
Article Figures & Data
Figures
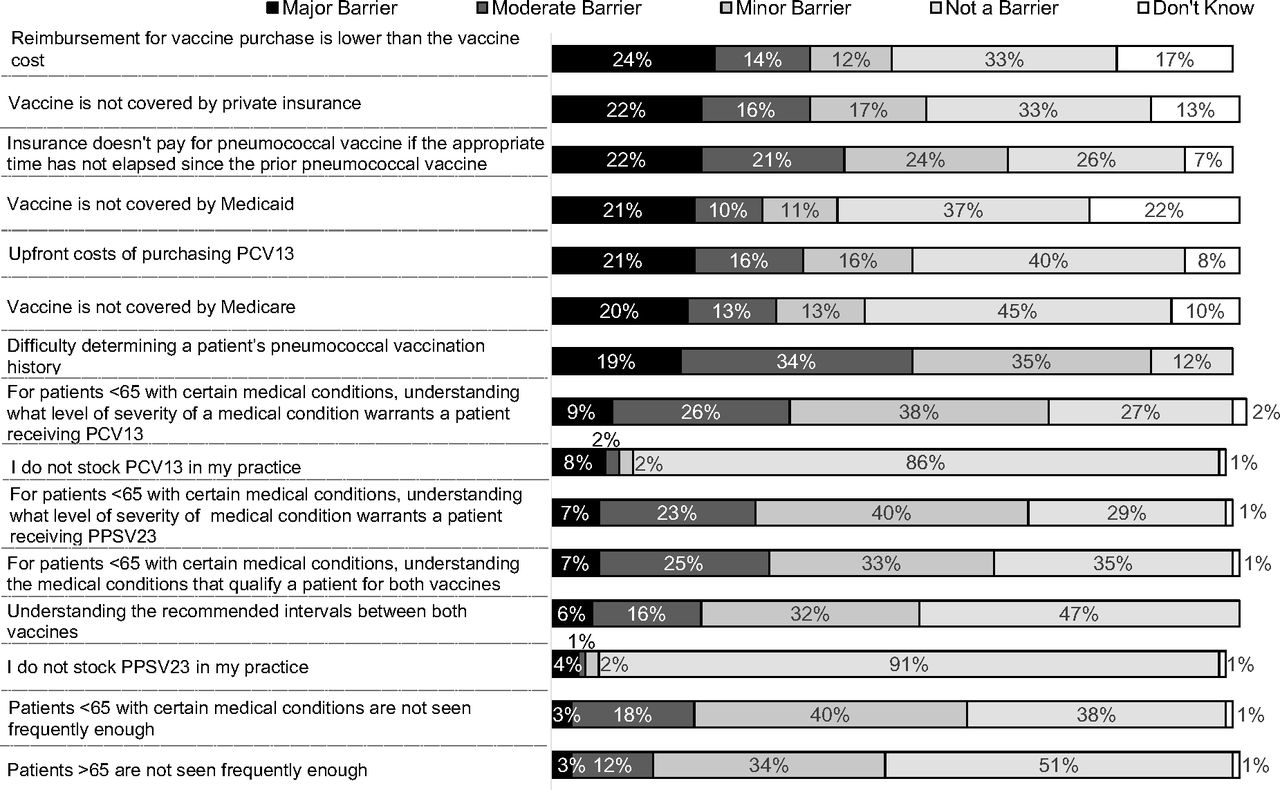
- Figure 1.
Physician-reported barriers to following Advisory Committee on Immunization Practices recommendations for giving pneumococcal conjugate vaccine (PCV13) and pneumococcal polysaccharide vaccine (PPSV23) in series, United States, 2016 (n = 602).
Tables
- Table 1.
Timeline of Advisory Committee on Immunization Practices Adult Pneumococcal Vaccination Recommendations*
Year Adult Pneumococcal ACIP Recommendations References 1984 PPSV23 recommended for adults aged ≥65 years 3 1989 In addition to adults ≥65, PPSV23 also recommended for- Adults aged 19 to 64 years with chronic illness, including cardiovascular disease, pulmonary disease, diabetes mellitus, alcoholism, cirrhosis, CSF leaks
Adults aged 19 to 64 years with immunocompromising conditions, including splenic dysfunction, anatomic asplenia, Hodgkin disease, lymphoma, multiple myeloma, chronic renal failure, nephrotic syndrome, organ transplantation, HIV
4 1997 Added specificity to previous indications: Cardiovascular disease to include congestive heart failure and cardiomyopathies
Chronic pulmonary disease to include chronic obstructive pulmonary disease and emphysema, but not asthma
5 Added PPSV23 recommendation for adults aged 19 to 64 years who live in an environment in which the risk of invasive pneumococcal disease or its complications is increased (eg, Alaskan Natives and certain American Indian populations, and patients in nursing homes)
have generalized malignancy
receive immunosuppressive chemotherapy
Added recommendation for revaccination with PPSV23 in 5 years for adults aged 19 to 64 years with immunocompromising conditions Added the concept of revaccinating adults ≥65 years who had received a dose of PPSV23 at an age <65 as long as 5 years have elapsed since the first vaccination 2010 PPSV23 recommended for adults aged 19 to 64 years who have asthma
smoke cigarettes
6 PPSV23 no longer recommended for Alaskan Natives or American Indians unless another indication for PPSV23 is present 2012 PCV13 recommended in series with PPSV23 for high-risk adults aged ≥19 years (those with immunocompromising conditions, functional or anatomic asplenia, CSF leaks, or cochlear implants) Pneumococcal vaccine–naïve persons should receive PCV13 first, followed by PPSV23 8 weeks later
If previously vaccinated with PPSV23, should receive PCV13 dose ≥1 year after PPSV23 dose
No changes to previously recommended doses of PPSV23
9 2014 PCV13 recommended in series with PPSV23 for all adults aged ≥65 years Pneumococcal vaccine–naïve persons should receive PCV13 first, followed by PPSV23 6 to 12 months later
If previously vaccinated with PPSV23, give PCV13 ≥1 year after receipt of the most recent PPSV23 dose
11 2015 Changes to recommended intervals between PCV13 and PPSV23 1-year interval recommended between PCV13 and PPSV23, regardless of which vaccine given first, for immunocompetent adults aged ≥65
12 ↵* Numerical references relate to the numerical references at the end of the manuscript.
ACIP, Advisory Committee on Immunization Practices; CSF, cerebrospinal fluid; PCV13, 13-valent pneumococcal conjugate vaccine; PPSV23, 23-valent pneumococcal polysaccharide vaccine.
- Table 2.
Case-Based Questions Aimed to Assess Knowledge of Advisory Committee on Immunization Practices Adult Pneumococcal Vaccine Recommendations
Question Answer Options* 1. A 65-year-old healthy woman with no history of prior pneumococcal vaccination sees you for an annual wellness visit. Which, if any, pneumococcal vaccine(s) should be administered at this visit? PPSV23
PCV13
None
Both
I would need to look this up
2. A 24-year-old man sees you for a routine office visit. He has asthma and has not previously received any pneumococcal vaccines. Which, if any, pneumococcal vaccine(s) should be administered at this visit? PPSV23
PCV13
None
Both
I would need to look this up
3. A 28-year-old woman with HIV infection sees you for a routine visit. She received 1 dose of PPSV23 1 year ago. Which, if any, pneumococcal vaccine(s) should be administered at this visit? PPSV23
PCV13
None
Both
I would need to look this up
4. A 42-year-old man with nephrotic syndrome sees you for a routine visit. He has not previously received any pneumococcal vaccines. Which, if any, pneumococcal vaccine(s) should be administered at this visit? PPSV23
PCV13
None
Both
I would need to look this up
5. A 66-year-old man with chronic heart disease sees you for a routine visit. He received 1 dose of PPSV23 at age 64. At what age, if at all, should he receive another dose of PPSV23? 66
67
69
75
I would need to look this up
6. A 42-year-old man with cochlear implants sees you for a routine visit. He had received a PCV13 vaccine at his otolaryngologist's office the day before. When should a PPSV23 vaccine be administered? Never; the patient does not need a PPSV23
At least 8 weeks after the PCV13 vaccine
At least 1 year after the PCV13 vaccine
At least 5 years after the PCV13 vaccine
I would need to look this up
7. A 67-year-old man with hypertension presents for a medication refill. You notice he received a PCV13 vaccine 6 months ago but has not received a PPSV23 vaccine. When should he receive the PPSV23 vaccine? Never; he does not need to receive PPSV23
Today
In 6 months
Five years after he received the PCV13 vaccine
I would need to look this up
8. A 45-year-old woman with a history of idiopathic thrombocytopenic purpura was vaccinated with PPSV23 vaccine before her splenectomy at age 43, and with the PCV13 vaccine last year. When should this patient receive her next dose of PPSV23 vaccine? Never; she does not need another dose of PPSV23
Five years after her first dose of PPSV23 vaccine
Today
When she is 65 years old
I would need to look this up
↵* Correct answers are boldface.
PCV13, 13-valent pneumococcal conjugate vaccine; PPSV23, 23-valent pneumococcal polysaccharide vaccine.
- Table 3.
Demographic and Practice Characteristics of Survey Respondents in a Study of Physicians' Perspectives on Adult Pneumococcal Vaccine Recommendations, United States, 2016
Characteristics Respondents (n = 617) Nonrespondents (n = 318) Age (years), mean (SD)* 53.5 (8.6) 55.3 (8.3) Male* 54.1 63.1 Specialty Family physician 47.5 50.9 General internist 52.5 49.1 Region* Midwest 27.1 21.7 Northeast 18.2 19.8 South 31.4 39.9 West 23.3 18.6 Location of practice Urban 47.2 44.7 Suburban 48.1 49.7 Rural 4.7 5.7 Setting Private practice 71.5 78.9 Hospital/clinic 22.2 14.5 HMO 6.3 6.6 No. of providers in the practice 1 12.4 18.3 2–4 25.1 27.7 5–10 32.3 30.9 ≥10 30.2 23.2 Physicians providing vaccines to adults 97.6 N/A Practice uses an EMR/EHR 93.6 N/A Proportion of patients aged ≥65 <10% 5.0 N/A 10–24% 17.4 N/A 25–49% 38.7 N/A ≥50% 38.9 N/A Practice accepts Medicare 94.8 N/A Practice accepts Medicaid 71.9 N/A Data are percentages unless otherwise indicated.
↵* P < .05 for sex, practice setting, region of country, number of providers, and mean age between respondents and nonrespondents (χ2, Mantel-Haenszel χ2, and t tests were used).
EHR, electronic health record; EMR, electronic medical record; HMO, health maintenance organization; N/A, not applicable; SD, standard deviation.
- Table 4.
Physician Knowledge of Adult Pneumococcal Vaccine Recommendation, United States, 2016 (n = 602)
Knowledge Concept Correct (%) Incorrect (%) Would Need to Look This up (%) Which pneumococcal vaccine should be given first to adults aged ≥65? 83 14 3 Qualifying conditions for PCV13 for patients aged <65 (HIV) 75 11 14 Interval between PCV13 and PPSV23 in immunocompetent adults aged ≥65 65 29 6 Interval between 2 PPSV23 doses when received at age <65 and patient is now aged ≥65 64 25 11 Which pneumococcal vaccine should be given first to a patient aged <65 with a qualifying condition (nephrotic syndrome) 54 30 16 Qualifying condition for PPSV23 in a patient aged <65 (asthma) 47 42 11 Interval between 2 PPSV23 doses in a patient aged <65 and who has a qualifying condition (splenectomy) 46 40 15 Interval between PCV13 and PPSV23 in patients aged <65 who have a qualifying condition (cochlear implant) 22 58 20 Some percentages do not add up to 100% because of rounding.
PCV13, 13-valent pneumococcal conjugate vaccine; PPSV23, 23-valent pneumococcal polysaccharide vaccine.




{kind=link}