
Article Figures & Data
Figures
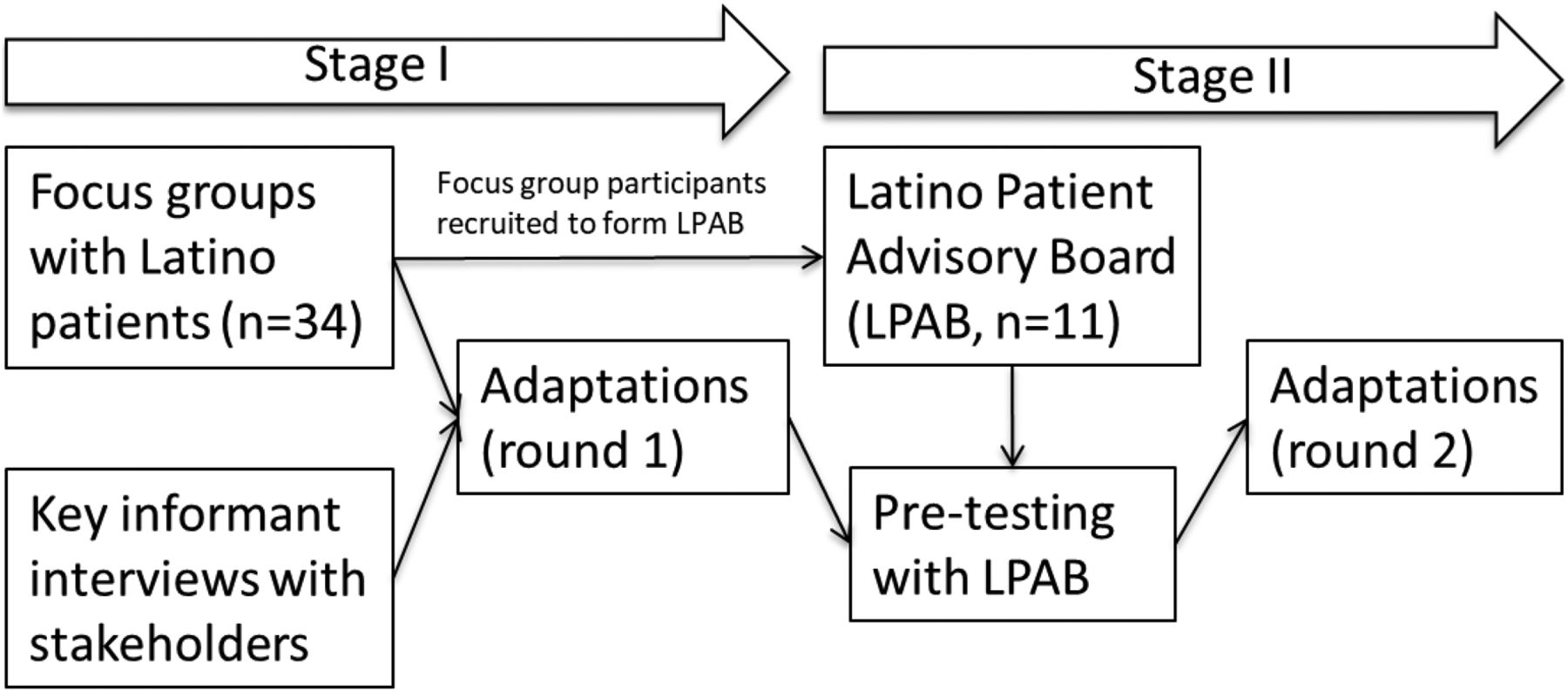
- Figure 1.
Cultural adaptation process for Vida Sana intervention.
Tables
- Table 1.
Description of Patient-Centered Outcomes Research Institute Patient Engagement Rubric with Examples from the Study
Engagement Principle Example from Study Reciprocal relationships: Roles of researchers, patients, and stakeholders are determined collaboratively and clearly stated. • Latino patient advisory board (LPAB) was formed with the goal of adapting the Group Lifestyle Balance intervention. • The first LPAB meeting included a discussion of roles, responsibilities, and ground rules. Colearning: Researchers, patients, and other stakeholders share their expertise with each other for mutual benefit. • Focus groups were used for researchers to learn from patients about their experience. • The LPAB provided their expertise in the cultural adaptation process. • Researchers shared their expertise in behavioral interventions with the LPAB during the adaptation process. Partnerships: Time and contributions of patients and stakeholders are valued and demonstrated in fair financial compensation. Also refers to a commitment to diversity and cultural competence. • Focus group participants were compensated for their time. • LPAB members were provided a meal and a stipend for each meeting they attended. Transparency, honesty, and trust: Information is readily shared among all partners. • LPAB members made recommendations and these were discussed with researchers until consensus was reached. Characteristic n or mean (% or SD) Female, n (%) 19 (56) Nativity, n (%) US born 5 (15) Foreign born, Mexico 22 (65) Foreign born, other 7 (20) Years in the US (foreign born), mean (SD) 24 (10.6) Age at migration, mean (SD) 23 (9.3) Education, n (%) Less than high school 3 (9) High school graduate 9 (27) Some college 8 (24) College or more 13 (39) Monthly household income, n (%) Less than $3,000 7 (21) $3,000–$6,999 5 (15) $7,000 or more 7 (21) Household members, mean (SD) 4 (1.4) Language preference for written materials, n (%) Spanish 21 (62) English 5 (15) No preference for Spanish or English 8 (24) Language preference for speaking, n (%) Spanish 21 (62) English 1 (3) No preference 12 (36) SD, standard deviation.
Focus Group Theme Category Focus Group Feedback 1st Round of Adaptations Family • Family was a key component of culture. • Included family members at 3 key timepoints in the intervention: the orientation session, a midintervention session, and the last session for graduation (Delivery). • Family support was most commonly reported as positive influence for changing lifestyle behaviors. • Negative influences from families included family members who were unsupportive of lifestyle changes or weight goals; time pressure/competing priorities from family members. • Developed tips for being a supportive family member (Content). Community • Community was a key component of Latino culture. • Provided support for participants to connect via the Smartphone applications (Delivery). • Included potluck meals (Delivery). Cultural foods • Food was an important element of Latino culture. • Incorporated a healthy meal at every group session (Delivery). • Cultural foods were the most commonly reported negative influences on healthy eating. • Ensured that meals provided healthy versions of cultural foods; examples included “sopes*,” ceviche, and black bean soup (Delivery). • Included more Latino food examples in intervention materials, including healthier, not-so-healthy, and traditional foods (Content). Healthy eating patterns • Traditional Latino eating patterns of a larger lunch and a smaller dinner were thought to promote weight maintenance. • The traditional Latino eating pattern was included as one option for a healthy eating pattern (Content). • Negative connotation of the term “diet” associated with restriction, deprivation, and limited food variety. • Avoided the term “diet” in favor of terms such as nutrition, eating, and eating plan (Content). • Challenges to healthy eating included eating breakfast consistently; finding time to cook appealing meals for the whole family. • Designed all session meals to account for budgets, time in preparation, and cultural norms (Delivery). Physical Activity • Physical activity in groups and children were sources of motivation to make healthy changes.
• Increased time in the US was associated with less occupational physical (more sedentary jobs) activity and exercise.
• Dancing and soccer were commonly mentioned as physical activity options that were culturally congruent. Three types of physical activity were discussed:○ Exercise: Zumba, walking, hiking, soccer, and gym workout.
○ Occupational: jobs in restaurants, hospitals, housekeeping and childcare.
○ Daily living: housekeeping, gardening, and commuting.
• Provided time for physical activity in groups during the sessions and encouraged physical activity among group participants outside of sessions (Content).
• Highlighted the distinction between leisure-time and occupational physical activity options and that each participants' activity mixture may be made up of different levels of each (Content).
• Emphasized the use of the pedometer to capture all types of physical activity (leisure-time, occupational, and daily living) (Delivery).
• Included more culturally congruent physical activity examples such as dancing and soccer (Content).Tech use • Heterogeneous familiarity with self-tracking via smartphone or web-based applications. • Allowed for time to introduce and troubleshoot the smartphone applications (Content). • Most participants were able to easily use the smartphone and web-based MyFitnessPal application to track diet. All but one participant downloaded the application on a smartphone without assistance. • Provided training on skills for self-tracking early in the intervention (Delivery). • Intervention coach provided online and in-person feedback on self-tracking information (Delivery). • All are interested in using the FitBit activity monitor as part of the intervention. • Provided all participants with a FitBit (Delivery). • The MyFitnessPal application was available in both Spanish and English, which was very helpful. • Encouraged participants to use MyFitnessPal application in their preferred language (Delivery). ↵* Sope is a traditional Mexican appetizer that includes vegetable and/or meat toppings on a thick corn meal base.
Original Group Lifestyle Balance Session Pretest Feedback 2nd Round of Adaptations Session 1: Welcome and getting started losing weight • Add an orientation session to the program and include family members so that they understand the intervention, its goals, and have simple tips for providing support to the participant. • Added an orientation session to accomplish the goals suggested by the patient advisors. The MyPlate graphic and concept is used to explain the intervention dietary goals to participants and their family members in the orientation session (Content). • Introduce skills sooner to capitalize on motivation. • Provided training on self-tracking diet and physical activity in session 1 (Content). Session 2: Be a fat and calorie detective • Very dense and long, consider reducing and moving some information to other session. • Moved a detailed section on weighing and measuring to session 1 to provide participants with tracking skills early on (Content). Session 3: Healthy eating • Introduce MyPlate earlier because it is important for calorie counting context and the visual is helpful for changing food choices. • Moved up the section on MyPlate to the orientation session (Content). • The session is too long. Session 4: Move those muscles • Positive feedback overall. • Moved discussion on pedometer from session 10 to this session (Content). • Further emphasized the distinction between leisure-time and occupational physical activity as they relate to planned versus unplanned activity (Content). Session 5: Tip the calorie balance • Positive feedback overall. • No changes. Session 6: Take charge of what's around you • Positive feedback overall. • Invited family members to this session (Delivery). • Included a potluck to create a sense of community with family members (Delivery). Session 7: Problem solving • The inclusion of family members was very positive but wanted them to be included in the prior session. • Family members were added to session 6 (Delivery). Session 8: Four keys to healthy eating out • Positive feedback overall. • Discussed strategies for social gatherings that are culturally congruent (Content). Session 9: Slippery slope of lifestyle change • Positive feedback overall. • No changes. Session 10: Jump start your activity plan • Introduce physical activity monitor earlier in session 1 because it allows participants to communicate via the smartphone application outside of the group sessions and it was helpful for tracking physical activity from the beginning. • Moved up the introduction of the pedometer to the first session (Content). • Added a group walk to promote a sense of community (Content). Session 11: Make social cues work for you • Positive feedback overall. • No changes. Session 12: Ways to stay motivated • Positive feedback overall. • Invited family members to session as a celebration for graduation; this included a second potluck where participants are encouraged to bring a healthy dish (Delivery).




{kind=link}