
Abstract
Background: Cardiovascular risk factors (CVRFs) in reproductive-aged women can lead to pregnancy complications and fetal anomalies.
Methods: We performed a cross-sectional analysis using data from the National Ambulatory Medical Care Survey, 2009–2010. The study sample included visits by reproductive-aged women with CVRFs diabetes, hypertension, hyperlipidemia, obesity, or tobacco use. The comparison group was visits by reproductive-aged women with no chronic disease. Family planning action was defined as counseling, medication, or procedure.
Results: Among an estimated 223,407,070 ambulatory visits, 30.8% were associated with at least 1 CVRF, and 17.2% had at least 1 family planning action. There was no increased frequency of family planning for visits by women with CVRFs compared with those with no chronic disease (17.4% vs 17.1%, respectively). In the multivariable model, the odds ratio (OR) of a woman with a CVRF receiving family planning was 1.2 (95% confidence interval [CI], 0.9–1.5). Visits for preventive care (OR, 2.3; 95% CI, 1.8–3.1), as well as gynecologic and sexual health care (OR, 2.6; 95% CI, 1.9–3.7), were significantly associated with increased odds of family planning.
Conclusion: There are low rates of family planning during visits by reproductive-aged women overall, with no significant difference for visits by women with CVRFs. Comprehensive preventive visits in primary care may especially benefit women of reproductive age with CVRFs, reducing the risk of poor pregnancy outcomes.
For women of reproductive age, cardiovascular risk factors (CVRFs) carry an immediate risk of complicated pregnancies and poor fetal outcomes. Health care providers and policymakers often frame CVRFs in terms of their long-term sequelae—heart disease and stroke—which are the leading causes of death in the United States.1 Women with untreated risk factors such as obesity, diabetes, hypertension, hyperlipidemia, and tobacco use, however, may have associated pregnancy complications such as preeclampsia, preterm birth, and miscarriage.2⇓–4 Moreover, approximately 6% of pregnancies are potentially exposed to teratogenic medications,5 and women with diseases such as diabetes and hyperlipidemia are more likely to be prescribed teratogens such as angiotensin-converting enzyme-inhibitors or statins.6,7 As the prevalence of CVRFs and the use of such medications in younger patients increases,8⇓–10 the provision of preconception counseling, including family planning, becomes increasingly important to promote healthy pregnancies in these patients.
Despite the importance of careful timing to optimize the pregnancies of women with CVRFs,11 previous research suggests low rates of family planning for women with specific CVRFs. In cross-sectional and cohort studies, women with diabetes are less likely to receive contraceptive counseling compared with nondiabetic women of reproductive age.12,13 Overweight or obese women are more likely to use sterilization methods rather than reversible forms of contraception;14 although sterilization is highly effective, the tendency to use this method among overweight or obese women may reflect inadequate counseling about alternative efficacious family planning therapies or provider concerns about the decreased efficacy of hormonal contraceptives.15,16
Low rates of family planning for women with CVRFs may not be unique to this clinical subgroup; almost half of all pregnancies in the United States are unintended, and family planning counseling is estimated to occur during only about 11.5% of office visits for women of reproductive age.12,17
Although there are guidelines for the safe and effective use of contraception in women with specific medical conditions,18 less is known about current rates of family planning provision to women with these risk factors.19 The purpose of this study is to describe the frequency of provider-reported family planning actions during visits with reproductive-aged women diagnosed with CVRFs compared with women with no chronic diseases. In addition, we aim to explore which patient, visit, and practice factors may mediate the association of a patient's health status and receipt of family planning. There is limited research on the content of visits of women with CVRFs—whether these women receive more family planning in recognition of their increased risk for pregnancy complications or if their visits are dominated by chronic disease management—to make an a priori hypothesis about the direction of the association. Thus we hypothesize that the frequency of provider-reported family planning actions is simply different for women diagnosed with CVRFs, with the aim of assessing the direction of association.
Methods
Data Source
We used data from the National Ambulatory Medical Care Survey (NAMCS) for the combined years of 2009 to 2010 to examine the relationship between CVRFs and family planning. NAMCS is an annual survey conducted by the National Center for Health Statistics (NCHS) within the Centers for Disease Control and Prevention.20 Participating physicians must not be employed by the federal government and must provide care in an office-based setting.21
NAMCS uses a multistage probability design,22 consisting of geographic entities of primary sampling units, a probability sample of practicing physicians selected from the master files of the American Medical Association and the American Osteopathic Association, and a probability sample of patient visits from sample practices. Survey forms are intended to be completed by physicians and clinic personnel, and physicians receive training by survey field members before participation. Participating physicians are assigned 1 of the 52 weeks in the given survey year, and a systematic random sample of visits from the assigned week is then selected.23 Each physician's sampling interval is designed to obtain about 30 patient records from each reporting week; thus large practices may have as few as 20% of visits sampled, whereas small practices may have 100% of visits sampled.24 For the 2010 NAMCS sample, the unweighted response rates was 58.3%.24 Analysis is based on the sampling unit of the physician–patient visit. The Boston University Medical Center Institutional Review Board reviewed and approved this study.
Inclusion and Exclusion Criteria
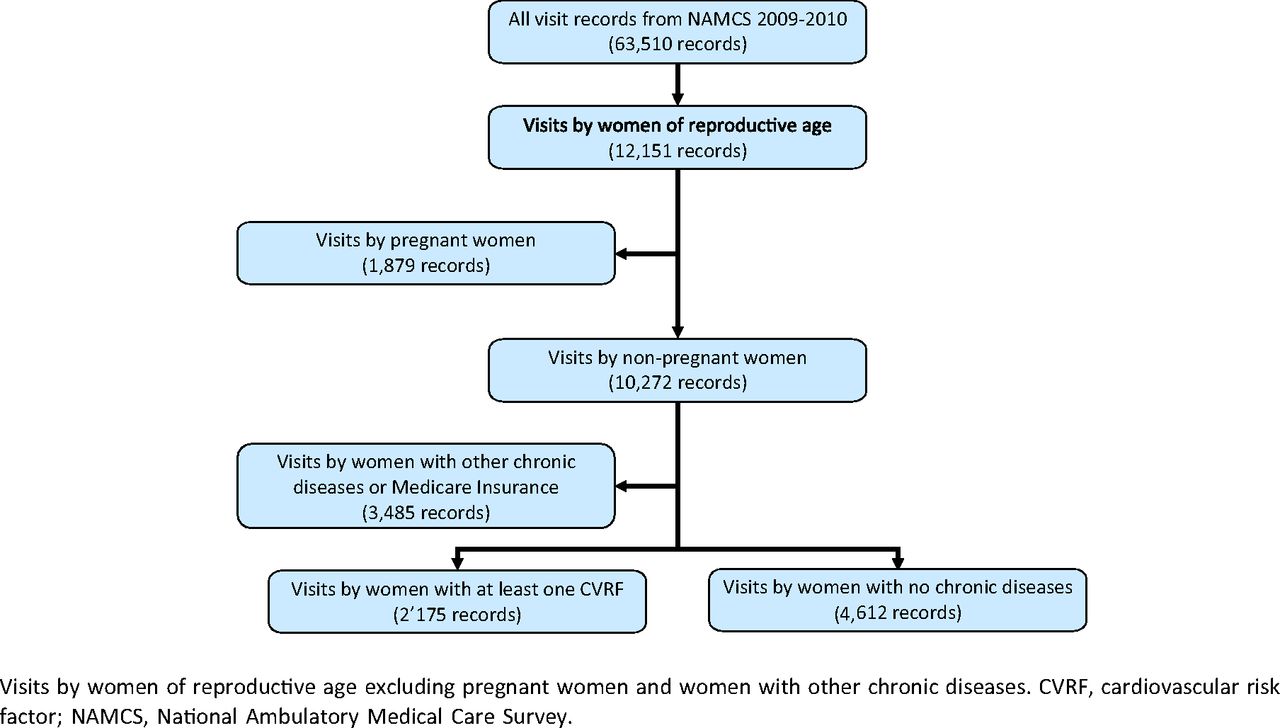
Our sample included visits by nonpregnant female patients between the ages of 14 and 45 with CVRFs or no other chronic diseases (Figure 1). Pregnant women were excluded using the NAMCS Reason for Visit codes and International Classification of Diseases, Ninth Revision (ICD-9), diagnosis codes for pregnancy and its complications (63.0 to 67.6 and V22-V24). Women with chronic conditions other than the CVRFs of interest, including cancer, ischemic heart disease, cerebrovascular disease, congestive heart failure, asthma, chronic obstructive lung disease, chronic renal failure, depression and other mental health diagnoses, chronic infections such as human immunodeficiency virus, arthritis, and osteoporosis, were also excluded. Reproductive-aged women with a higher burden of illness compared with the general population may have a different frequency of family planning than women with no chronic disease. Visits with these women were excluded from the analysis sample to provide a refined comparison to the exposure group. In addition, visits in which Medicare was identified as the insurance type were excluded, with the reasoning that reproductive-aged women who qualify for Medicare have comorbidities that would also affect the frequency of family planning actions.

Study sample.
Exposure/Independent Variable
Our CVRFs of interest included diabetes mellitus, hypertension, hyperlipidemia, obesity, and tobacco use. We captured these conditions with corresponding NAMCS Reason for Visit codes and ICD-9 diagnosis codes (250, 401, 272, 278, 3051-), calculated body mass index ≥30 kg/m2, indicated current tobacco use status under “Patient Information” and chronic disease status under “Provider's Diagnosis For This Visit” on the patient record form. The independent variable was dichotomized as “visit with any cardiovascular risk factor” or “visit with no chronic disease.”
Outcome/Dependent Variable
Family planning was defined by counseling and/or treatment. We identified family planning by 5 possible criteria: NAMCS Reason for Visit Code; ICD-9 diagnosis code (V25, V26, V45); ICD-9 procedure codes for intrauterine devices, subdermal implants, and sterilization procedures (66.2 to 66.3, 669.7); counseling for family planning or contraception indicated under “Health Education”; and contraceptive medications. Contraceptive medications could be newly prescribed or continued medications and included oral contraceptive pills, emergency contraception, transdermal patches, vaginal rings, and injectable contraceptives. Existing intrauterine systems are not part of the NAMCS drug list. A visit was considered to include “any family planning” if at least one of the above criteria was met.
Additional Independent Variables/Covariates
All covariates were determined a priori based on a review of the literature and clinical judgment. Patient-level covariates examined were age, race/ethnicity, median household income associated with the patient's ZIP code, and insurance. We categorized age as adolescent (14 to 17 years old), adult (18 to 34 years old), and advanced maternal age (35 to 45 years old). For insurance type, private insurance, Medicaid, and self-pay were retained; categories of “no charge,” “worker's compensation,” and “other” were collapsed to the category of “other.”
Provider-level covariates included continuity measures (ie, indication of a visit with the patient's primary care physician (PCP) or with a provider within the same practice) and provider specialty. Specialty categories defined by NAMCS were further collapsed into primary care specialties (general and family practice, internal medicine, and pediatrics), obstetrics/gynecology, and other (general surgery and primarily subspecialty care). The two available practice-level covariates were region associated with the practice ZIP code (northeast, midwest, south, and west) and metropolitan statistical area.
Visit-level covariates were the major reason for visit (preventive or nonpreventive) and concurrent gynecologic or sexual health care. Family planning actions may be more likely to occur at a preventive care visit, whereas patients and providers may prioritize acute and chronic disease needs at other types of visits. We hypothesized that at visits in which patients receive gynecologic or sexual health care, either the provider or the patient may be more inclined to raise family planning concerns. Visits for gynecologic care or sexual health care were identified by NAMCS Reason for Visit and ICD-9 codes for pelvic inflammatory disease, cervicitis, vaginitis, and other disorders of the female reproductive tract, as well as indication of a pelvic examination, Papanicolaou test, or testing for human papillomavirus, chlamydia, or human immunodeficiency virus.
Data Analysis
Using SAS software version 9.3 (SAS, Inc., Cary, NC), we developed bivariate and multivariable models that used weights and design variables provided by the NCHS to account for the multistage probability sampling used to collect the NAMCS data. These analyses took into account the design of the larger NAMCS survey by using specialized commands in SAS to analyze the subsets of data from complex sample surveys.
Descriptive statistics were computed on the primary independent variable of visits with any CVRFs and the dependent variable of visits with any family planning. The frequency and weighted percentages of individual CVRFs in the sample were calculated.
Bivariate analyses were performed for primary outcome and exposure using the Wald χ2 test of significance. Subsequently, each covariate was included individually in a logistic regression model of primary outcome and exposure; all but one covariate (visit within the same practice as the patient's PCP) resulted in a >10% change in the parameter estimate for the primary independent variable of visits with any CVRF. We ultimately included this variable in the final logistic regression model since continuity of care was conceptually important. Three variables derived from the patient's ZIP code exhibited potential collinearity: percentage of population with a bachelor's degree or higher, percentage living in poverty, and median household income. The last of these variables was chosen as the indicator of socioeconomic status for the regression model because it limited the standard error (SE) of the parameter estimate to the greatest degree. In the final logistic regression we included the following covariates: age category, race/ethnicity, median household income based on the patient's ZIP code, insurance type, visit with patient's PCP, visit with patient's established practice, specialty category, metropolitan statistical area status and region of the practice, major reason for visit (preventive or nonpreventive), and receipt of any gynecologic or sexual transmitted disease care provided during visit. The Wald χ2 test of significance was performed for each covariate and the overall regression model. Covariates with statistically significant parameter coefficients (ie, age category, major reason for visit, provider specialty category, and receipt of gynecologic or sexual health care) were tested in the multivariable regression model using interaction terms with the primary exposure variable of visit with any CVRF.
In accordance with the standard of the NCHS, we considered estimates to be reliable if they were based on at least 30 records and had a relative SE of ≤30% for univariate point estimates.25 In our analysis sample, relative SEs fell within this range, with the exception of metropolitan statistical area status (30.5%) and other specialty (32.6%). We report the number of patient records for each variable, as well as the percentage of visits computed using sampling weights.20 Findings statistically significant at P < .05 are noted.
Results
We identified 6,787 visit records of nonpregnant women of childbearing age in 2009 to 2010, representing 223,407,070 ambulatory visits. The majority of visits were by adults between the ages of 18 and 34 years old (50.7%) and were paid for with private insurance (73.0%) (Table 1). Approximately 43% of visits were within primary care specialties and 23.1% of visits were categorized as preventive. Nearly one quarter of visits included delivery of gynecologic or sexual health care.
Visits with any CVRF (30.8%) were typically by older women, with a mean age of 32.3 years (SE, 0.4 years) compared with visits by women without chronic diseases (28.8 years; SE, 0.3 years). Visits with any CVRF were further characterized by lower use of private insurance compared with Medicaid and self-pay (Table 1). The mean number of yearly visits by patients with any CVRF was 2.8 compared with 2.5 for patients without chronic diseases, a difference that was statistically significant (P < .001). Records could have more than 1 CVRF recorded; of all records, 69.2% (SE, 0.8%) had no CVRF, 22.7% (SE, 0.7%) contained 1 risk factor, and 5.5% (SE, 0.3%) had 2 risk factors. The most common risk factors were obesity and tobacco use.
Approximately 17.2% of visits had at least 1 family planning action. Visits with family planning had higher frequencies of adult patients, private insurance use, and obstetrician/gynecologist specialty care. Over 50% of visits classified as preventive or including gynecologic or sexual health care included at least 1 family planning action. Bivariate analysis of visits with family planning and visits with CVRFs showed no difference between the frequency of family planning for visits with CVRFs and those with no identified chronic disease (p = .81) (Table 2).
In the multivariable logistic regression, the odds ratio (OR) of receiving family planning with the presence of any CVRF was 1.2 (95% confidence interval [CI], 0.9–1.6; Table 3). Visits by women of advanced maternal age were associated with lower odds of family planning actions (OR, 0.4; 95% CI, 0.3–0.5), as were visits with primary care (OR, 0.5; 95% CI, 0.3–0.9) or other specialties (OR, 0.3; 95% CI, 0.2–0.5). Conversely, preventive visits and visits with gynecologic or sexual health care were significantly associated with increased odds of family planning actions during an ambulatory visit with a female patient of reproductive age (OR, 2.3; 95% CI, 1.8–3.1 and OR, 2.6; 95% CI, 1.9–3.7, respectively). The following variables were added to the multivariable regression models as interaction terms with any CVRF: age category, specialty, preventive care, and gynecologic or sexual health care; none were statistically significant.
Discussion
Despite the substantial body of scientific evidence demonstrating that women with CVRFs are at higher risk of pregnancy and perinatal complications, family planning within this vulnerable population remains low. Using a large national database, we found only 17.2% of visits by reproductive-aged women included any family planning and that the odds of family planning during visits by women with CVRFs were not significantly different from visits with no chronic diseases. For the population at large, management of CVRFs is essential to prevent the long-term harm of cardiovascular disease. In contrast, for a woman of reproductive age, these risk factors endanger a pregnancy and the health of a fetus in the immediate future.
Our results are consistent with a study using NAMCS that found that contraceptive counseling was documented for <20% of visits in which potentially teratogenic medications were prescribed to reproductive-aged women.26 Similarly, in a recent study using survey data from the Maryland Pregnancy Risk Assessment Monitoring Systems, postpartum women with hypertension, diabetes, and heart disease were no more likely to report receiving antepartum contraceptive counseling than women without these comorbidities.27
Our findings are not surprising in the context of a fragmented health care delivery system. Women of reproductive age commonly receive preventive care, including family planning services and cervical cancer screening, from specialty providers such as obstetrician/gynecologists or specialty clinics such as freestanding family planning clinics.28 While these services fill gaps in access to women's health care, they limit coordination of care, which is particularly important for women with CVRFs.29
The importance of preconception care in patients with medical comorbidities has been recognized by institutional and professional bodies including the Centers for Disease Control and Prevention,30 the Institute of Medicine,31 and the American College of Obstetricians and Gynecologists,11 yet implementing it remains elusive. The Patient Protection and Affordable Care Act (PPACA) offers opportunities to realize care integration for reproductive-aged women by delivering health care through a patient-centered medical home (PCMH). This restructured health care delivery model promotes preventive services, including preconception care and chronic disease management, within an integrated health care team. In our study the odds of any family planning action were 2.3 times higher for preventive visits and 2.6 times higher for visits where gynecologic or sexual health care was provided. The increased likelihood of family planning in the setting of comprehensive, preventive health visits suggests that the PCMH model of health care delivery may promote essential integrated preconception care for reproductive-aged women. While we observed a lower odds of family planning action for visits in primary care specialties compared with obstetrics and gynecology, further adoption of the PCMH model and reimbursement of preventive services may shift more provision of family planning into primary care.
Furthermore, the PPACA emphasizes the use of information technology and quality measures,32 which can facilitate coordinated care for reproductive-aged women with CVRFs. For example, decision support tools for electronic prescribing of medications can alert a provider that a patient is of childbearing age and caution against the use of teratogenic medications, unless pregnancy is not a possibility.33 Such alerts show promise in promoting among providers and patients the review of pregnancy intention and increased contraception use among women taking potentially harmful medications.33,34 In a cluster randomized controlled trial, screening reproductive-aged women with a “contraceptive vital sign” increased documentation of contraception in women not desiring pregnancy, though further work needs to be done to increase the provision of family planning services in the primary care setting.35 Current quality metrics such as Healthcare Effectiveness Data and Information Set (HEDIS) measures do not feature preconception care as a standard of care and have a dearth of standards related to ensuring healthy pregnancy outcomes.36 Preconception quality measures standardized through the electronic medical record would raise expectations about the provision of these services.
Our study has a number of strengths, including use of a large national data set designed to represent the provision of outpatient care across the United States. Prior studies using NAMCS data demonstrated low rates of family planning counseling for women with diabetes.12 Our analyses expand the population of interest to women with any of several CVRFs, some of which, such as obesity, are far more common than diabetes and less recognized as risk factors for pregnancy complications. We used multiple methods to identify both exposure and outcome variables, an inclusive strategy that increases the sensitivity of our analysis. We used variables at the patient, provider, and system level to examine multiple possible factors influencing rates of family planning actions and created a novel composite variable for gynecologic and sexual health care as a facilitating process variable.
Our findings must be viewed within the context of certain limitations. There is a risk of misclassification bias if women with CVRFs were not appropriately identified; however, in our study we used multiple methods to select women with at least 1 CVRF. Patients with chronic conditions such as hyperlipidemia and diabetes may be expected to have more visits with their provider than women with no chronic conditions. We compared the number of visits for women with CVRFs and women with no chronic diseases and did not find a clinically meaningful difference in the frequency of visits. Therefore we did adjust the model to account for differences in the baseline number of visits according to disease state.
Counseling services have been shown to be underreported in the NAMCS; in an observational study designed to validate NAMCS methods, family planning counseling on the NAMCS form was highly specific when compared with direct observation (specificity, 0.99) yet was quite insensitive (sensitivity, 0.29), indicating that physicians substantially underreported how often family planning counseling was delivered.37 Although underreporting is unlikely to differ according to the presence or absence of CVRFs, the overall low rates of reported counseling may hinder the ability to detect meaningful differences between groups. The rates of family planning documented in the NAMCS may be interpreted as the “lowest estimated limit” of counseling that in fact occurs.
We recognize that there are several important family planning factors that the NAMCS survey cannot capture, such as a patient's desire to conceive at the time of the visit, her sexual orientation, or history of sterilization. The lower odds of family planning counseling observed among women of advanced maternal age may indeed reflect known sterilization of the patient or her partner. Although we identified most types of contraception, certain contraceptive methods (barrier contraception such as condoms and diaphragms and preexisting intrauterine devices) are not recorded. There may be differences in the frequency of use of these other forms of contraception according to the presence of chronic disease.38,39
Although the NAMCS is a national survey with complex sampling designed to provide reliable information about the delivery of health care in outpatient practices across the country, the quality of the data are limited by the survey response rate and whether the selected ≥30 records obtained from each practice are truly representative of the patient population. Nevertheless, the systematic and random sampling strategy used by the NAMCS would be expected to reduce any nondifferential bias based on the presence of CVRFs.
The NAMCS provides information at the visit level, rather than the individual patient level; thus we can only draw conclusions about the frequency of family planning occurring at single visits. This raises the question of how often family planning should occur; our data cannot capture whether a patient received counseling at an earlier visit or received counseling at least once in the past 12 months. While further research is needed to determine the optimal frequency of family planning, a patient's intentions to have children may change from one visit to the next,40 and the low frequency of family planning actions in our study demonstrates that more attention needs to be dedicated to addressing the preconception needs of reproductive-aged women. While regularly assessing pregnancy intention may seem daunting to the busy PCP, pregnancy intention may represent a “teachable moment” for chronic disease self-management—an opportunity to capitalize on the patient's motivation for a healthy child and educate her on adopting healthy behaviors.41 At a minimum, yearly family planning counseling during a preventive visit would move toward the goal of a developing a reproductive life plan,42 with an opportunity to engage in cardiovascular disease prevention.
Conclusion
There is a low frequency of documented family planning during visits with reproductive-aged women, with no significant increase among women with CVRFs that are associated with pregnancy complications. Proposals under the PPACA, including the PCMH, information technology, and quality measures, may promote the integration of preconception care into primary care, especially benefitting reproductive-aged women with CVRFs.
Notes
This article was externally peer reviewed.
Funding: This work was supported by the American Cancer Society Physician in Training Award in Cancer Prevention (PTAPM-97-185-16), VA-OAA Advanced Fellowship Program in Health Issues of Women Veterans.
Conflict of interest: none declared.
- Received for publication January 16, 2014.
- Revision received June 13, 2014.
- Accepted for publication June 23, 2014.




{kind=link}