
Abstract
Purpose: The purpose of this study was to investigate the effects of a cognitive behavioral therapy–oriented anger management and stress control program on smokers' quit rates.
Methods: Of 2348 smokers, 350 were randomly allocated into study and control groups (n = 175 each). An individualized therapy cessation technique was selected for each participant (combination of behavioral counseling, nicotine replacement therapy, and/or pharmacotherapy). The participants in the control group attended a standard quit program, whereas the study group also received an additional 5-session (90 minutes each) cognitive behavioral therapy–oriented program aimed at improving their anger and stress coping skills. At the beginning of the study, both groups were asked to complete the Trait Anger Scale (TAS) of the State and Trait Anger Scale and the Self-Confident (SCS) and Hopeless (HS) subscales of the Stress Coping Styles Inventory; pretest smoking status of both groups and their coping skills were compared with each other as soon as the program ended (post-test results) and after 3 and 6 months (first and second follow-up tests).
Results: Although there was no difference between pretest scores on the TAS (P = .234), SCS (P = .130), and HS (P = .148) subscales, post-test results indicate that the study groups' TAS and HS scores decreased and SCS scores increased (P < .001), whereas there was no change in the control group (P > .05). The study group had a better quit level after 6 months compared with the control group (44% vs 27.4%; P < .001). The anger management and stress control program was found to have a significant effect on cessation (odds ratio, 2.09; 95% confidence interval, 1.14–3.85).
Conclusion: The anger and stress coping skills program may increase the success of quitting smoking.
The importance and effectiveness of primary care interventions in preventing smoking are well known.1 As part of health promotion activities, one priority has been to increase the success rates of smoking cessation.2,3 However, up to 75% of smokers start to smoke again within 6 months, even though they receive behavioral support, nicotine replacement therapy (NRT), or drugs (bupropion or varenicline).4 Many studies have been performed to understand the interacting physiological and psychological factors involved in relapse.5 Some sociodemographic risk factors (sex, education level, marital status, living alone, and income) have been identified. Nicotine—a very potent psychological and neurological stimulant that influences behaviors, emotions, and mood—is implicated as the main factor responsible for initiation, maintenance, and relapse in terms of smoking.6⇓⇓–9 In recent years a strong relation between anger, stress, and smoking has been noticed.10,11 Smokers report that they smoke more when they are stressed, angry, anxious, or sad and that they expect that smoking will alleviate these negative moods.12 There is strong evidence that nicotine reduces emotions of stress and anger because deprivation causes increases in feelings of anger and stress, despite whether they are amplified by other distressing withdrawal symptoms.13 Several different interacting models, such as a direct effects mechanism (opioid and reward pathway models) and moderator (restoration of homeostasis model) and mediator effects [situation by trait adaptive response (STAR) model] have been investigated to explain the relation between nicotine, stress, and anger.14⇓⇓⇓–18
Despite all the evidence concerning the relationship between smoking, anger, and stress, the effect of this relationship on relapse is not well documented. Some recent studies noted that individuals with high levels of trait anger and stress are more prone to start smoking again.19,20 More recent studies revealed that smokers with insufficient anger management and stress control skills are more vulnerable to relapse.21,22 These data reflect the importance of effective anger management and stress control skills in dealing with nicotine abstinence and successful maintenance of quitting smoking. Support for anger and stress is used in many quit-smoking counseling activities.23 These activities, however, do not address the actual problem. Without improved anger management and stress control skills, smokers who have since quit are at a high risk of relapse in the face of adverse daily life experiences (which may cause high levels of anger and stress) whenever they need the support previously provided by smoking.24 Anger management and stress control skills are regarded as being in the main domains of emotional intelligence and can be upgraded and promoted with proper cognitive behavioral approaches.25 It would, therefore, be a logical assumption that improving these skills results in an increase in smokers' quit rates, which may help them to avoid relapse, not only in the short term but also in the mid-term. To test this hypothesis, we designed a 5-session anger management and stress control program to promote these skills in smokers who are willing and ready to quit. This study investigates the effect of a cognitive behavior—oriented anger management and control program designed to be applied in primary care settings dealing with quit-smoking activities to increase quit rates.
Materials and Methods
Design
The study was designed as a randomized controlled trial between March 2010 and December 2011. It was performed at the Ondokuz Mayıs University Medical Faculty Department of Family Practice Smoking Quittance Clinic, Turkey. Before the study began, a power analysis was conducted to calculate the number of participants within different treatment groups. Based on the literature, we assumed standard deviation of 22, 8 levels, a target power of 0.8, and a maximum difference of 20. Based on that analysis, we calculated a minimum number of 28 participants in each treatment group. To minimize the risk of affecting the study outcomes, we decided to investigate the effects of this program on smokers who had never tried to quit before. Relapsed smokers might have experienced some of the cessation strategies and had a negative attitude toward the methods they had used previously. The other criteria for inclusion in the study were willingness to take part in and attend all sessions, age >18 years, intent to quit smoking within 6 months, smoking >10 cigarettes a day, not taking any psycho-regulatory medication (antidepressants, anxiolytics, or antipsychotics), not having any psychiatric illnesses, not being pregnant or breastfeeding, and applying all the program session content for 6 months.
In our clinic, smokers are placed on a waiting list for the following month after their initial sociodemographic, health, and smoking features are investigated. After we announced that a cognitive behavioral therapy—oriented anger management and stress control program aiming to increase these skills of smokers was to be implemented, we selected smokers who fulfilled the research criteria for the study and control groups from these waiting lists. Each month, a new study group (a total of 12 different study groups) and control group (a total of 12 different control groups) were added to the research; participants were selected from the previous month's waiting list.
To obtain optimal efficiency from cognitive behavioral treatment (enough experiences to be shared, stimuli for discussion, etc.), the number of participants in the groups had to be limited to approximately 20. This would have limited our research to a single study and control group. Therefore we decided to form each month new study (12 in total) and control (12 in total) groups limited to approximately 20 participants selected at random from our clinic's waiting list. The first study and control subgroups were selected from the waiting list of February 2010, and the 12th and last subgroups from the January 2011 list. The total study population consisted of 2348 smokers admitted to our clinic between February 2010 and January 2011. Of these, 350 smokers (175 smokers in each group) were selected for the research. To perform basic randomization in groups, participants who fulfilled the study criteria and were on the previous month's waiting list were divided into 2 different lists by sex in order of application. First, the male and female smokers at the top of both lists were assigned to the study subgroup, the second smokers on both lists to the control subgroup, the third to the study subgroup, the fourth to the control subgroup, and so on, until they were equally divided. The remaining smokers on the waiting list who did not meet the study criteria (n = 1418) or who were not interested in participating in the research (n = 580) were administered our clinic's standard treatment procedure (control group treatment program), consisting of approximately 3 months of treatment and follow-up. An informed consent form was obtained from each participant, and a confidentiality contract was signed by study group members.
At the beginning of the program, each participant in the study and control subgroups was asked to respond to the Fagerstrom Test for Nicotine Dependence (FNDT), the State Trait Anger Inventory, and the Styles of Coping with Stress Inventory (pretests). Pretests were collected from subgroups between March 2010 (first study and control subgroups) and January 2011 (12th study and control subgroups). Our clinic's standard quitting procedure was applied to both subgroups, whereas the 5-week anger management and stress control coping program was applied to the study subgroups alone. Smoking status of participants in both subgroups, together with their skills, were compared and recorded as soon as the program ended, 30 to 35 days from their first visits (post-test results). Post-test results were collected from subgroups between May 2010 (first study and control subgroups) and March 2011 (12th study and control subgroups). The same data were collected the third and sixth months after post-tests were administered to both subgroups (first and second follow-up tests). First follow-up tests were collected between September 2010 (first study and control subgroups) and August 2011 (12th study and control subgroups) and the second follow-up tests between November 2010 and December 2011 (including relapsed participants). At the end of the study, the results from the participants in these subgroups were pooled and evaluated as a single study group and single control group. Although the participants in the study subgroups knew that they were in the anger management and stress control program, the data collectors were blind when applying the tests. Relapsed participants reenlisted in our clinic for a new round of treatment 6 months later.
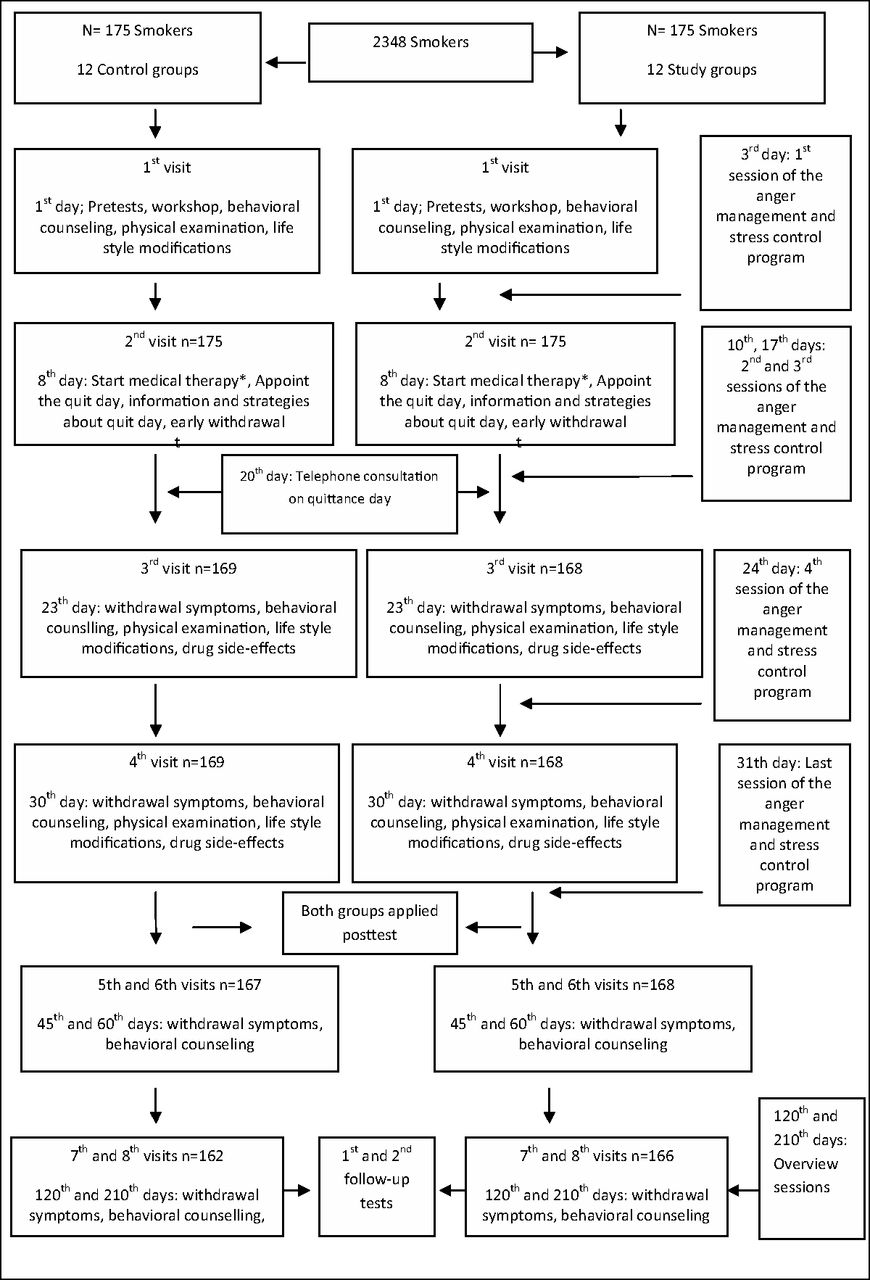
The participants were expected not to smoke for any reason after the contracted quit day. Smoking status of patients was established by self-report and assessment of carbon monoxide with an inhaler. Participants who relapsed on just 1 or 2 occasions were not excluded from the study. Participants with readings of ≤10 ppm carbon monoxide were regarded as smoking free.26 Participants' smoking status was investigated 4 times. The first investigation was performed between the 7th and 10th days after the contracted quit day (post-test). The second investigation was the 30th day after the quit day, the 3rd was at the 90th day (1st follow-up test), and the 4th was at approximately the 180th day (2nd follow-up test). A flowchart of the study procedure administered to all study and control subgroups is shown in Figure 1. The study was performed in all subgroups in this chronological order, with no more than 3 or 4 days' delay because of differences in quitting times and some national holidays.

Flowchart of the study procedure administered to all participants in the study and control groups (a total of 12 groups); a new study and control group were included every month between March 2010 and February 2011.
Both groups received a 40-minute session of the same workshop on their first visit. Participants in the control group received nearly 150 minutes of individualized face-to-face treatment (in approximately 10 visits) for 6 months (control groups' treatment program). Participants in the study group received 630 minutes of group (5 + 2 sessions) and 100 minutes of individualized (10 visits) face-to-face treatment for 6 months (anger management and stress control program). We calculated that approximately 440 work hours (for 175 participants) were needed for the control group and nearly 420 work hours were needed for the study group in 6 months.
Control Group Treatment Program (Clinic's Standard Program)
All subjects took part in several types of smoking cessation activities according to their smoking status, dependency level, and indications.27⇓⇓–30 This program includes a group workshop, face-to-face interventions aimed at maintaining lifestyle changes, NRT, and pharmacotherapy. Patients who apply to the Ondokuz Mayıs University Family Practice Smoking Cessation Clinic are enrolled in an average 3-month smoking cessation program. Approximately 10 interviews (4 in the first month, 3 in the second, and 3 in the third) are conducted during the program. If necessary, one visit per month can be planned. Appointments are made to form groups of 20 patients each.
During the first meeting, a workshop is held at which smoking cessation techniques and nicotine addiction are discussed with the group for approximately 1 hour. At this workshop, members share previous smoking cessation experiences. All group members are encouraged to share their experiences and thoughts concerning how they started smoking, the benefits of quitting, any close friends or relatives who were harmed by smoking, any close friends or relatives who successfully quit smoking, and previous attempts to quit (How long did you quit for? What went wrong? Which method was used?). In the next step, a short, interactive presentation is given to consolidate negative emotions against smoking and reinforce the desire to quit. In this part of the session, strategies for smoking cessation, drug therapies including NRT and behavioral approaches to dealing with addiction, are discussed. To avoid withdrawal symptoms (mostly coping with anger and stress), basic techniques (increase physical activity, change one's environment, the effect of relaxing music, hobbies, and deep breathing, etc.) are discussed for at least 20 minutes. Patients first are asked to perform some lifestyle modifications and change their smoking habits (discussion and handouts). These changes aim to prepare the patient for the quitting day. They include changing the cigarette brand used, not smoking for 90 minutes after waking up, smoking only after meals or with tea or coffee (if these usually accompany smoking), avoiding offering and accepting cigarettes from other people, smoking alone (if being in a group triggers smoking), changing one's usual smoking places (at home, work, etc.), refraining from alcohol intake for 3 months (if smoking accompanies alcohol use), and, finally, increasing the amount of daily physical exercise (half hour, moderate). They are finally asked to find a quit buddy from their workshop group for the future quitting process; then the workshop is concluded.
On the same day, each patient is privately interviewed for a minimum of 20 minutes, and a general physical examination (anthropometric parameters included) is performed. The principles of motivational interviewing are used during this session.31 Each smoker is given an individualized behavioral counseling session lasting 20 minutes. In this first step, the smoker is encouraged to make lifestyle changes, and the next appointment is scheduled, usually for a week to 10 days later. At the second appointment, lifestyle changes are evaluated, the basic techniques for withdrawal symptoms are revised face to face, and a quit day is agreed on (generally 10 to 12 days later). Pharmacological treatment (drugs) begins here. If the patient wishes to use NRT, he or she is recommended to start on the quit day. On the quit day, a telephone call is made to the patient in an attempt to increase motivation. After 2 days of quitting, another interview is conducted if possible. In these interviews, nicotine withdrawal symptoms, strategies to overcome them, side effects or any other problems associated with drugs (if used), and reinforcement of motivation are discussed. Subsequently, similar interviews are conducted every 10 to 15 days.
Treatment Groups
There were 4 different treatment groups. The first group was treated with behavioral counseling (BC; motivational interviewing with lifestyle modification) only, the second group received BC with NRT, the third received BC with bupropion, and the fourth BC with varenicline. Smokers' choice of treatment group was discussed with them based on their smoking history, FNDT scores, and indications and contraindications set out by the Turkish Ministry of Health. NRT is mostly used with smokers with FNDT scores <3, and varenicline or bupropion with smokers with FNDT scores ≥3. All drugs were provided free for 3 months during the study period by the Ministry of Health. Written consent was obtained from all patients before initiating pharmacotherapy. NRT is used in doses of 21 mg, either as gum or patches, for as long as necessary. Bupropion is recommended at 150 mg for the first 3 days of therapy and 300 mg from the fourth day, usually for 3 months. Varenicline is used at 500 mg for the first 3 days, 1000 mg between the fourth and seventh days, and 2000 mg from the eighth day, usually for 3 months.
Anger Management and Stress Control Skills Training Program
The cognitive behavioral therapy—oriented anger management and stress control program was applied to the study group for 5 weeks in 90-minute sessions as soon as the standard cessation program was initiated (2 days after the first interview). We designed a 5-session program (90 minutes each). The program is structured along eclectic, educational, and didactic experimental principals in accordance with time limitations. Many resources were used to design the program, as mentioned elsewhere.32 The program content is presented in Appendix 1. Participants are expected to acquire the following skills: ability to notice clues to anger and stress; ability to recognize physical, emotional, and behavioral responses to sources of stress and anger; ability to learn and use techniques of relaxation and proper breathing for the control of stress in daily life; to gain awareness of anger and stress-related situations, such as uncontrolled behavior, physical assaults, or regrettable behavior; to gain awareness of the damaging effects of stress and anger on relationships, overeating, smoking, or drug use to appease anger and stress together with associated physical and legal problems; ability to recognize anger and stress-related negative automatic thoughts, and core and adjacent beliefs, and the ability to detect and define negative emotions that accompany these as they arise; ability to use various skills and cognitive restructuring to control stress and anger; ability to recognize cognitive diversions; ability to share emotions without aggression; ability to use effective communication, social interaction, time management, use of humor, changes in the environment, and so on; ability to express anger and other negative emotions with “I” language; ability to use effective listening skills and notice inappropriate listening reactions; ability to control stress and anger and to display willingness to maintain communication and create empathy in an attempt to establish understanding at times of conflict. As usual in cognitive behavioral—oriented therapy, 2 additional sessions were held at the third and sixth months aiming to overview the content of the anger management and stress control program and share participants' experiences. Before these sessions, the first and second follow-ups using the Trait Anger Scale (TAS) of the State and Trait Anger Scale and the Self-Confident subscale (SCS) and Hopeless subscale (HS) of the Stress Coping Styles Inventory were applied to the participants in the study group.
Tools
Fagerstrom Test for Nicotine Dependency
The FNDT is a 6-item self-report scale frequently used worldwide to determine levels of nicotine addiction.33 Although the test is actually modified from the Fagerstrom Tolerance Questionnaire, it has better internal consistency and is more easily answered. In terms of the overall logic of this test, it is based on number of cigarettes smoked and length of smoking-free periods. The instrument yields a dependency score between 0 (low) and 10 (high).
State Trait Anger Scale
Developed by Spielberger et al,34 the State Trait Anger Scale has 2 main subscales, the TAS, consisting of 10 self-reported items, and the Anger Expression Scale, which has 3 different subscales of 8 self-reported items (a total of 24 items). We used TAS scores as variables indicating trait anger level for this research. An individual can score between 0 and 40 on the TAS. Higher scores on the TAS indicate that the individual's trait anger level is high. Validity and reliability of the Turkish version of the test was investigated by Ozer.35 Cronbach α values have been calculated as 0.90 for the State Trait Anger Scale and between 0.82 and 0.90 for the subscales.
Styles of Coping with Stress Inventory
This inventory is based on the Ways of Coping Styles questionnaire designed by Folkman and Lazarus.36 Sahin and Durak37 worked on the Turkish version of this scale and developed the Styles of Coping with Stress Inventory. This consists of 30 self-reported items on a 4-point Likert scale. The questionnaire has 5 subscales indicating different approaches to coping with stress: self-confident approach (7 items), optimistic (5 items), hopeless (8 items), seeking social support (4 items), and submitted (6 items). Cronbach α values for the subscales were calculated as 0.92, 0.86, 0.88, 0.94, and 0.84. The overall Cronbach α value for Styles of Coping with Stress Inventory is 0.90. A higher scores on any subscale indicates that the subject uses that approach to cope with stress. We used the self-confident and hopeless subscales in our study. The individual can score from 0 to 21 on the SCS and from 0 to 24 on the HS. Subjects with higher scores on the SCS are regarded as using effective (problem-based) stress coping skills. However, subjects with higher scores on the HS are regarded as using ineffective (emotion-based) coping skills.
Statistical Analyses
The results of the items (pretest, post-test, first follow-up and second follow-up of TAS, SCS, and HS) were regarded as independent variables. The relations between demographic, smoking features, and results of the items were investigated using the χ2 test, Pearson correlation analysis, the independent samples t test, and 2-way repeated measures analysis of variance. Two proportions tests were used to analyze the difference between cessation success rates between the treatment groups. Independent factors affecting smoking cessation were investigated using logistic regression analyses. Minitab version 10 (Minitab, Inc.; available from: http://www.minitab.com/en-us/downloads/) was used for power analyses and the 2 proportions test. All the remaining statistical analyses were performed on SPSS version 13.0 (SPSS, Inc., Chicago, IL). P < .05 was considered statistically significant.
Results
Of the original 350 subjects included, 328 (93.7%) completed the study (22 dropped out, 13 from the study group). All the dropouts were regarded as relapsed. Data from the dropouts were excluded from the point at which they left the study. Among these dropouts, 15 participants experienced severe drug side effects (eg, abdominal pain, vomiting, atopic dermatitis) and their treatment had to be changed. We also were unable to contact 7 relapsed participants during data collection.
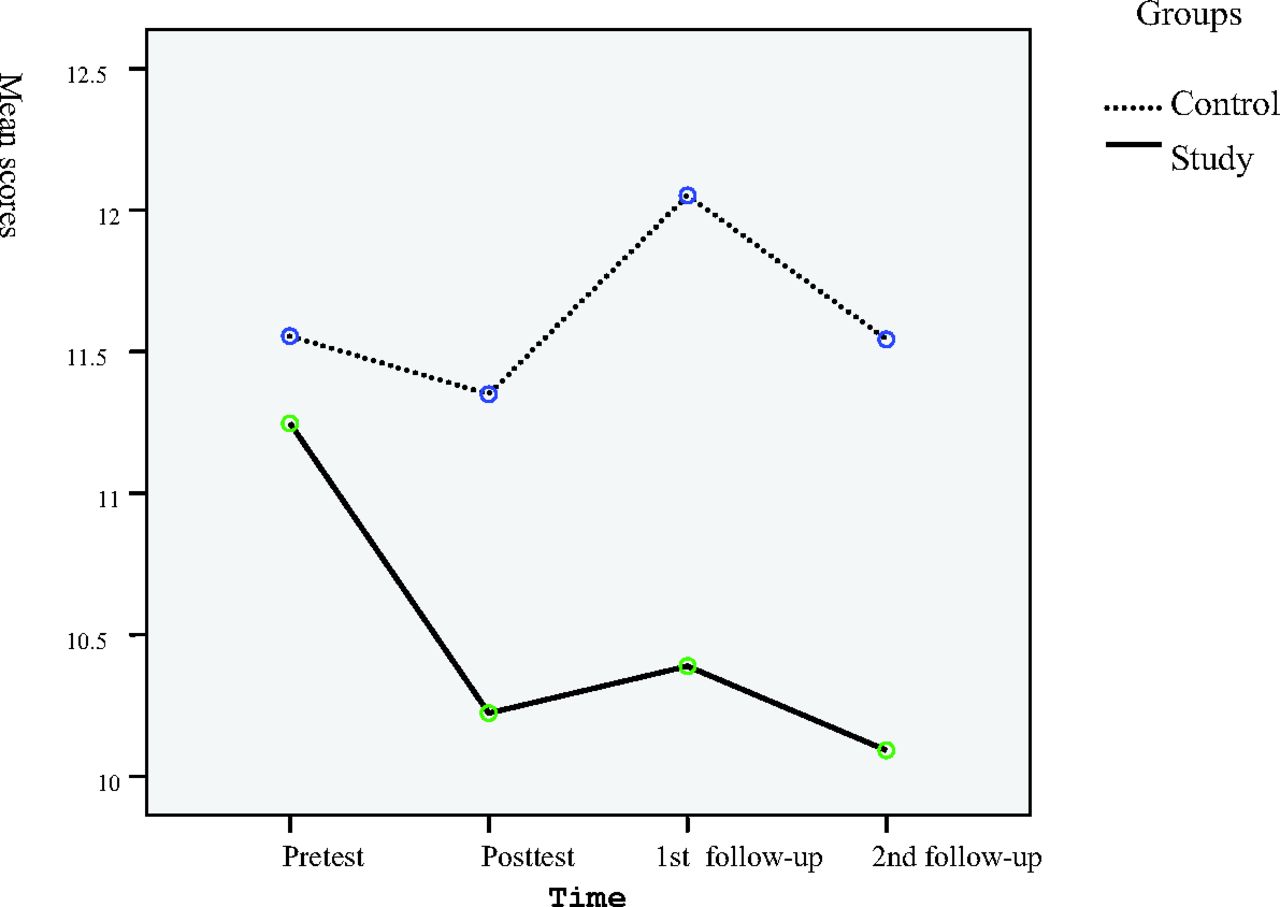
The epidemiologic and clinical features of the 2 groups and their statistical relations are shown in Table 1. Pretest, post-test, first follow-up, and second follow-up scores and their statistical relations within (study or control) or between groups (study and control) are presented in Table 2. There was no statistical difference between TAS, SCS, and HS pretest scores in terms of age, FNDT score, or package/year values in either group. However, women had higher pretest SCS scores compared with men (t = 2771; P = .006). Pretest, post-test, and first and second follow-up results for TAS, SCS, and HS were not statistically different in the control group (F = 1.201, P = .234; F = 1.018, P = .130; and F = 1.616, P = .148, respectively). They were, however, different in the study group (F = 25.041, P < .001; F = 13.506, P < .001; and F = 3.829, P < .01, respectively). The profile plots of the study and control groups' pretest, post-test, and the first and second follow-up mean TAS scores are shown in Figure 2, those for SCS in Figure 3, and those for HS in Figure 4. Although there was no statistical difference between the pretest scores of the 2 groups at the beginning of the study, the study group had lower scores on the TAS (t = 6.569; P < .001) and HS (t = 2.114; P = .03) and higher scores on the SCS (t = 6.918; P < .001), according to the post-test results. The first follow-up and second follow-up scores of the 2 groups' TAS (t = 8.851 and 12.798, respectively; P < .001 for both), SCS (t = 10.151 and 10.255, respectively; P < .001 for both), and HS (t = 5.564; P < .01 and t = 3.897; P = .02, respectively) results were statistically different from each other. The pretest TAS and SCS scores of the relapsed smokers compared with the smokers who quit were both statistically higher in the control group (TAS: 22.7 ± 3.8 vs 20.12 ± 2.4; t = 4.377, P < .001 and SCS: 49.83 ± 5.8 vs 46.72 ± 5.1; t = 3.181; P < .001). This significance was not observed in the study group, however (P > .05). Although there was no difference in the pretest scores for TAS, SCS, and HS, post-test SCS scores were higher in the BC + varenicline (mean, 14.10 ± 1.2; F = 2.377; P = .005) and BC + bupropion groups (mean, 14.31 ± 0.9; F = 2.589; P = .003) compared with the BC only (mean, 13.50 ± 1.3) and NRT (mean, 11.72 ± 0.8) treatment groups in the study group. The same relation also was observed in the control group. Post-test SCS scores were affected among the treatment types; varenicline exhibited the highest mean (mean,12.45 ± 1.0; F = 16.946; P < .001) compared with the other groups.
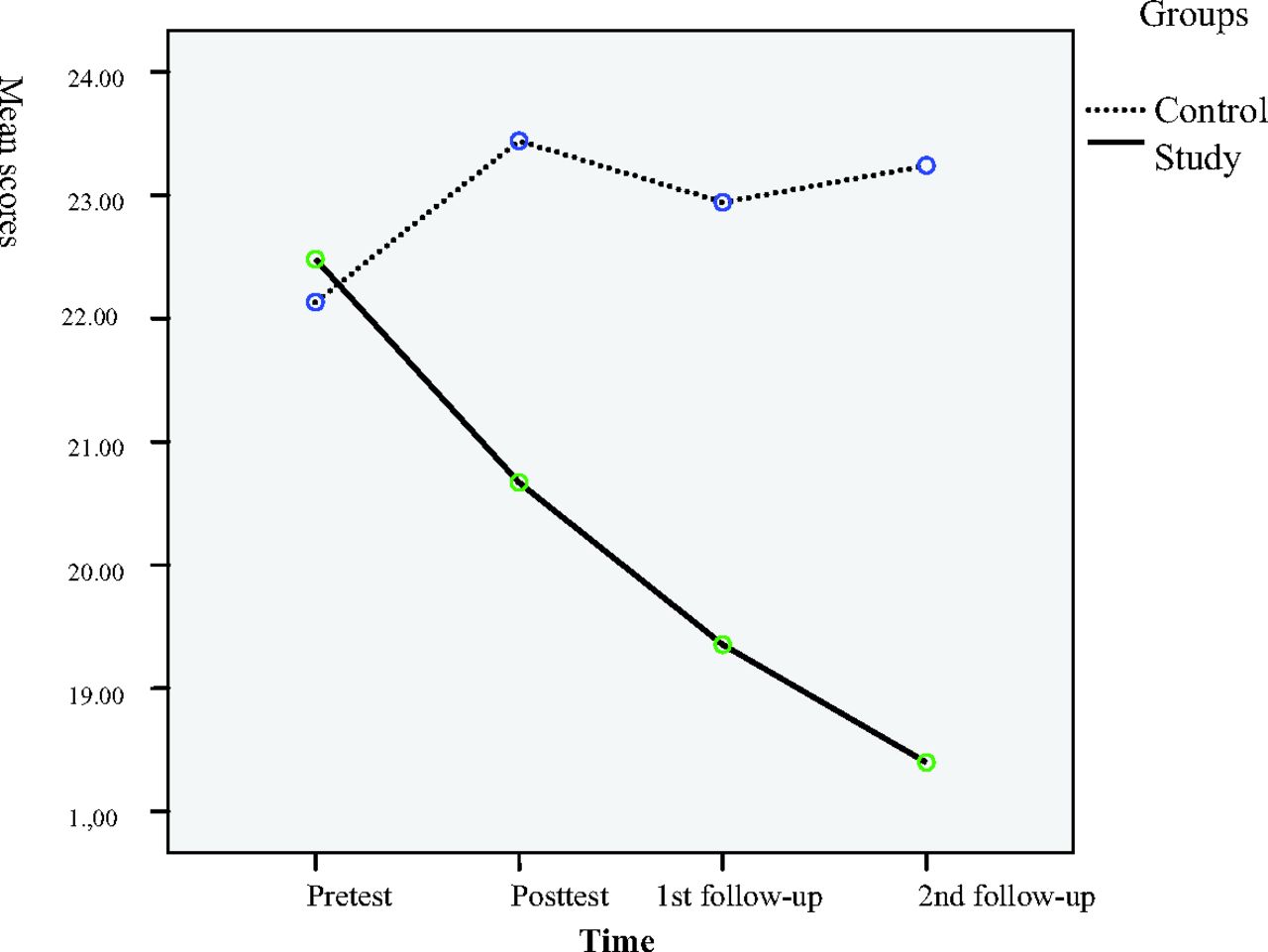
Comparison of estimated marginal means of pretest, post-test, and first and second follow-up tests for Trait Anger Scale of the State and Trait Anger Scale in the control and study groups.

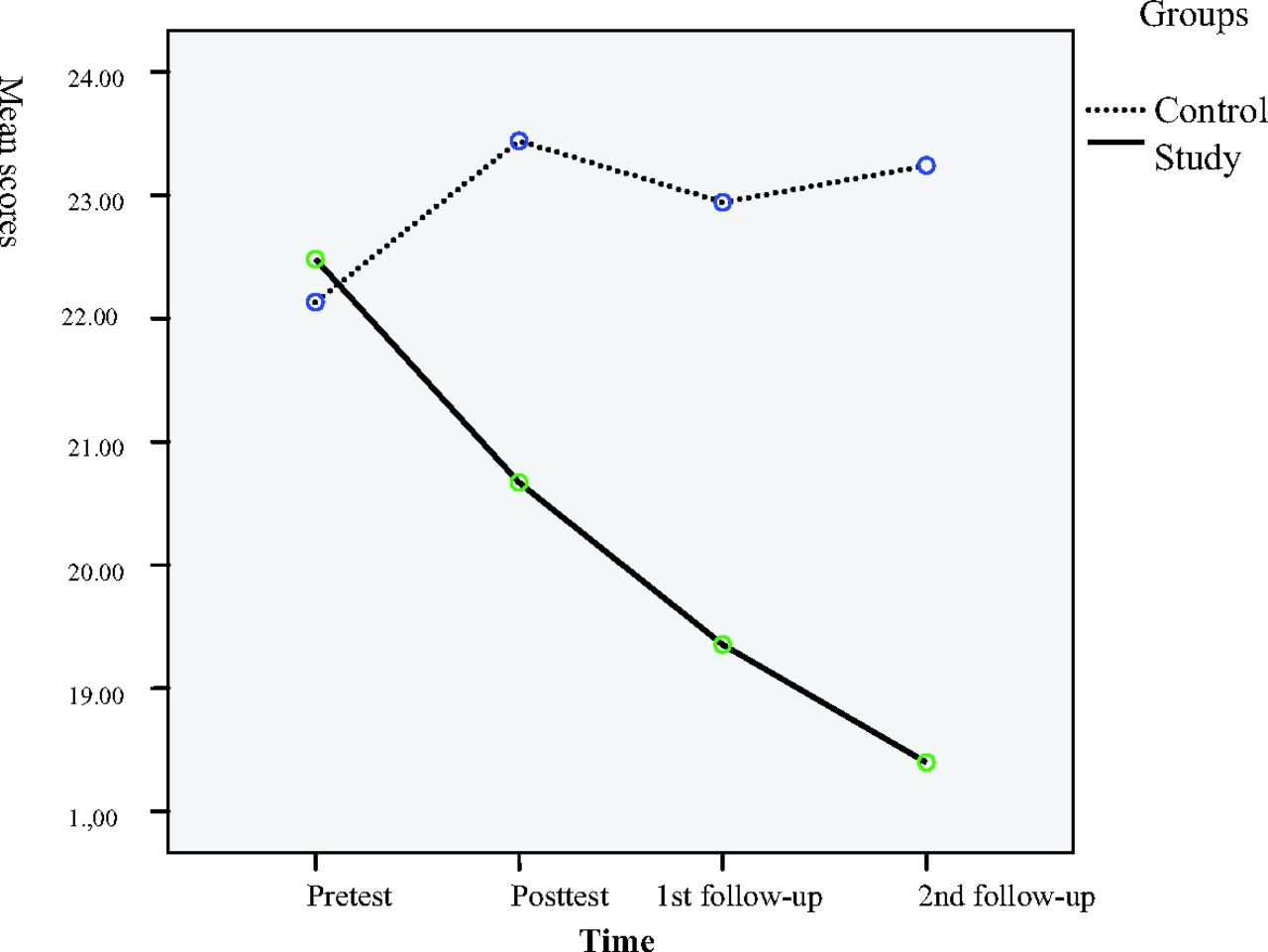
Comparison of estimated marginal means of pretest, post-test, and first and second follow-up tests for hopeless subscale of the Stress Coping Styles Inventory in the control and study groups.
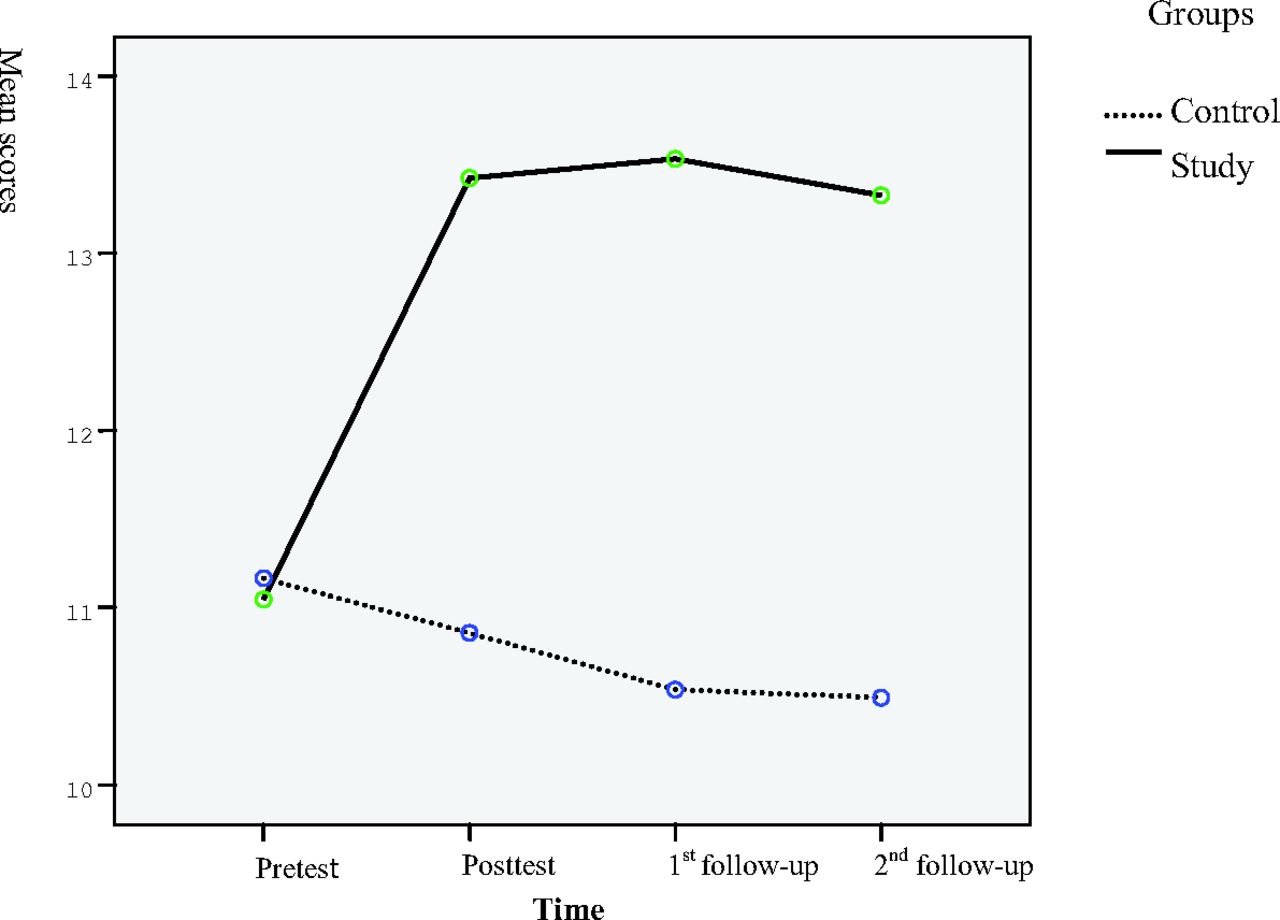
Comparison of estimated marginal means of pretest, post-test, and first and second follow-up tests for self-confident subscale of the Stress Coping Styles Inventory in the control and study groups.
The study group had a better quit rate at the end of the study compared with the control group (44% vs 27.4%; χ2 = 9.816; P < .001). Relapse rates in the first week and the first, third, and sixth months based on quit methods between the study and control groups are presented in Table 3. In the study group, success rates were 38% in the BC group (n = 11), NRT 46.3% in NRT (n = 21), 42.3% in bupropion (n = 19), and 46.4% in varenicline (n = 26) over the 6-month period. The equivalent results in the control group were 16.2% in the BC group (n = 5), 23.8% in NRT (n = 10), 28.8% in bupropion (n = 13), and 35.2% in varenicline (n = 20). Quit rate was not correlated with the selected cessation method (P > .05) at the end of the 6 months in either group. In the study group, 98 participants (56%) relapsed. Most of the relapses occurred in the first week and between the second week and first month. In the study group, one third of relapses occurred in the first week (n = 33, 33.6%), and another 27 smokers (27.5%) relapsed between the second week and the first month (61.1% of all relapses). The rates in the control group were 74 (58.8%) in the first week and another 29 (22.8%) between the second week and the first month (81.6% of all relapses).
A logistic regression model was used to investigate the factors affecting quitting smoking. First, the statistical significance between different variables (age, sex, marital status, application to join the anger management and stress control program, initial FNDT scores, packs per year, number of previous attempts at quitting, treatment groups, and pretest and post-test TAS, SCS, and HS scores) and cessation success was investigated. The final model was established from statistically significant correlations, application to the anger management and stress control program, and pretest and post-test TAS, SCS, and HS scores. This model is described in Table 4. According to this model, participation in the anger management and stress control program, low scores on the post-test TAS and HS, and higher scores on the post-test SCS were identified as factors in effective cessation for 6 months.
Discussion
The most striking result of this study was the higher quit rates in the study group compared with the control group (44% vs 27.5%) over 6 months. The National Institute for Health and Clinical Excellence regards a 27.5% quit rate in the first 6 months as favorable.29 However, the quit rate in our study group considerably exceeded these expectations. Our findings reveal that, compared with the control group, the participants in the study group who took part in the anger management and stress control program improved their self-coping anger and stress skills. However, the control group's trait anger scores were slightly elevated, and the percentage of participants using effective stress coping strategies remained unaltered during the study period, as confirmed in other studies.38,39 These data confirm the effectiveness of the program in promoting these skills, which may account for the increased quit rates in our study group. Our study highlights the importance of anger and stress in smoking cessation; participants with higher post-test scores on TAS and HS and low SCS scores were at risk for relapse. Cougle et al21 reported that anger experience was uniquely associated with a lifetime history of smoking cessation failure in 5692 adults from the National Comorbidity Survey. Early relapse is known to be a highly critical aspect of smoking cessation, and relapse rates within 2 weeks can be as high as 75%.40
In our study, most of the relapses occurred in the first week after cessation. Relapse rates during this period were 29.1% in the study group compared with 42.2% in the control group. It is interesting that the study group had a 22% lower relapse rate compared with the control group, although they had received only 3 sessions of the anger management and stress control program at that time. There is evidence of an association between increased trait anger and early relapse, which may be related to an increased tendency to experience situational irritants, leading to an increased craving to smoke.41 Perkins et al10 also reported that increases in anger levels after quitting were associated with relapse within 5 days. Swan et al11 detected the same relationship in 28-day relapse. Paterson et al20 more recently reported that patients (n = 117) who had self-reported increased pre- to post-quit state anger levels compared with other subjects (n = 130) were more prone to relapse (odds ratio [OR], 1.06; 95% confidence interval [CI], 1.01–1.10). Furthermore, smokers with increased anger after quitting relapsed almost twice as quickly as those with no increase in anger symptoms after quitting (hazard ratio, 1.98; CI, 1.32–2.96).
Specific cognitive and behavioral strategies are needed to maintain initial treatment success and minimize the rate of relapse. One such strategy is to help familiarize the patient with withdrawal symptoms and teach very basic techniques for anticipating and coping with common high-risk situations. This is used in many cessation programs. A second approach is to help the smoker promote permanent self-control. The efficiency of these 2 strategies was tested in our study. Both groups attended our standard quitting program, which uses many motivational and reinforcement strategies (face-to-face counseling, workshops, NRT, pharmacotherapy, and telephone and partner support). We provided the control group with anger management and stress control strategies for withdrawal symptoms twice, first in the workshop (group discussion) and again during the second visit (face-to-face counseling), which was on the quit day and scheduled for 10 minutes. However, the study group also spent 5 weeks in the cognitive behavioral therapy—oriented anger management and stress control program. Traditional disease-based models attribute smoking relapse to endogenous factors such as cravings or withdrawal, whereas cognitive behavioral theories emphasize contextual factors (eg, environmental stimuli and cognitive processes).42 Whether a high-risk situation culminates in relapse depends largely on the individual's capacity to exhibit an effective coping response, defined as any cognitive or behavioral compensatory strategy that reduces the likelihood of relapse. Cognitive factors involved in determining relapse liability, such as successful navigation of high-risk situations, may increase self-efficacy (the perceived capacity to cope with an impending situation or task) and thus in turn reduce the probability of relapse. Conversely, a return to the target behavior can undermine self-efficacy, increasing the risk of future relapses.43 Our program is mainly influenced by 2 different aspects that interact with one another in the relationship between smoking, anger, and stress. One aspect is smokers' use of nicotine as an ineffective and unhealthy way of coping with their anxiety, stress, and anger as a self-learned maintenance therapy.44,45 The other aspect, which is avoiding this phenomenon and promoting, perceiving, and increasing individuals' ability to select effective anger and stress coping strategies, is essential. There are 2 main ways of coping with anger and stress: problem focused and emotion focused.46 Problem-focused strategies, which we aim to promote among our participants with our program, use planned, learned activities to alter the situation that causes stress. We measured this variable with the SCS. Emotion-focused strategies are largely passive and concentrate on diminishing negative emotions, avoiding contact with stressors, and seeking psychological and social support, which we measured with the HS.
The effect of cognitive behavioral therapy on maintaining smoking cessation has recently been receiving increased attention. Thorndike et al47 reported that after 5-session cognitive behavioral therapy, although participants' compensatory coping skills were not enhanced, the success rate in the study group was 38% compared with 22% in the control group. Kapson et al48 reported that after 8 sessions of cognitive behavioral therapy participants' compensatory skills improved, with a success ratio of 33% over a 3-month period. However, both these studies were designed to investigate the effects of cognitive behavioral therapy on more or less depressive-prone smokers. Agboola et al49 investigated the effects of 36 skill-based relapse prevention studies in a systematic review. Cognitive behavioral therapies with relapse-based self-help interventions had a significant effect in increasing long-term abstinence (OR, 1.52; 95% CI, 1.15–2.01), and group counseling exhibited significant short-term efficacy (OR, 2.09; 95% CI, 1.14–3.85). We calculated the effect of our anger management and stress control program on cessation at 6 months as an OR of 2.09 and a 95% CI of 1.142 to 3.852.
Family practice mostly advocates horizontal health care services instead of longitudinal organizations (specialized centers) to deal with smoking cessation. This is particularly important in countries with a high prevalence of smoking. However, although family practitioners believe that they should recommend preventive and health-promotion activities, in practice they seem less likely to do so.50 In one large, multinational study across 11 countries (n = 2082), Brotons et al51 found that family practitioners regard a heavy workload, shortage of time, and lack of financial reimbursement as the main barriers to health promotion activities. Lack of adequate training and acquisition of proper skills for smoking cessation also are noted as barriers. Werner et al52 reported that more than half (57%) of family practitioners (n = 73) were using nonadherent motivational interviewing techniques when dealing with patients. Lack of motivation, training, support, educational resources, and protocols; concerns over low success rates; and failure to use the skills of the members of the primary care unit were identified as barriers to prevention activities on the part of family physicians. Family practitioners need highly successful, not time-consuming, easy-to-maintain, well-designed, collaborative health promotion activities. Our study revealed that the anger management and stress control program is more time/cost-effective compared to the individual approach (our clinic's standard treatment program). For the same amount of smokers (175 each) the same amount of time is required, however, the quit rates of patients who participated the anger management and stress control program are far higher. Calculated for a total of 175 participants, to achieve a 27.4% quit rate for the control group, we need 440 work hours compared with a 44% quit rate for approximately 420 work hours in the study group over 6 months.
Our study may have some weaknesses. One is the number of the participants. The behavioral therapies group sessions described were designed for no more than 20 participants (14 to 15 would be ideal), and there was only one therapy team available to teach them. This limited the number of participants. The other issue is isolating the effect of our program on smoking cessation. It is debatable whether the outcomes of the control group would have been better (quit rates and decrease in TAS, SCS, and HS post-test results) if they had received other types of group therapy on a different topic instead of individual follow-up. As described, in our standard program (control groups' treatment program) we also discuss anger management and stress control (tips, facts, and strategies) with all our participants at least twice (in the group during a workshop and individually during the second visit) for approximately 20 minutes each. Another design to isolate the effect would be to apply anger management and stress control activities individually or during group therapy. Cognitive behavioral therapy always works best with groups, so we decided to design our study in this way. The second dimension is the participants in both groups who used several techniques and medication types to quit smoking (BC, NRT, bupropion, or varenicline). As discussed earlier, NRT eased the effects of anger and stress, whereas varenicline and bupropion are mood modulators. Although participants who used varenicline in the study and control groups had better quit rates compared with smokers treated with BC and NRT in the control groups, the quit rates according to treatment type were not significant in the study group. It can be assumed that participation in the anger management and stress control program boosted the cessation effect of all the methods used in the study group. This may be attributed to several factors. The cessation effects of BC, NRT, bupropion, and varenicline are known to decrease in the mid- and long-term.50 In addition to the content of the anger management and stress control program applied to the study group, we used several different individual or group cessation techniques in both our groups (eg, self-help booklet, telephone consultation, face-to-face behavioral counseling). Another factor is that all the participants were highly motivated and directly sought help to quit smoking by applying to our departmental clinic. It is also possible that smokers with higher trait anger and worse ability to cope with stress might benefit more from this program.
Conclusion
The cognitive behavior—oriented anger management and stress control program had positive effects on reducing relapse rates. Cognitive behavioral therapy is a promising approach for smoking cessation activities. Further data are needed to investigate the effects of this kind of intervention in the short, mid-, and long term.
Appendix
The Agenda of The Anger Management and Stress Control Program
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication March 7, 2014.
- Revision received June 6, 2014.
- Accepted for publication June 16, 2014.




{kind=link}
{kind=link}
{kind=link}
{kind=link}