evidence of an open and sharing atmosphere. Practice delivery B4: Just collaborating at the end, having an open discussion, getting perspectives from different health care professionals is always good too and like even for today, we identified gaps in terms of the classes that we were offering for nutrition so it brought to light something like change right that can happen so it's good. I've, I've really enjoyed it. A11: It's really good. One thing that I have addressed is that in the waiting room we don't have any bariatric chairs, which can be a little bit uncomfortable so I have ordered those through the PCN for the clinic and for my office as well. B2: Yeah, well the one clinic where the scale was in the front entrance, I moved it to the back room into the clinic or in the office where I was and it was fine so. Interactional findings: Collective sense-making B2: Yeah I really like that. I like doing that because then you can learn something, then you talk with everybody about certain things and then you could try it in their clinic if you can so. B6: I like the breakout sessions so we get a chance to talk about and how it applies to our settings and to patients, I like that part of it. A5: I thought it was very good. I especially enjoyed today. I think it gives us new ways to look at things and I think we need each other's ideas because lots of times there's just one little thing that somebody else does that you never thought of and if we, if we work in isolation, you know if we never have meetings then and we always do the same thing with patients, we don't get any new ideas and I think that's important in learning, you know trying different things. Maybe it won't work but at least you've tried or, or it gives you another idea. Field notes from learning collaboratives: ∙ There are many examples of provider troubleshooting what they are learning with the realities of its application in clinics. Example: how to ask with very sensitive patients, or how to deal with weight bias when the doctor is the problem? ∙ There are examples of providers sharing ideas, little tricks, and often, specific wording of issues or questions that work well for them with patients. There was often rich discussion around topics wherein providers clarified any misunderstandings and found a common understanding of topics/facts/ideas that were brought up during the talk. Dynamic intervention and evaluation design Example of feedback that led to project adjustment A10: I think the facilitator should rotate or I don't think you're going, I think the group altogether is too big so I think they should try to rematch the groups a bit because there's certain, like the group I'm in is a very quiet group Field notes Deliberate introductions between participants are necessary and should be planned. Deliberate planning and strong facilitation of learning collaboratives: using quiet time before goal setting, trying different approach to encourage responses. Print-outs of materials and providing binders work well. Group activities and interactive methods (writing on charts, using sticky dots) were well received and could be used more often. Engagement Examples Intervention focus and design was reached through collaboration with the organization. Open communication was maintained by all involved. Study length, focus, and intensity were agreed upon through detailed discussion with the organization management and staff. A = Nurse
B = Dietician
C = Mental Health Consultant.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- What is known about the role of external facilitators during the implementation of complex interventions in healthcare settings? A scoping review
- Identifying Practice Facilitation Delays and Barriers in Primary Care Quality Improvement
- Practice Transformation Under the University of Colorados Primary Care Redesign Model
- Advancing the Science of Implementation in Primary Health Care