
Abstract
Purpose: Rates of risky substance use and substance use disorders are high in primary-care practices, yet the adoption of universal screening and brief intervention (SBI) has been slow and uneven. This study aimed to describe SBI-related attitudes, practices, and perspectives regarding practice change among medical providers in a minority-majority state.
Methods: We conducted a cross-sectional, on-line survey of a practice-based research network of medical providers serving predominantly Hispanic/Latinx and Native American patients in rural and urban settings. The main variables were clinician 1) perspectives on the need to address substance use problems in primary care, 2) current screening and intervention practices, and 3) satisfaction with and willingness to make changes to their practices.
Results: Although providers endorsed alcohol and opiate misuse to be significant problems in their practices, only 25% conducted universal screening. Providers reported focusing most of their screening efforts on those with substance use dependence. In general, providers rated importance of and ability to make practice changes moderately high. There was high interest in practice coordination with the community followed by interest in a collaborative care approach.
Conclusions: Providers mainly focus efforts on the relatively few patients at the tip of the pyramid (substance use dependence) rather than on the majority of patients who comprise the middle of the pyramid (risky substance use). Practice change strategies are needed to increase universal screening with a focus on risky substance use, particularly in practices serving racial/ethnic communities.
The integration of screening and brief interventions (SBIs) for patients with unhealthy alcohol and drug use in primary care continues to represent a significant challenge for clinicians in their efforts to address an expanding list of preventable health problems.1 Strong evidence supports universal screening for alcohol use while federal agencies encourage screening for drug use, especially in the context of illicit drug and prescription drug misuse.2⇓⇓–5 Despite these recommendations and awareness regarding the scope of the problem, research has consistently documented missed opportunities for detecting these problems.6
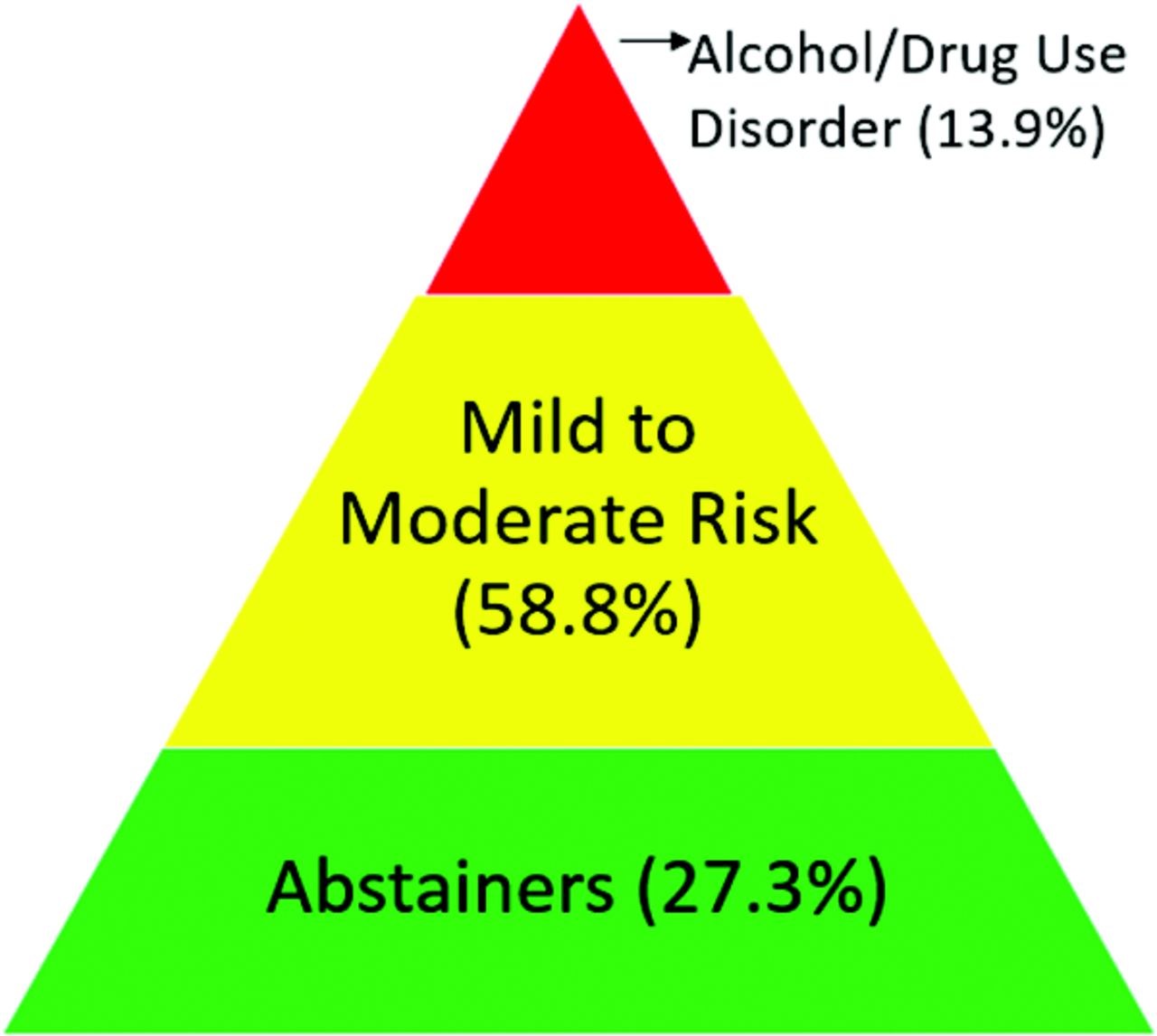
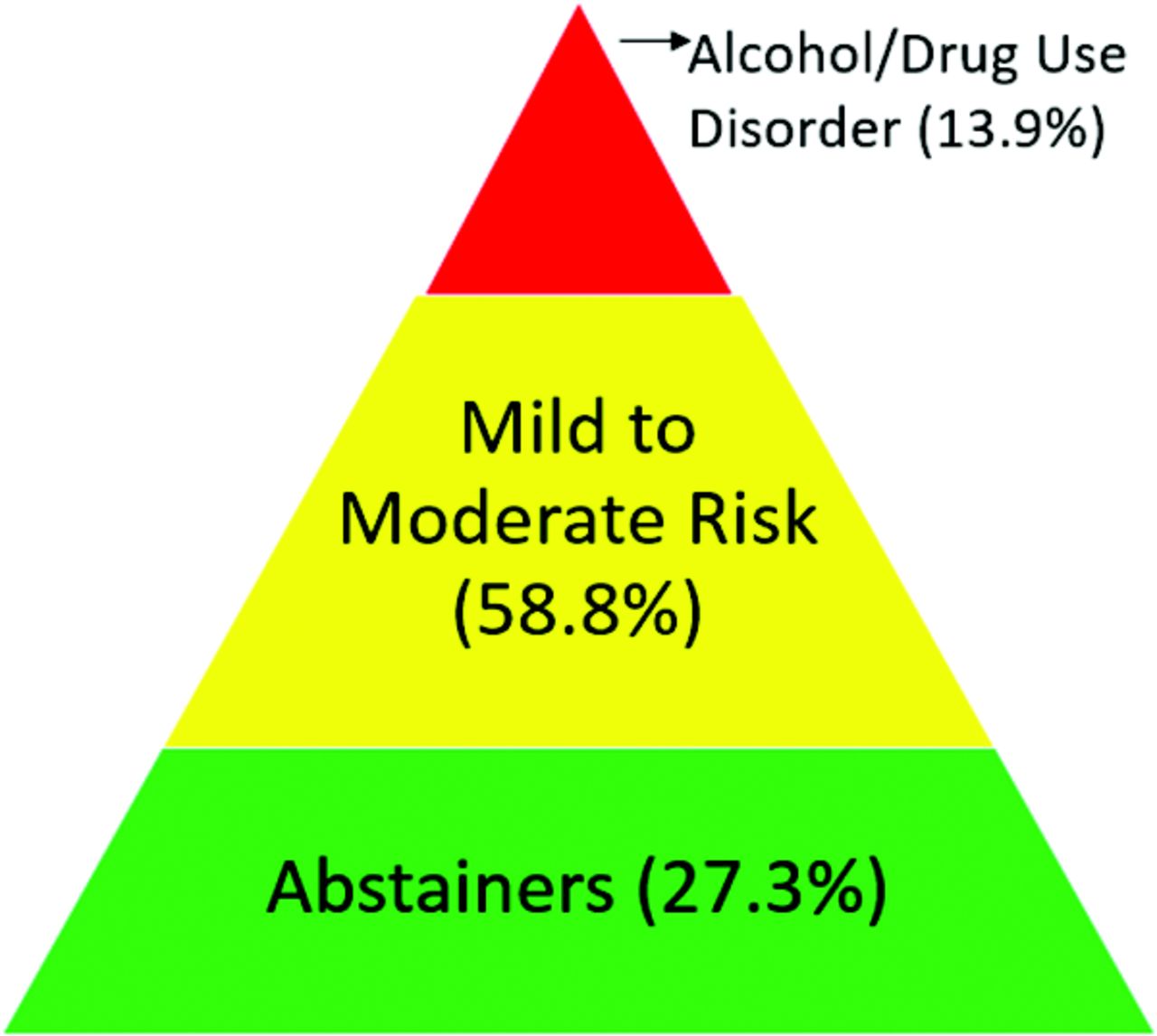
Efforts to assist primary care providers have addressed some, though certainly not all, of the existing barriers, such as time limits and lack of financial resources.7 Lengthy screening questionnaires have been reduced to a single question, motivational interviewing techniques have demonstrated effectiveness and can be deployed during the brief encounter, and patient-centered medical home models provide guidance about the integration of other practice staff in these efforts.8⇓⇓–11 Although these resource-focused solutions are helpful, they may not adequately acknowledge another important dimension of the SBI dissemination problem: the “prevention paradox.”12 The prevention paradox refers to research confirming that the majority of overall adverse health effects (eg, increased mortality, injury, and life problems)13, are attributable to a larger group (59%) of drinkers that fall into the low- or high-risk alcohol use categories compared with the 13.9% that meet past-year alcohol use disorder (AUD) criteria.14–15 These percentages of drinking practices have been commonly represented within a pyramid (see Figure 1). In practice, there may be a stronger emphasis on identifying and treating patients at the “tip of the pyramid” (eg, patients who meet criteria for AUD) while the guidelines emphasize that stronger evidence exists for SBI efforts for those at earlier stages.8 This potential misalignment of SBI counseling resources may help explain low rates of clinician self efficacy in managing patients with substance use disorders.1
In New Mexico, a geographically expansive state with both current and historically highest death rates from alcohol and drug overdose, the need to expand SBI is particularly urgent.16–17 We conducted a cross-sectional survey on SBI attitudes and practices among primary care clinicians in Research Involving Outpatient Settings Network (RIOS Net), a practice-based research network in New Mexico, serving low-income, predominantly Hispanic/Latinx and Native American communities. The aims of the survey were to characterize primary care clinician views about management of risky alcohol and drug use and explore their practices and perceived barriers to enhanced SBI practices in medically underserved communities. We compared views on alcohol versus opiate SBI. This survey represents the first step within a multi-stage research project toward identifying potential strategies to inform practice-based interventions aimed at expanding SBI to those patients in the middle of the pyramid.
Methods
Study Design and Setting
We conducted a cross-sectional survey of primary care providers in RIOS Net, a practice-based research network in New Mexico. We excluded pediatrician members of the network given our focus on the adult patient population. The study was approved by the University of New Mexico Human Research Protections Office.
Measures
The research team developed a survey to assess clinician approaches and attitudes to SBI for alcohol and opiate misuse in primary care settings in medically underserved communities (see Appendix 1 for the full survey). We reviewed substance abuse literature and consulted with clinicians who specialize in alcohol and drug use health services research to create the survey. We reviewed validated instruments to guide development of our final survey (eg, Organizational Readiness for Change18, Assessment of Chronic Illness Care18). A total of 6 RIOS Net Executive Board members and Department Family Medicine Residents piloted the survey. Survey items included scaled (visual analog 1 to 100, eg, 1 = not at all helpful or strongly disagree and 100 = significant or strongly agree), multiple choice, and 1 ranking of priorities question. Items focused on clinician ratings of the need to address substance use problems in primary care, current screening and intervention practices and satisfaction with and willingness to make changes to their practices.
Data Collection
We administered the provider survey electronically through Research Electronic Data Capture (REDCap19), a web-based electronic data capture program. Nonresponders were sent additional solicitations at 7-to-10-day intervals. After 5 e-mail solicitations, article surveys were mailed to nonresponders. This was followed by another mailing 2 weeks later. As an incentive, all respondents were entered into a pool and were eligible to win gift cards. The survey took approximately 15 minutes to complete and respondents earned 1.5 units of continuing medical education credits. At the conclusion of the survey, we included links (references on article-based questionnaires) to educational activities and clinical resources on SBI for alcohol and drug use. We exported the anonymous data for statistical and qualitative analysis.
Data Analysis
Responses from clinicians who used the web-based questionnaire were stored in the REDCap database. Article-based responses were double-entered by research staff into Microsoft Excel. Analyses of all data were done using Stata software. To report results of the survey, we calculated the mean and standard deviation of each continuous survey response. Further, we explored differences between continuous responses for alcohol versus opiates using paired t-tests. Categorical responses were summarized using frequencies. To explore differences between responses for alcohol versus opiates, the Stuart-Maxwell test, a generalization of McNemar's test for multiple categories, was used. For post-hoc analyses, we conducted ANOVAs to explore differences on survey responses based on years of practice. All statistical significance tests were 2-sided and conducted at the 0.05 significance level.
Results
Participants
The sampling frame consisted of 126 eligible clinician members of RIOS Net. The survey response rate was 55% (N = 69; 45% women). The sample is described in Table 1. On average, respondents were 51.7 years of age (SD = 9.2 years; range, 32 to 69 years) with 19.8 years of experience as a medical provider (SD = 10.0 years, range, 1 to 40 years). The majority of respondents were family physicians (68%) and were distributed across University of New Mexico (32%), Community Health Center (29%), and Indian Health Service (21%) outpatient primary care settings.
Summary of Health Professionals' Characteristics Expressed as Absolute Numbers and Percentage
Overall, in line with our research aims and emergent findings, these results are organized in 4 categories: 1) perception of the problem and level of prioritization, 2) reported SBI approaches, 3) considerations for practice changes, and 4) post-hoc exploratory analyses to examine variability in responses. Within each of these main categories, we present findings for addressing risky alcohol and opiate use followed by commonalities and differences in addressing these 2 substances. Table 2 presents survey item results.
Medical Provider Responses to Survey about Alcohol and Opiate Screening, Brief Intervention, and Referral to Treatment in Primary Care
Perception of Problem and Level of Prioritization
While not reaching statistical significance, we observed a trend toward providers reporting that opiate misuse was more of a problem in their patient population than was alcohol misuse (P = .054). Respondents more strongly agreed that addressing opiate use was a priority than addressing alcohol. This higher rating for opiates may be attributable to the significant escalation in prescription pain medication misuse and overdose death rate in New Mexico and the nation. Providers also rated the degree to which their clinic leadership prioritized these topics at the same level, with opiate use once again higher than for risky alcohol use.
Reported SBI Approaches
We asked a series of questions assessing the circumstances that lead to screening. Providers reported relying mostly on their clinical impressions based on individual patient characteristics to detect substance use problems in contrast with a universal screening system. They reported this case finding approach at higher levels for patients with opiate problems (65%) compared with alcohol problems (50%). However, when looking at clinician rates of screening for opiate misuse at all patient visits (15%) and for well visits (13%), the rates almost doubled for alcohol screenings (26% and 22%, respectively). Only about a quarter of respondents indicated that they screened patients at every visit (eg, universal screening) for alcohol and this rate was lower for opiates.
When asked about who initiates screening in the practice, clinicians reported doing so more often than nurses/medical assistants and/or having patients complete a screening questionnaire. Clinician-led screening was reported at a higher level for opiates (77%) than for alcohol (62%). Congruently, there was moderate agreement that screening was the clinician's responsibility. Perceptions of clinic staff investment in addressing alcohol and opiate problems were rated similarly at the midpoint of the range. Lastly, consistent with our interestin understanding how clinicians direct screening efforts along the pyramid, we asked respondents to rank priorities for alcohol screening. Providers ranked “people meeting criteria for alcohol use disorder” as the highest priority with the second highest rating for “patients with mild/moderate alcohol use” and lastly “patients with no current alcohol use problems; I focus on prevention” (see Table 3).
Medical Provider Rankings of How they Focus Their Screening Efforts
Most clinicians reported that they provided a mix of substance use interventions within the practice combined with referring to community resources at equal levels for both alcohol and opiate problems. Clinicians reported similar levels of awareness of community resources for these patients. About half of participants perceived that patients felt comfortable seeking treatment for alcohol or opiate use problems.
Considerations for practice changes
Only about half of clinicians felt strongly or somewhat satisfied with how their practice addressed patients with opiate use problems; slightly more were satisfied with their practice's management of alcohol use problems. Considering this lack of satisfaction, almost three quarters of these clinicians felt that making changes in practice approaches to these problems was important, and about the same percentage felt confident their practices could make the improvements needed (see Table 2). When asked about different strategies for improved care that might be considered, the highest level of interest was in increased coordination with community resources and learning collaborative approaches.
Post-hoc Analysis of Data Variation
We observed large variability across the visual analog questions (0 to 100), so we conducted post-hoc ANOVAs to examine potential clinician characteristics, including years of experience, for associations with screening attitudes and behaviors.20 We divided the groups into 3 categories based on years of practice: ≤ 10 years (Mdn1), 11 to 19 years (Mdn2), and ≥20 years (Mdn3). Four questions yielded significant differences in ratings based on years of practice : 1) practice staff felt invested in patients with alcohol problems (Mdn1 = 74, Mdn2 = 56, Mdn3 = 48; P = .011), 2) clinic leadership prioritized alcohol problems (Mdn1 = 80, Mdn2 = 54, Mdn3 = 50; P = .032), 3) increasing practice efforts to address alcohol problems was important (Mdn1 = 88, Mdn2 = 66.5, Mdn3 = 71; P = .027), and 4) noted interest in a collaborative approach care model (Mdn1 = 88, Mdn2 = 84, Mdn3 = 73; P = .035). Those with fewest years of practice rated these questions higher than those with more years of practice. For opiate-related questions, 1 significant difference: those with fewer years of practice noted interest in training on effective instruments to detect opiate use problems (Mdn1 = 80, Mdn2 = 73.5, Mdn3 = 66.5; P = .025).
Discussion
We surveyed primary care providers' perspectives and reported practices regarding SBI for risky alcohol and opiate use in a rural Southwestern, minority-majority state. In general, primary care providers reported alcohol and opiate use to be problems in their practice and mostly reported similar management approaches with both problems. Despite United States Preventive Services Task Force (USPSTF) recommendations for universal screening for alcohol misuse5, only a quarter of providers reported universal screening for alcohol. Low rates of universal screening are consistent with previous findings that only one third of adults reported their primary care providers asked about alcohol and drug use.20 Although the USPSTF does not endorse universal screening recommendations for drug use, 15% of our participants reported doing so for opiates. This is substantially lower than a national survey of physicians, which reported 68% asked new patients about illicit drug use.21 Most providers reported both relying on their clinical judgment to identify alcohol and opiate problems and focusing their efforts on patients at the extreme end of the alcohol use spectrum (ie, those at the “tip of the pyramid”).
While recognizing the important role that primary care providers play in addressing patients with severe substance use disorders (“tip of the pyramid”), there is a need to simultaneously refocus providers' efforts to patients in the middle of the pyramid in concordance with available evidence. Our findings reflect some of the known challenges associated with delivering SBI in primary care while also presenting a view of opportunities to make changes.
Collectively, our findings suggest that clinicians lead SBI efforts in their practice settings for select patients who they believe, based on clinical impressions, may be at a higher risk for a substance use disorder. At the same time, they endorsed survey items that may lead to enhanced attention to middle of the pyramid patients. Providers strongly endorsed collaborative care models and increased practice coordination with community resources as strategies to enhance SBI. Important for successful change, providers reported confidence in their ability to make practice-level changes. Clearly, these new models will be important in creating more comprehensive team-based changes aimed at broadening the scope of SBI to the middle levels of the pyramid.22
Our findings are consistent with emerging models of integrating primary care and behavioral health. Results from this survey suggest that efforts to increase coordinated care of this type are both desired and needed. Efforts should focus on both overcoming identified barriers as well as developing successful strategies for disseminating and implementing culturally appropriate SBIs.23–24 Strategies that may also be helpful to promote practice change include identifying practice “champions” of SBI25, ensuring training and dissemination of definitions of risky drinking; introducing evidence-based SBI approaches; updating practices on billing codes to cover SBI; and equipping providers with feasible SBI counseling techniques that fit the brief encounter.8,26⇓–28
While the lack of evidence to support screening for other drugs is problematic, our survey findings indicate that these providers are actively managing these patients and desire training and practice changes to improve care delivery. There has been a call for more research on screening for risky drug use to guide providers to improve patient care.29 Even in the absence of evidence to support action in screening for drug use, there still may be compelling and ethical reasons for medical providers to consider screening for drug use such as 1) prescription drug interactions, 2) health concerns, and the 3) alarming increase in opiate overdose and mortality.29
Cultural and Geographic Context
These survey findings reflect the views and experience of providers with large percentages of Hispanic/Latinx and Native American patients in New Mexico. Racial/ethnic populations experience substantial substance misuse related health disparities17,30, underlining the compelling need to find effective and feasible approaches to this problem in primary care. Extending SBI access and moving away from the tip of the pyramid in culturally diverse settings will likely require adapting or expanding current “best practices” to increase culturally appropriate SBI practices and patient receptivity. For instance, one screening study in a hospital setting found greater reductions in drinking and drug use among Non-Hispanic White and African American patients compared with Hispanic/Latino patients indicating potential differences across cultural groups.31 Future research should attend to the cultural context and various social determinants of health, such as poverty, discrimination, and neighborhood factors, to examine barriers and ways to facilitate culturally effective SBI.
Limitations
These findings on primary health care providers' perspectives on SBI and referral to treatment must be taken in the context of the limitations of the research. Although the response rate was acceptable, the sample size of providers was relatively small and based on respondents from a set of providers in underserved communities in New Mexico. These results may not generalize to other locations beyond the Southwest. However, clinician respondents were experienced (average, 20 years) and included statewide representation with patient population diversity. Finally, New Mexico consistently ranks high nationally in both prescription drug overdose and alcohol death rates. Therefore, developing a better understanding of clinician observations about SBI barriers and facilitators from these types of settings may offer greater potential to inform primary care practice change efforts.
Conclusion
Through this cross-sectional survey of SBI for alcohol and opiate misuse, we sampled clinicians in a practice-based research network primarily serving American Indian and Hispanic/Latinx populations and found low rates of universal screening practices. Most screening was targeted to specific individuals based on clinical judgment and these medical providers reported prioritizing screening patients with substance use dependence (the tip of the pyramid) rather than patients with risky substance use (the middle of the pyramid). One strategy that may help practices move to universal screening is to engage, as appropriate, other practice staff in coordinated screening models, while another may be through integration of behavioral health providers into primary care. Finally, given the alarming substance-related health disparities among racial/ethnic populations and other underserved groups16,17,30, future research is needed to examine cultural factors and social determinants of health that may influence the successful implementation and impact of SBI among our rapidly diversifying nation.
Acknowledgments
We gratefully acknowledge Drs. Lauren Hund and Betty Skipper for their assistance with statistical analyses.
Notes
This article was externally peer reviewed.
Funding: Research reported in this publication was supported by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under Award 1P20MD004811-01. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/31/2/243.full.
- Received for publication March 20, 2017.
- Revision received November 7, 2017.
- Accepted for publication November 13, 2017.




{kind=link}