
Article Figures & Data
Figures
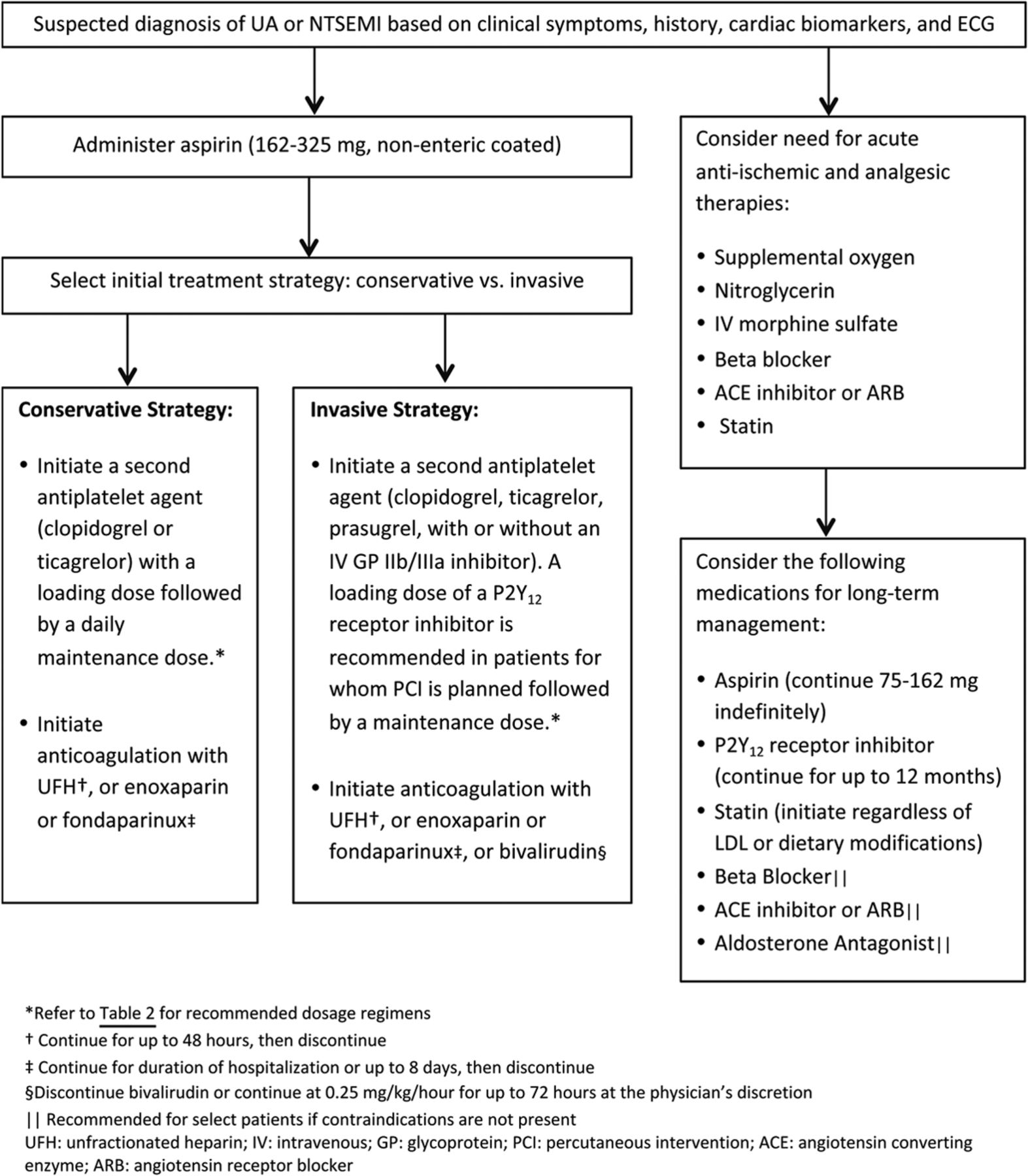
- Figure 1.
Pharmacologic management of patients with Unstable Angina (UA)/Non-ST Elevated Myocardial Infarction (NSTEMI).2,11 ECG, electrocardiogram.
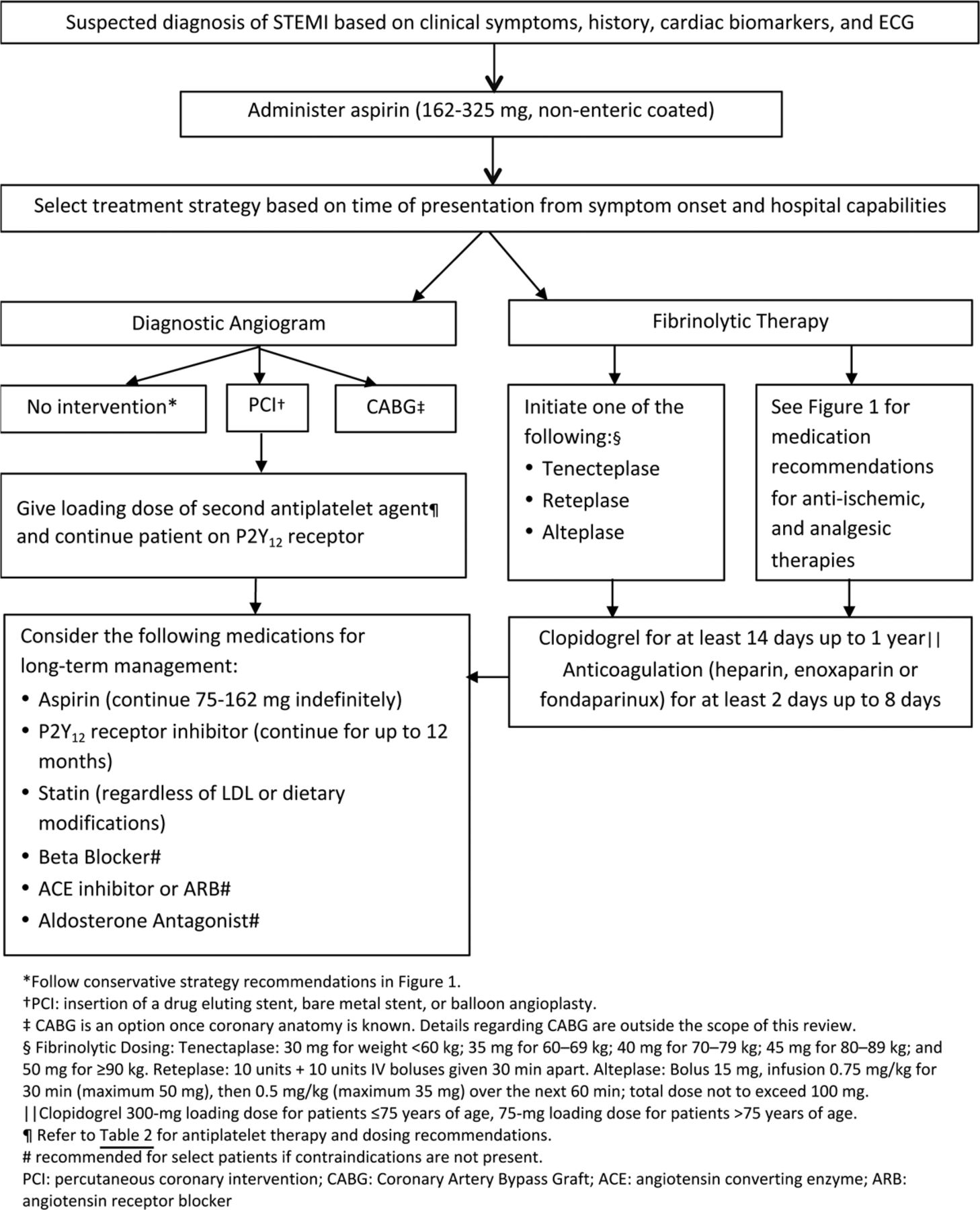
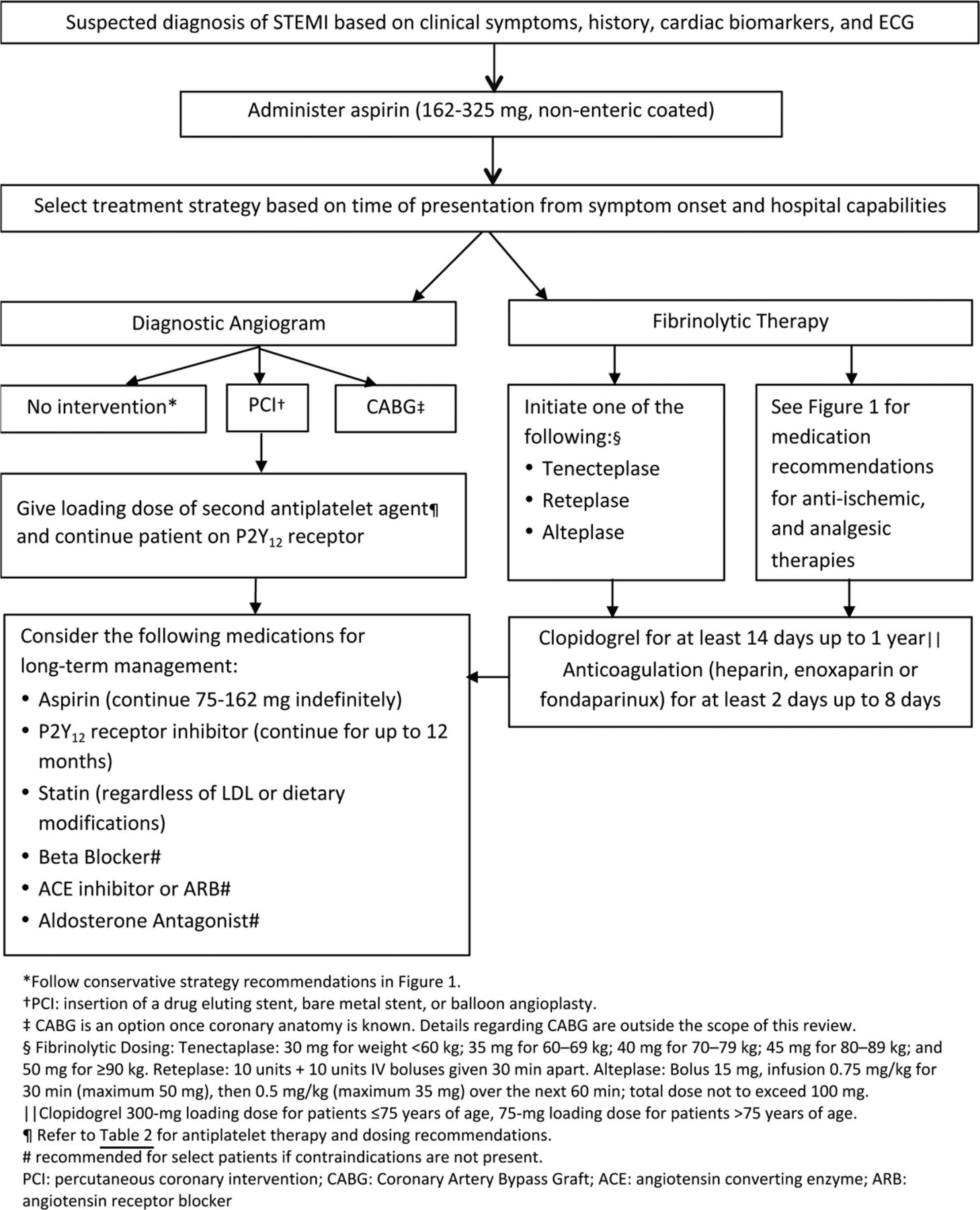
- Figure 2.
Pharmacologic management of patients with ST-elevated myocardial infarction (STEMI).3 ECG, electrocardiogram.

Tables
- Table 1. The Thrombosis in Myocardial Infarction (TIMI) Risk Score for Unstable Angina (UA)/Non-ST Elevated Myocardial Infarction (NSTEMI)2
Baseline Characteristics (1 point for each of the following): TIMI Risk Score (points) Rate of Composite Endpoint (%)‡ Age ≥65 years; At least 3 risk factors for CAD*; Prior coronary stenosis ≥50%; ST segment deviation; At least 2 anginal events in last 24 hours; Use of aspirin in last 7 days; Elevated serum cardiac biomarkers† 0–1 4.7 2 8.3 3 13.2 4 19.9 5 26.2 6–7 40.9 ↵* Risk factors include family history of CAD, hypertension, hypercholesterolemia, diabetes, or being a current smoker.
↵† CKMB fraction and/or cardiac-specific troponin level.
↵‡ All-cause mortality, new or recurrent MI, or severe recurrent ischemia requiring urgent revascularization through 14 days after randomization.
CAD, coronary artery disease; MI, myocardial infarction; CKMB, MB fraction of creatine kinase.
Clopidogrel (Plavix)14 Prasugrel (Effient)15 Ticagrelor (Brilinta)16 Dosing Loading dose for PCI 600 mg 60 mg 180 mg Loading dose for medical management 300 mg 180 mg Maintenance dose 75 mg once daily 10 mg once daily (Consider 5 mg once daily if patient is <60 kg) 90 mg twice daily Onset of action 6 hours with 300 mg dose 30 minutes 60 minutes 2 hours with 600 mg dose Perioperative considerations Hold for 5 days prior to surgery Hold for 7 days prior to surgery Hold for 5 days prior to surgery Clinical pearls Genetic polymorphisms of the CYP 2C19 enzyme lead to variable antiplatelet effects Not FDA approved for medical management, only for patients undergoing PCI Should not be used with daily aspirin maintenance doses of >100 mg Currently, the only generic prescription option Contraindicated in patients with prior stroke or TIA May cause dyspnea, bradyarrythmias, and ventricular pauses No net benefit for patients <60 kg and patients ≥75 years of age Undergoes CYP 3A4 metabolism (concern for drug interactions) Only agent shown to have mortality benefit PCI, percutaneous coronary intervention; FDA, U.S. Food and Drug Administration; TIA, transient ischemic attack.
Dabigatran (Pradaxa) Rivaroxaban (Xarelto)* Apixaban (Eliquis) Clinical trial RE-DEEM (phase II)28 ATLAS-ACS-2-TIMI-51 (phase III) 29 APPRAISE-2 (phase III)32 Patient population 1861 patients presenting with STEMI or NSTEMI 7817 patients presenting with STEMI 7392 patients with recent ACS and ≥2 additional risk factors for recurrent ischemic events Primary outcome Composite of major or clinically relevant minor bleeding Composite of CV death, MI, or stroke Efficacy: a composite of CV death, MI, or stroke Safety: major TIMI bleeding Results There was a dose-dependent increase in bleeding with dabigatran compared with placebo: HR, 1.77 (95% CI, 0.70–4.50) for 50 mg; HR, 2.17 (95% CI, 0.88–5.31) for 75 mg; HR, 3.92 (95% CI, 1.72–8.95) for 110 mg; and HR, 4.27 (95% CI, 1.86–9.81) for 150 mg (all given twice daily) Rivaroxaban reduced the primary efficacy endpoint of CV death, MI, or stroke compared with placebo (8.4 vs 10.6%; HR, 0.81; 95% CI, 0.67–0.97; P = .019) There was no significant reduction in the occurrence of ischemic events when comparing apixaban to placebo (7.5 vs 7.9%; HR, 0.95; 95% CI, 0.80–1.11; P = .51) Rivaroxaban increased non-CABG TIMI major bleeding (2.2 vs 0.6%; P = .001) and ICH (0.6 vs 0.1%; P = .015) without a significant increase in fatal bleeding (0.2 vs 0.1%, P = .51) Apixaban demonstrated an increase in major TIMI bleeding compared with placebo (1.3 vs 0.5%; HR, 2.59; 95% CI, 1.50–4.46; P = .001) Conclusions Dabigatran was associated with a dose-dependent increase in bleeding events in this patient population when compared to placebo Rivaroxaban reduced CV events in this patient population when compared with placebo, albeit at an increased risk of bleeding Apixaban increased the frequency of major bleeds without a significant reduction in ischemic events compared with placebo ↵* The FDA has denied the proposed expanded indication for rivaroxaban as a treatment for patients with ACS to reduce the risk of MI, stroke, death, or stent thrombosis.30 Rivaroxaban 2.5 mg twice daily is approved in Europe for secondary prevention of ACS in combination with standard antiplatelet therapy.31
APPRAISE-2, Apixaban for Prevention of Acute Ischemic Events 2; ATLAS-ACS-2-TIMI-51, Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome—Thrombolysis In Myocardial Infarction-51; CABG, coronary artery bypass grafting; CV, cardiovascular; HR, hazard ratio; ICH, intracranial hemorrhage; MI, myocardial infarction; RE-DEEM, The Randomized Dabigatran Etexilate Dose Finding Study in Patient with Acute Coronary Syndromes Post Index Event with Additional Risk Factors for Cardiovascular Complications Also Receiving Aspirin and Clopidogrel. STEMI, ST-elevated myocardial infarction; NSTEMI, non-ST elevated myocardial infarction; TIMI, thrombosis in myocardial infarction; CI, confidence interval.




{kind=link}
{kind=link}