
Article Figures & Data
Figures
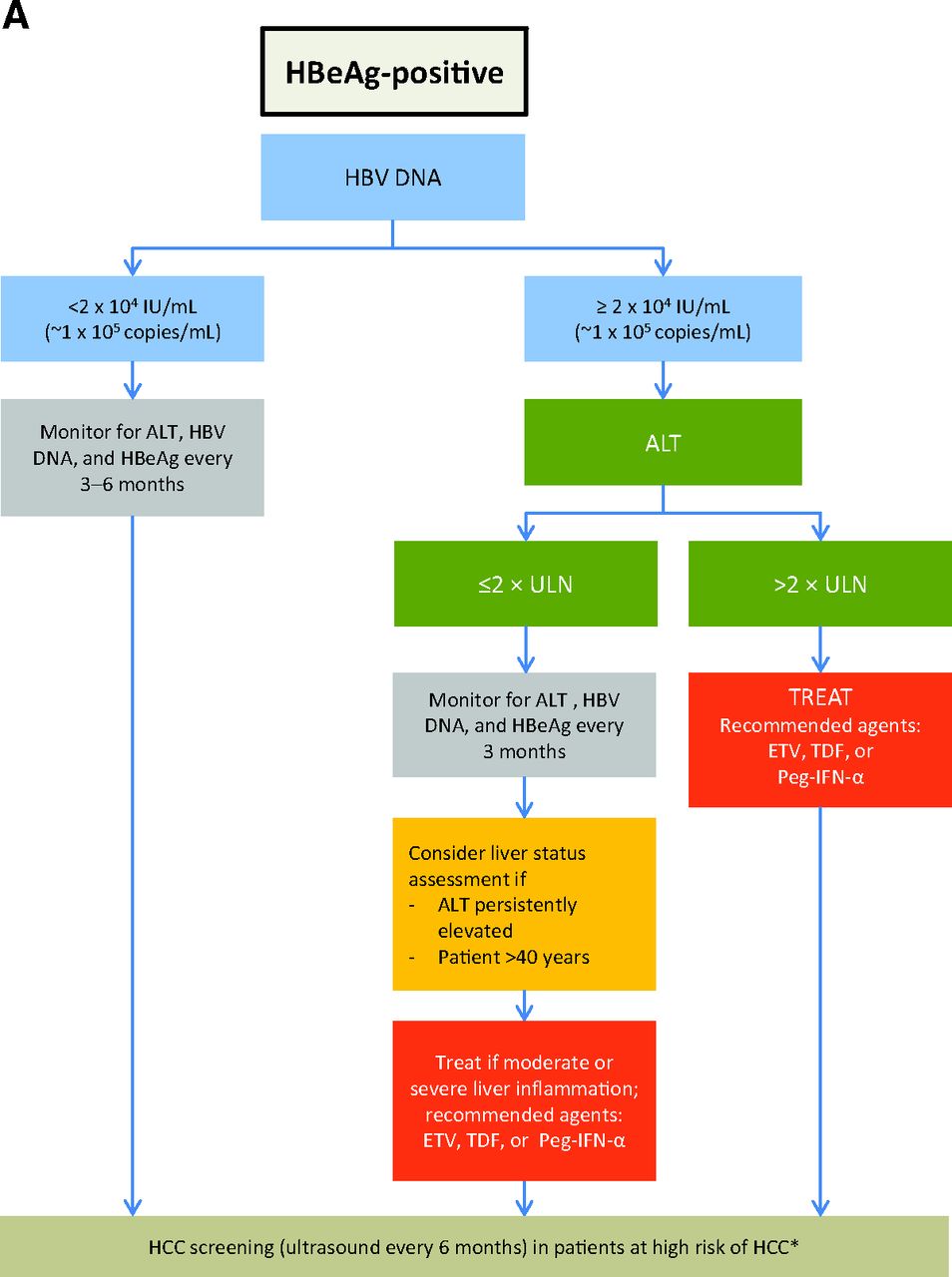
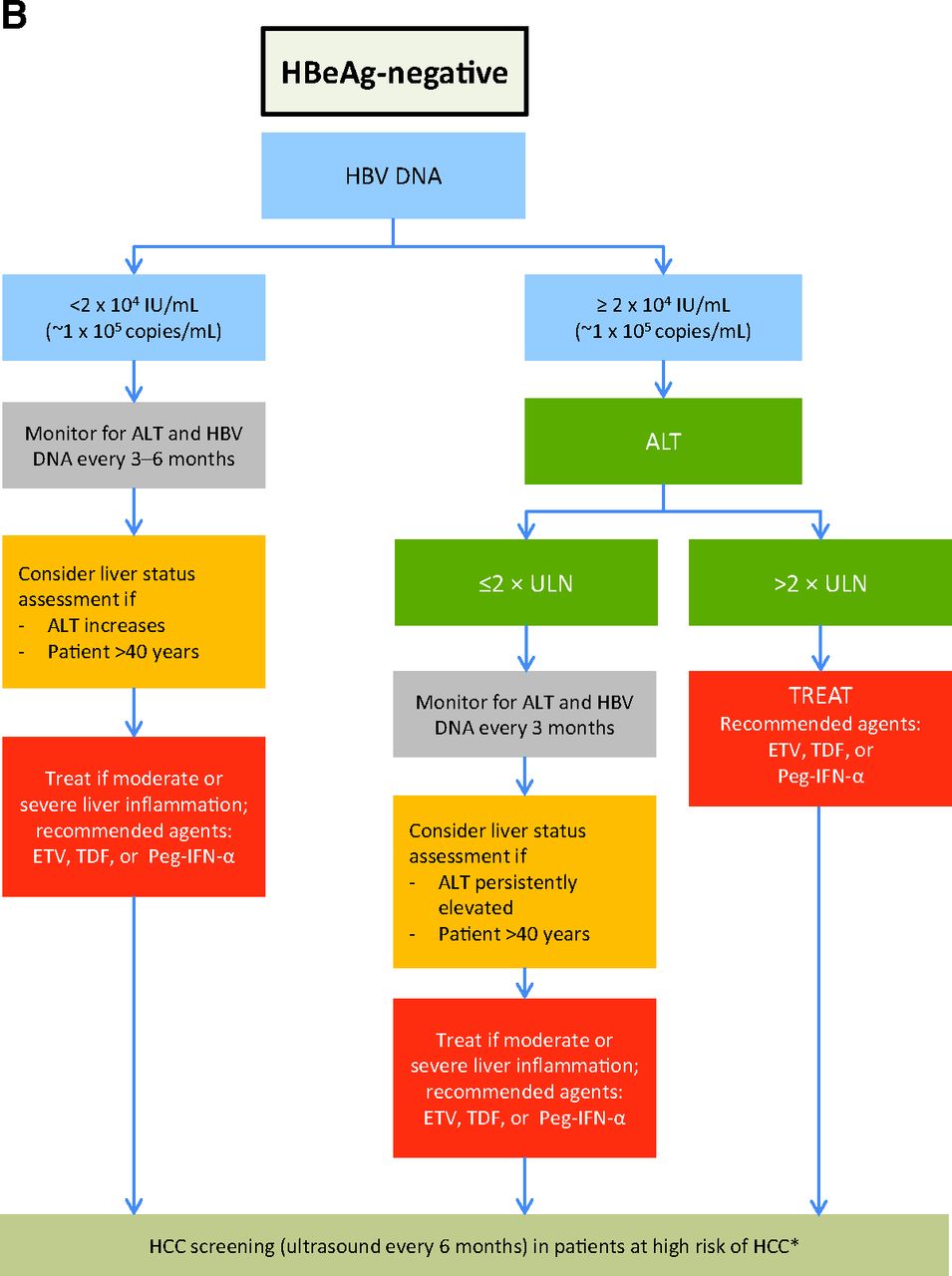
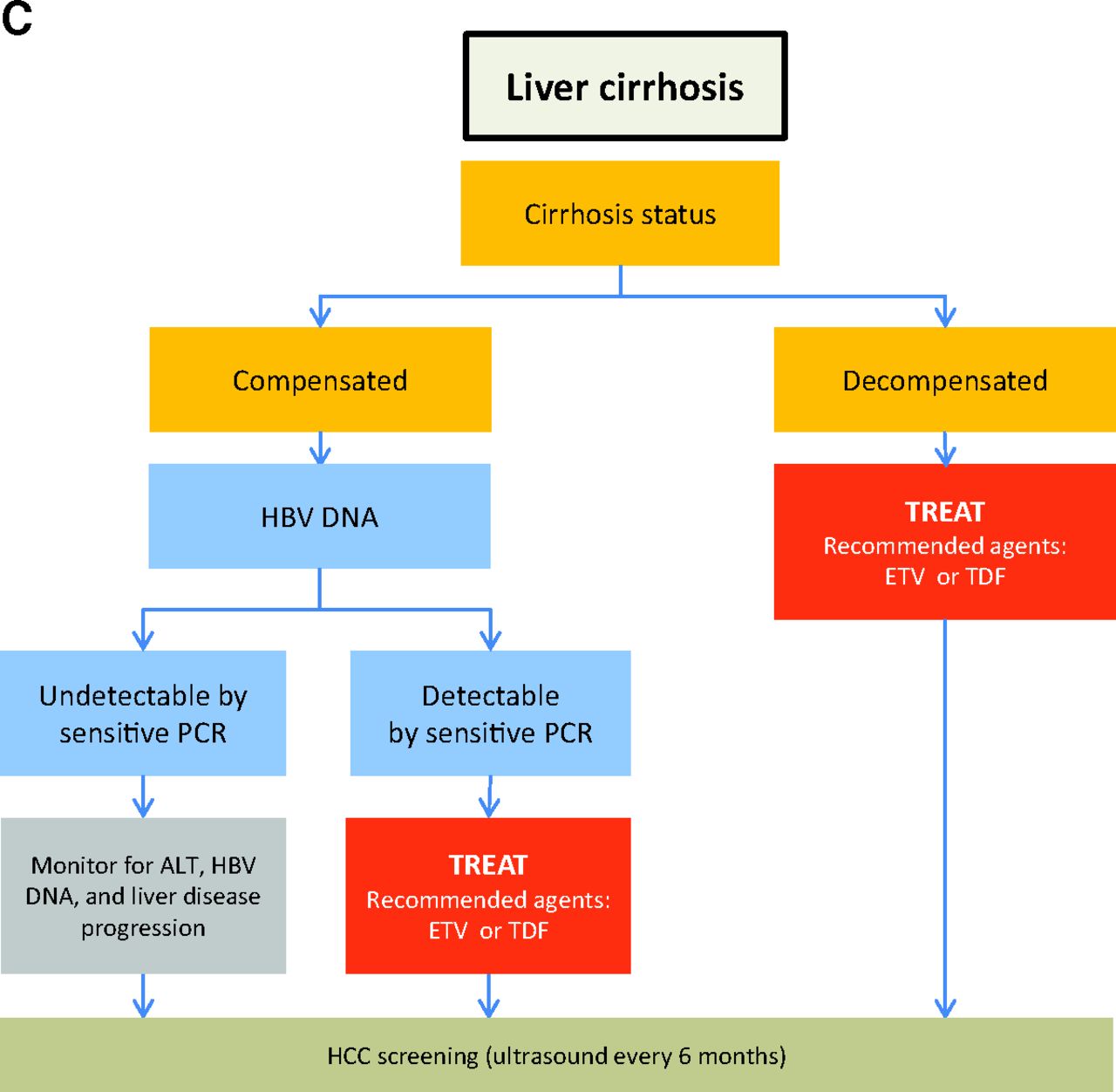
- Figure 1.
Treatment algorithm for patients with chronic hepatitis B (CHB) who have hepatitis B e antigen (HBeAg)–positive disease (A), HBeAg-negative disease (B), or cirrhosis (C). The strength of all recommendations is A (based on guidelines for management of CHB from the American Association for the Study of Liver Diseases, the European Association for the Study of the Liver, and the Asian Pacific Association for the Study of the Liver10–12). Alanine aminotransferase (ALT) upper limit of normal (ULN): 19 IU/mL in women, 30 IU/mL in men. Sensitive real-time polymerase chain reaction (PCR): lower limit of detection, ∼5-10 IU/mL; lower limit of quantification, ∼30 IU/mL. *See the text for definition of patients at high risk of hepatocellular carcinoma (HCC). ETV, entecavir; HBV, hepatitis B virus; Peg-IFN-α, pegylated interferon-α; TDF, tenofovir.



Tables
- Table 1. Characteristics and Clinical Prognosis of the Different Phases of Chronic Hepatitis B Infection
CHB Phase Serum HBV DNA (IU/mL) HBeAg Anti-HBeAg HBsAg, log10 (IU/mL) ALT* Liver Disease Precore/Core Promoter HBV Variant Age (Years) Prognosis Immune tolerant >2 × 106–7 + − 4.5–5.0 Normal None/minimal WT <20–25 No or minimal liver disease development as long as ALT remains normal Immune clearance (HBeAg-positive disease) 2 × 104–5 + − 3.0–4.5 Persistently or intermittently elevated (>2× ULN), ALT flares possible (>5× ULN) Possible necroinflammation; may lead to fibrosis or cirrhosis if HBeAg-positive phase is prolonged WT > mutant 20–40 Favorable prognosis if HBeAg seroconversion occurs (inactive carrier state) The shorter the duration of the immune clearance phase, the better the prognosis and the lower the risk of liver disease development or progression Inactive carrier <2 × 103 − + 1.5–3.0 Normal Necroinflammation may disappear; halt of any liver disease progression WT > mutant (stable inactive carriers) >35–40 Favorable prognosis, unless advanced fibrosis/cirrhosis has developed during the HBeAg-positive phase Mutant > WT (patients who will undergo reactivation) Reactivation (HBeAg-negative disease) Fluctuating, >2 × 103–4 − + 2.5–4.0 Persistently or intermittently elevated Advanced Mutant >> WT >35–40 May lead to fibrosis progression or cirrhosis Data compiled from Liaw et al,11 Liaw,22 and Kwon and Lok.23
↵* Alanine aminotransferase (ALT) upper limit of normal: 19 IU/mL in women, 30 IU/mL in men.
CHB, chronic hepatitis B; HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; ULN, upper limit of normal; WT, wild type.
- Table 2. Summary of Anti–Hepatitis B Virus Treatment Indications as Recommended by Major Practice Guidelines
Practice Guidelines AASLD10 APASL11 EASL12 HBeAg-positive ∙ HBV DNA >20,000 IU/mL
∙ ALT >2× ULN
∙ No spontaneous HBeAg seroconversion after 3–6 months' observation∙ HBV DNA ≥20,000 IU/mL
∙ ALT ≥2× ULN∙ HBV DNA >20,000 IU/mL
∙ ALT >2× ULN∙ HBV DNA >20,000 IU/mL
∙ ALT ≤2× ULN
∙ Moderate or worse liver inflammation or significant fibrosis (on biopsy*)∙ HBV DNA ≥20,000 IU/mL
∙ ALT ≥1 to <2× ULN
∙ Moderate or worse liver inflammation or fibrosis (on biopsy or noninvasive fibrosis assessment*)∙ HBV DNA >2000 IU/mL
∙ ALT >1× ULN
∙ Moderate or worse liver inflammation or moderate fibrosis (using a standardized scoring system†)∙ HBV DNA >2000 IU/mL
∙ Cirrhosis∙ HBV DNA ≥2000 IU/mL
∙ Advanced fibrosis/cirrhosis∙ Detectable HBV DNA
∙ CirrhosisHBeAg-negative ∙ HBV DNA >20,000 IU/mL
∙ ALT >2× ULN∙ HBV DNA ≥2000 IU/mL
∙ ALT >2× ULN∙ HBV DNA >20,000 IU/mL
∙ ALT >2× ULN∙ HBV DNA >2000 IU/mL
∙ ALT ≥1–2× ULN
∙ Moderate or worse liver inflammation or significant fibrosis (on biopsy)∙ HBV DNA ≥2000 IU/mL
∙ ALT ≥1 to <2× ULN
∙ Moderate or worse liver inflammation or fibrosis (on biopsy or noninvasive fibrosis assessment*)∙ HBV DNA >2000 IU/mL
∙ ALT >1× ULN
∙ Moderate or worse liver inflammation or moderate fibrosis∙ HBV DNA >2000 IU/mL
∙ Cirrhosis∙ HBV DNA ≥2000 IU/mL
∙ Advanced fibrosis/cirrhosis∙ Detectable HBV DNA
∙ Cirrhosis↵* Assessment of liver disease is recommended if the patient is 40 years or older.
↵† Assessment of liver disease is recommended if the patient is 30 years or older. Biopsy is to be considered in patients of older age and/or with fluctuating/minimally elevated alanine aminotransferase (ALT) concentrations or family history of hepatocellular carcinoma.
AASLD, American Association for the Study of Liver Diseases; APASL, Asian Pacific Association for the Study of the Liver; EASL, European Association for the Study of the Liver; HBeAg, hepatitis B e antigen; HBV, hepatitis B virus; ULN, upper limit of normal.
- Table 3. Recommendations for the Management of Chronic Hepatitis B Infection in Special Patient Populations
Patient Population Key Issues Recommendations Decompensated liver disease* ∙ Higher risk of cirrhosis, HCC, and mortality
∙ Often associated with comorbidities such as renal dysfunction, protein malnutrition, or vitamin deficiencies∙ Treatment is indicated irrespective of HBV DNA levels to improve clinical status
∙ Recommended agents: ETV and TDF (well tolerated and shown to improve liver status)
∙ Regular monitoring of renal function and lactic acidosis recommended during ETV or TDF therapy
∙ IFNs contraindicated; they may increase risk of sepsis and decompensationHCV, HDV, or HIV coinfection ∙ Multiple viruses to be managed
∙ Higher risk of cirrhosis, HCC, and mortality∙ Treatment should target the dominant virus
∙ In HIV coinfection, LVD and TDF are active against both HBV and HIV; ETV is not recommended unless the patient also receives HAART
∙ Peg-IFN only drug effective against HDV
∙ Some reports of renal toxicity with TDF in HBV/HIV-coinfected patientsLT recipients ∙ Risk of HBV reactivation ∙ Anti-HBV prophylaxis before and/or after LT recommended
∙ HBIg with or without LVD historically is the most common approach; however, there is no consensus on HBIg dose and duration (that is, long-term low dose vs. short-term high dose; HBIg withdrawal; on-demand HBIg on NUC maintenance)
∙ Alternative prophylactic regimens: ETV or TDF, alone or combined with HBIgImmune-suppressive or chemotherapy ∙ Risk of HBV reactivation ∙ In HBsAg-positive patients, preemptive NUC therapy should be initiated at the onset of immunesuppressive or chemotherapy to prevent HBV reactivation
∙ In anti-HBc-positive patients receiving rituximab, anti-HBV prophylaxis is recommendedPregnancy ∙ Risk of perinatal infection from highly viremic mothers
∙ Risk of fetal damage∙ IFN-based therapy is contraindicated because of its antiproliferative effect
∙ LdT and TDF are classified as category B (no risk in animal studies but unknown in humans)
∙ LVD, ADV, and ETV are classified as category C (teratogenic in animals, unknown in humans)Pediatric patients ∙ Infection at an early age is associated with an increased risk of long-term complications
∙ Long-term safety and drug resistance are important concerns∙ Recommended to initiate treatment if ALT persistently >2× ULN
∙ IFNs given parenterally and associated with temporarily disrupted growth43Data compiled from refs. 10–12.
↵* Defined as child B or C cirrhosis, or Child–Turcotte–Pugh score ≥7.
ADV, adefovir; ALT, alanine aminotransferase; ETV, entecavir; HAART, highly active antiretroviral therapy; HBc, hepatitis B core antigen; HBIg, hepatitis B immunoglobulin; HBsAg, hepatitis B s antigen; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; HDV, hepatitis D virus; HIV, human immunodeficiency virus; IFN, interferon; LdT, telbivudine; LT, liver transplant; LVD, lamivudine; NUC, nucleo(s)tide analog; Peg-IFN, pegylated interferon; TDF, tenofovir; ULN, upper limit of normal.
Agent (Trade Name) Route Class Dosage Duration Resistance Side Effects Adults Children Interferons Interferon α-2b (Intron A) Subcutaneous — 5 × 106 IU daily or 10 × 106 IU 3 times weekly 3 × 106 IU/m2, 3 times weekly, up to a maximum of 10 × 106 IU weekly* HBeAg-positive: 16−24 weeks
HBeAg-negative: 48 weeks— Influenza-like symptoms, fatigue, headache, malaise, emotional lability (anxiety, irritability) Pegylated-interferon α-2a (Pegasys)† Subcutaneous — 180 μg weekly Not indicated in patients <18 years old 48 weeks — Nucleo(s)tide analogs ETV (Baraclude)† Oral NUC 0.5 mg daily in NUC-naïve patients‡
1.0 mg daily in LVD-experienced patients‡ (≥16 years old)Indicated for patients aged ≥2 years and weighing ≥10 kg
Patients ≤30 kg: weight-based dosing of oral solution
LVD-naïve: 3–9 mL daily
LVD-experienced: 6–18 mL daily
Patients >30 kg
LVD-naïve: 10 mL (0.5 mg) solution or one 0.5-mg tablet daily
LVD-experienced: 20 mL (1 mg) solution or one 1-mg tablet daily≥1 year HBeAg-positive: until HBeAg seroconversion* with maintained undetectable HBV DNA (plus ≥6–12 months' consolidation therapy)
HBeAg-negative: until maintained undetectable HBV DNA (plus ≥6–12 months' consolidation therapy)1% at year 5 Negligible TDF (Viread)† Oral NUC 300 mg daily‡ (patients ≥12 years) Not indicated for patients <12 years old None up to year 5 Potential nephrotoxicity LdT (Tyzeka; Sebivo) Oral NUC 600 mg daily‡ (patients ≥16 years) Not indicated for patients <16 years old 17% at year 2 Negligible ADV (Hepsera) Oral NUC 10 mg daily‡ (patients ≥12 years) Not indicated for patients <12 years old 29% at year 5 Potential nephrotoxicity LVD (Epivir, Zeffix) Oral NUC 100 mg daily‡ Patients aged 2–17 years: weight-based dosing, oral solution or tablets; 3 mg/kg daily (maximum 100 mg daily)* 24% at year 1
70% at year 5Negligible Data compiled from Lok and McMahon,10 European Association for the Study of the Liver clinical practice guidelines,12 US prescribing information for Baraclude (Bristol-Myers Squibb, 2014); Viread (Gilead Biosciences, 2013); Tyzeka (Novartis, 2013); Hepsera (Gilead Biosciences, 2012); Epivir (ViiV Healthcare, 2013); Pegasys (Genentech/Roche, 2014); and Intron A (Merck, 2011).
↵* Use in pediatric patients approved in the United States but not in the European Union. Hepatitis B e antigen (HBeAg) loss and anti-HBe-positivity on 2 occasions 1–3 months apart.
↵† Recommended first-line agents.
↵‡ Dose adjustment is required in patients with impaired renal function (creatinine clearance <50 mL/min).
ADV, adefovir; ETV, entecavir; HBV, hepatitis B virus; LdT, telbivudine; LVD, lamivudine; NUC, nucleo(s)tide analog; TDF, tenofovir.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Markers of HBV Infection and CHB Disease Progression
- HBV Screening
- Overview Management of CHB
- Special Considerations and Unresolved Issues in CHB Management
- Treatment Duration and Stopping Rules
- Role of Noninvasive Assessment of Liver Disease
- HCC Screening and the Role of HCC Risk Scores
- Directions for Future Research
- New Treatments for CHB
- Acknowledgments
- Notes
- References
- Figures & Data
- References
- Info & Metrics