
Abstract
Background: Clinicians strive to deliver individualized, patient-centered care. However, these intentions are understudied. This research explores how patient characteristics associated with an high risk-to-benefit ratio with hypoglycemia medications affect decision making by primary care clinicians.
Methods: Using a vignette-based survey, we queried primary care clinicians on their intended management of geriatric patients with diabetes. The patients' ages, disease durations, and comorbidities were systematically varied. Clinicians indicated whether they would intensify glycemic control by adding a second-line hypoglycemia medication.
Results: A convenience sample of 336 primary care clinicians completed the survey. Despite the recommendations for HbA1c targets <8% for more complex patients, an 80-year-old woman with an HbA1c of 7.5%, longstanding diabetes, coronary disease, and cognitive impairment and with instrumental activity of daily living dependencies, had a predicted probability of treatment intensification of 35%. Internists were 11% and nurse practitioners were 14% more likely to intensify treatment than family physicians (P < .01). These provider differences remained significant after controlling for geographic differences in treatment intensification. Providers in Florida were more likely to intensify treatment (P < .01).
Conclusions: Primary care clinicians often chose to intensify glycemic control despite individual patient factors that warrant higher glycemic targets based on existing guidelines. This research identifies possible missed opportunities for patient-centered goal setting and raises questions about the influence of training and practice environment on clinical decision making.
- Blood Glucose
- Clinical Decision-Making
- Diabetes Mellitus
- Geriatric Health Services
- Hyperglycemia
- Hypoglycemic Agents
- Patient-Centered Care
- Primary Health Care
Older adults with diabetes are at greater risk for adverse consequences of the disease, notably hypoglycemia, with tight glycemic control.1⇓–3 This is particularly true for older adults with long-standing diabetes, coexisting cardiovascular disease, or cognitive impairment. This iatrogenic risk also increases with age. The rate of hospitalization for hypoglycemia in diabetic patients aged ≥75 years is twice that of those aged 65 to 74, and rates of hospitalization for hypoglycemia now exceed those for hyperglycemia among the Medicare population.4
To avoid this harm, the American Diabetes Association (ADA)5,6 and the American Geriatric Society7,8 recommend tailoring glycemic targets based on a patient's life expectancy, number and severity of comorbid chronic diseases, and cognitive and physical functioning. According to the ADA guidelines for older adults6, glycohemoglobin (HbA1c) targets <7.5% are appropriate for older adults with few comorbid conditions and intact cognitive and physical functioning (healthy); targets <8% are appropriate for older adults with comorbid chronic diseases, impaired instrumental activities of daily living (IADLs), or mild to moderate cognitive impairment (complex/intermediate); and targets <8.5% are appropriate for patients with end-stage illness receiving long-term care, with moderate to severe cognitive impairment, or with impaired activities of daily living (very complex/poor health). The American Geriatric Society endorses this 3-tiered approach to glycemic management with a lower bound of 7% for all older adults and an upper bound of 9% for those with poor health and limited life expectancy.8
Despite all the effort that has gone into creating these consensus statements, a paucity of the literature examines how clinicians respond to these recommendations in practice when tailoring treatment for individual patients with diabetes. In this study we focus on community-dwelling older adults with diabetes who fit into the healthy and intermediate categories of clinical complexity and, per existing guidelines, should have HbA1c targets <7.5% (healthy) or <8% (complex/intermediate). We presented common patient scenarios to primary care clinicians, who most often manage older adults with diabetes, in order to investigate the effect of certain patient characteristics on their decision making. We specifically measured whether clinicians would chose to intensify treatment (defined as adding a second agent) and how this intensification varied by patient characteristics. We hypothesized that clinicians would treat more aggressively younger patients without cognitive impairment or a history of heart disease.
Methods
This study used a vignette survey of primary care clinicians, including internal medicine (IM) physicians, family medicine (FM) physicians, and nurse practitioners (NPs). A vignette was a 1-paragraph description of a common patient scenario. We systematically varied the patient characteristics to better understand whether clinicians individualize care and what patient factors drive these treatment decisions. Respondents were specifically asked whether they would add a second-line diabetes medication (intensify medication therapy) for a patient who had already been treated for 6 months with first-line metformin therapy.
Data and the Sample
A convenience sample was obtained primarily through the use of state licensure lists from Minnesota and Florida. We also had participants from 3 Agency for Health Care Research and Quality practice-based research networks (PBRNs) and a small state professional association meeting. To be eligible, physicians and NPs had to be actively practicing primary care medicine at least 75% of the time.
For the PBRNs, participants were contacted by the network director using a standardized e-mail invitation with an embedded link to complete the online survey. E-mail addresses of PBRN members were not released to investigators. For the clinician e-mails obtained through licensure lists, the study primary investigator (EMM) e-mailed clinicians directly using the same standardized e-mail invitation used by the PBRNs. All responses were collected anonymously using Qualtrics software. A small number of study participants completed the study in person while attending a state professional association meeting. This study was exempted from full review by the University of Minnesota Institutional Review Board Human Subjects Committee (study no. 1305E33481).
Vignette Design
The patient factors randomly varied in the vignettes were HbA1c level, age, disease duration, presence of cognitive impairment with IADL dependencies, and history of coronary artery disease with previous coronary artery bypass graft. Each of the 4 patient characteristics were presented at 2 HbA1c levels (Table 1), yielding a total of 16 possible vignette combinations. All vignettes depicted a hypothetical patient of the same sex, weight, kidney function, and ability to pay for medications. In addition, every patient had hypertension, mild neuropathic symptoms, no comorbid depression, and no activity of daily living dependencies. Each respondent viewed 4 randomly selected vignettes. Therefore, every clinician did not receive the same survey. A sample vignette and the response set are provided in the Appendix.
Description of Patient Characteristics Systematically Varied in Factorial Vignettes
Measures
Treatment intensification was defined as adding any 1 of 5 classes of approved second-line medication therapies. A dichotomous variable was created to indicate intensification of medication therapy. Any choice to add another medication was categorized as treatment intensification.
In addition to the vignette characteristics, we investigated the effects of several clinician characteristics on the decision to intensify treatment. Clinician training was defined using an item that asked respondents to self-identify as “physician, family medicine,” “physician, internal medicine,” “nurse practitioner,” or “other.” Clinicians were not specifically asked about specializations. Other clinician and practice characteristics were investigated: year in which the respondent finished professional education, average duration of a routine visit (minutes), and percentage of practice that is Medicare (<25%, 25–75%, >75%).
Analyses
We used bivariate analysis and multivariate regression to study the effect of vignette characteristics on the decision to intensify treatment. Because clinicians viewed >1 vignette, we used random effects probit, a regression model that accounts for correlations between responses from the same clinician, or clinician cluster effects. Vignette and clinician characteristics were entered into the model as fixed effects, with a random intercept for each clinician. The random effects model assumed that variation across respondents is not correlated with the independent variables included in the model (vignette factors). The Hausman test confirmed that this assumption held for the current analysis and that random effects was an appropriate model (P = .30, fail to reject null hypothesis that variation across respondents is correlated with predictors). We also were able to estimate the intraclass correlation, or the amount of total variation attributable to idiosyncratic clinician effects. All analyses were conducted using Stata software version 14.
Results
A total of 366 clinicians comprised the analytic sample. We excluded 30 surveys (8% of respondents) from the analytic sample because their self-reported specialty was “other” or not provided (n = 11), geriatric or palliative care (n = 9), or endocrinology or nephrology (n = 10). Although complete denominator information was not available, we estimated the response rates to be around 8% to 10% for respondents identified using licensure lists, 20% to 25% for those in the PBRNs, and >80% for the participants attending a local professional conference. Data were collected between August and December 2015.
Respondent characteristics for the 73 IM physicians, 108 FM physicians, and 155 NPs are provided in Table 2. Respondents completed their professional education (medical school for physicians) between 1955 and 2015 (median, 1996). IM physicians had, on average, 10 more years since finishing their education (median, 1986). NPs had fewer years since completing their professional education (median, 2003). Clinicians reported a mean duration of a routine visit at 23 minutes (range, 5–90 minutes). The mean duration of a routine visit was similar across clinician types. When asked to estimate the percentage of their practice comprising Medicare patients, 28% of sample reported <25% of their practice was Medicare patients, 20% reported >75% of their practice is Medicare, and most respondents (52%) had practices with between 25% and 75% Medicare patients. NPs were the most likely to report having >75% of their patient population enrolled in Medicare, followed by IM and FM physicians. Of the sample, 52% practiced in Florida, 25% practiced in Minnesota, and 23% practiced in other states (predominately Wisconsin and Colorado). FM physicians were mostly likely to practice in Minnesota. NPs were most likely to practice in Florida. Most of the sample (76%) was obtained using licensure lists from Minnesota and Florida.
Characteristics of Primary Care Clinicians Completing Survey
Effect of Patient Characteristics on the Decision to Intensify Treatment
Figure 1 presents unadjusted rates of treatment intensification by vignette characteristics at the 2 HbA1c levels considered in this vignette study (7.5% and 8.5%). An 80-year-old with long-standing diabetes was significantly more likely to have her treatment intensified than a 65-year-old with a short diabetes duration at both HbA1c levels (P < .01). At an HbA1c of 7.5%, the 80-year-old had her treatment intensified 39% of the time compared with 70% of the time for the 65-year-old. Hypothetical patients with cognitive impairment that affected IADLs were also significantly less likely to have their treatment intensified at both HbA1c levels compared with hypothetical patients without cognitive impairment. In vignettes, at an HbA1c of 7.5%, the patients with cognitive impairment had their treatment intensified 51% of the time compared with 61% of the time for patients without cognitive impairment (P < .05). Having a history of heart disease with previous coronary artery bypass graft did not affect the decision to intensify treatment at an HbA1c of 7.5%. At an HbA1c of 8.5%, patients with a history of heart disease were more likely to have their treatment intensified than those without a history of heart disease in the vignettes (89% vs 82%, respectively; P < .05).
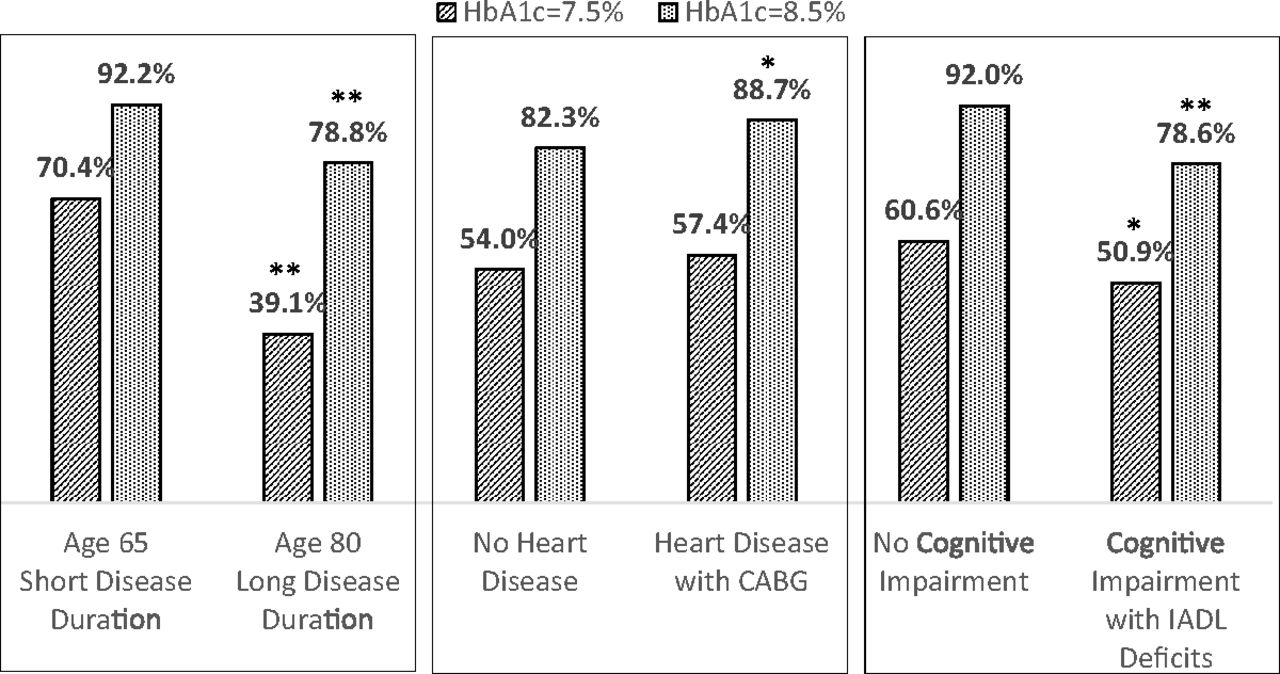
Unadjusted rates of treatment intensification by vignette characteristics at 2 glycohemoglobin levels. *P < .05; **P < .01. CABG, coronary artery bypass graft; HbA1c, glycohemoglobin; IADL, instrumental activities of daily living.
The effects of patient characteristics in the vignette on the decision to intensify treatment were similar in the adjusted models. Using random effects probit regression (Table 3, model 1), we found that having a higher HbA1c (8.5% vs 7.5%) increased the probability of treatment intensification by 32 percentage points. Being 80 years old decreased the probability of treatment intensification by 21 percentage points compared with being 65 years old. Having cognitive impairment decreased the probability of treatment intensification by 11 percentage points. Coronary artery disease was not significantly associated with the probability of intensification in the full model (P = .11).
Effect of Patient and Clinician Characteristics on Treatment Intensification
Effect of Clinician Characteristics on the Decision to Intensify Treatment
Most clinician characteristics we specifically measured in the survey were not related to the decision to intensify treatment (Table 3, model 2). Having a longer than average visit duration, a predominately Medicare patient population, or recent completion of professional education (within the past 5 years) did not significantly affect the decision to intensify treatment. However, we did observe differences in intensification by clinician type. FM physicians were significantly less likely than IM physicians or NPs to intensify medication therapy in geriatric patients. NPs were 14 percentage points more likely to intensify therapy than FM physicians; IM physicians were 11 percentage points more likely to intensify therapy than FM physicians (P < .01).
Some of this variation in intensification by clinician type may be better explained by geographic differences in practice patterns (Table 3, model 3). Over half of respondents to this survey and almost 75% of the NPs in the study practice in Florida. Practicing in Florida, compared with practicing in Minnesota or another state, increased the probability of treatment intensification by 14 percentage points (P < .01). After accounting for geographic differences in practice patterns, NPs were 7 percentage points more likely to intensify therapy than FM physicians; IM physicians were 8 percentage points more likely to intensify therapy than FM physicians (P < .05). Adding the source of the survey population (licensure vs PBRN or conference) was not significant once Florida was added to the model (results not shown). The interclass correlation reveals 59% of the variation (95% confidence interval [CI], 49–68%) in the decision to intensify medication therapy was due to unmeasured clinician characteristics.
Treatment Intensification for the Healthiest and Most Complex Hypothetical Patients
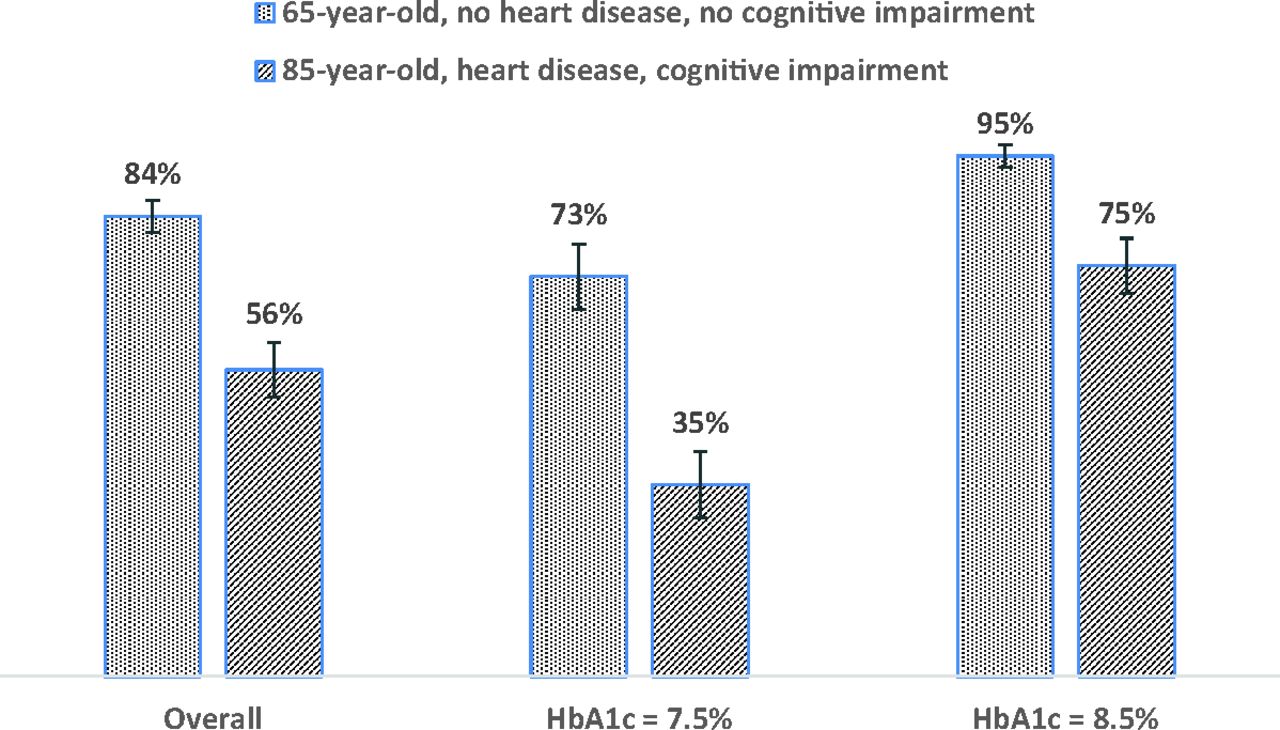
Figure 2 shows the predicted probability of treatment intensification for the healthiest and most complex hypothetical patients in the study at 2 HbA1c levels. A 65-year-old woman with a short diabetes duration and no heart disease or cognitive impairment had a mean predicted probability of treatment intensification of 73% (95% CI, 67–78%) at an HbA1c of 7.5%, and probability of 95% (95% CI, 93–97%) at an HbA1c of 8.5%. An 80-year-old woman with long-standing diabetes, coronary artery disease, and cognitive impairment with associated IADL impairment had a mean predicted probability of treatment intensification of 35% (95% CI, 29–41%) at an HbA1c of 7.5% and of 75% (95% CI, 70–80%) at an HbA1c of 8.5%.
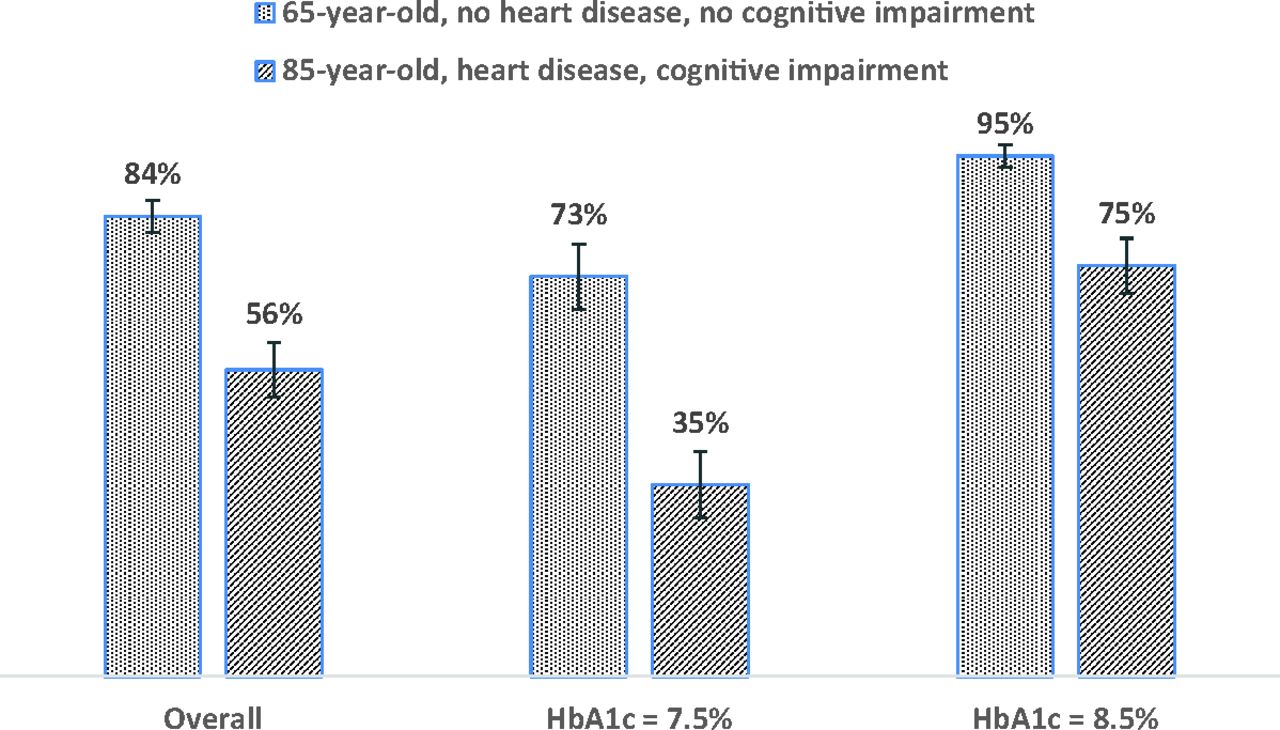
Predicted probability of treatment intensification for the healthiest and most complex cases presented in the vignettes, overall and at 2 glycohemoglobin levels. The graph shows the predicted probability of treatment intensification for a 65-year-old with short disease duration, no cognitive impairment, and no heart disease (healthiest vignette patient) compared with that for an 80-year-old with long-standing diabetes, cognitive impairment with impaired instrumental activities of daily living, and heart disease with previous bypass graft (most complex vignette). Marginal effects were estimated holding physician-level factors (longer than average visit length, ≥75% of practice comprising Medicare patients, completed education in the past 5 years, clinician type, and state where the physician practices). HbA1c, glycohemoglobin.
Discussion
The ADA guidelines for older adults6 recommend HbA1c targets <7.5% for older adults with few comorbid conditions and intact cognitive and physical functioning, and targets <8% for older adults with comorbid chronic diseases, impaired IADLs, or mild to moderate cognitive impairment. In this vignette-based study, we observed appropriately high rates of treatment intensification for relatively younger patients with few comorbid conditions and intact physical and cognitive function. For otherwise healthy older adults, the mean predicted probability of treatment intensification was 73% (95% CI, 67–78%) at an HbA1c of 7.5% and was 95% (95% CI, 93–97%) at an HbA1c of 8.5. However, we also detected potential missed opportunities to provide guideline-consistent care for older patients with comorbid cognitive impairment. An 80-year-old woman with long-standing diabetes, coronary artery disease, and cognitive impairment with associated IADL impairment had a mean predicted probability of treatment intensification of 35% (95% CI, 29–41%) at an HbA1c of 7.5%, despite the fact that the guidelines suggest an appropriate HbA1c target <8%.
Contrary to expectations, preexisting cardiac complications did not decrease the likelihood that clinicians would intensify treatment in this study. Post hoc analyses of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial and the Veteran's Affairs Diabetes Trial (VADT) suggest that tight glycemic control may confer additional risk of death for people with preexisting cardiovascular risk with long-standing diabetes.9,10 More research is needed to understand why the presence of coexisting coronary artery disease, which is specifically mentioned in existing guidelines, did not affect clinician behavior in the current study.
Our findings also hint at differences in treatment intensification by clinician type and/or by state. Overall, FM physicians were about 8 percentage points less likely than IM physicians and NPs to intensify glycemic medications. This is after controlling for a large, state-level difference in intensification between Florida and other states involved in the study (mainly Minnesota and Wisconsin). As the geriatric population continues to grow and the primary care workforce shortage deepens, the need increases for evaluation of practice patterns and patient outcomes associated with clinician type.11 Given the dramatic increase in the number of Medicare beneficiaries treated by NPs12, and given that Florida is second only to California in the number of Medicare beneficiaries, additional research is warranted to disentangle training and state effects. If clinician-type differences are replicated, policy and workforce deployment strategies may look to family medicine training programs to identify and leverage factors that promote individualized care for older adults with multiple chronic conditions.
Given the convenience nature of the sample and the low response rates, we have to be careful when interpreting and generalizing findings. In particular, we need to consider the effects of nonresponse error and coverage bias. Nonresponse error occurs when people who respond to the survey are different from those who do not respond. Clinicians who provide accurate e-mail addresses during licensure are likely different from those who do not, and clinicians who respond to unsolicited e-mails to complete surveys without a financial incentive are different from those who do not. We suspect that clinicians attending a regional conference, participating in PBRNs, or responding to an unsolicited request for help with a survey about diabetes care may be more familiar with the existing patient-centered guidelines than other clinicians. If this is the case, our estimates of potential overtreatment, or missed opportunities to follow existing recommendations for older adults, may be conservative. We also have some coverage bias. With the licensure lists, we started out with e-mails for approximately 60% of licensed primary care clinicians in Florida and Minnesota. However, 5% to 10% of these E-mails were not active, and we were unable to estimate the percentage of remaining e-mails that were actually monitored (vs “junk e-mails”). Therefore, caution should be used when generalizing these findings to the population of all licensed primary care clinicians in those states or to all clinicians of a certain discipline.
However, with those generalizability caveats, vignette studies have been shown to be good predictors of how clinicians will behave in clinical settings.13 By systematically varying factors in existing guidelines, factorial vignette surveys are a cost-effective way to broadly understand practice patterns and compliance with quality initiatives. Our estimates of potential missed opportunities are closely aligned with recent survey results revealing that one third of primary care clinicians thought it would be difficult to follow the Choosing Wisely HbA1c recommendation for older adults, which asks clinicians to “Avoid using medications other than metformin to achieve hemoglobin A1c <7.5% in most older adults.”14 As part of the same study, clinicians reported existing pay-for-performance (P4P) initiatives tied to lower HbA1c levels and fear of potential litigation as reasons they may not reduce medication burden as a person develops additional comorbid complications that limit life expectancy.14 P4P or pay-for-quality incentives rewarding intermediate outcomes (HbA1c levels) below a certain threshold (eg, <8%) are widespread.15,16 Policy options to address overtreatment include incentives to appropriately deintensify treatment17 or to decrease rates of hypoglycemia.18 It is important that we align incentives to provide appropriate care throughout the implementation and evaluation of the Merit-Based Incentive Payment System.19
Finally, our study shows that 59% of the variation in the decision to intensify medication therapy was not related to the factors mentioned in the existing patient-centered guidelines (age, disease duration, cognitive impairment, and cardiac complications) or to the clinician factors we measured. We are left to speculate as to the other factors affecting primary care clinicians' decisions to intensify glycemic medication therapy. In addition to P4P incentives, these “other factors” likely include the influence of training/mentorship20, environmental or regional variation in medication use (we found some evidence of state variation in the current study)21, influence of drug companies on individuals22,23, or habitual prescribing behavior.24 These factors are likely to affect the degree of success we have implementing current (or future) guidelines and therefore deserve careful consideration and more research.
Our findings add to an important and growing body of evidence of missed opportunities to consider comorbid conditions indicating higher glycemic targets in order to avoid known harms.1,4,14,25⇓⇓–28 In addition, factorial vignettes may serve as a tool for identifying and providing feedback to individual clinicians and health care systems regarding the (under)value placed on individualized, patient-centered care. Future research should further investigate the process and influences on clinician decision making regarding individualizing glucose targets for high-risk geriatric patients, including the influence of training and practice environment. The policy implications are substantial, including the construction of performance incentives, quality reporting, and primary care workforce recommendations.
Notes
↵† Died March 6, 2017.
This article was externally peer reviewed.
Funding: EMM is supported by an Agency for Healthcare Research and Quality National Research Service Award (4T32 HS000011-30).
Conflict of interest: none declared.
To see this article online, please go to: http://jabfm.org/content/31/2/192.full.
- Received for publication March 30, 2017.
- Revision received October 19, 2017.
- Accepted for publication October 29, 2017.




{kind=link}
{kind=link}