
Abstract
Background: Pharmaceutical abuse is a burgeoning problem, and various forms of drug diversion are becoming more common. At present, little is known about those who attempt to deceive physicians to receive medications, and even less is known about those who successfully avoid detection and abuse-related repercussions. The goal of this study is to assess the prevalence of attempted physician deception in a general population, explore common motives, and evaluate risk factors associated with the behavior.
Methods: A stratified random sampling technique was used to obtain a locally representative sample of 2349 young adults. The sample was 48.4% male, 68.9% white, 24.4% black, and 2.8% Hispanic. Selected individuals were surveyed using a self-report instrument (80.4% response rate).
Results: Of the respondents, 93 (4.0%) self-reported having attempted to deceive a physician to obtain a pharmaceutical. Most of these indicated that they were at least partially motivated by their own abuse. Approximately half reported that selling a portion of the prescription was a motivating factor. Alcohol use, marijuana use, and pharmaceutical misuse each were risk factors associated with attempted deception. Although no traits were definitively linked to the behavior, attempted deception was more commonly reported by men, Hispanics, self-identified lesbian/gay/bisexual/transgender individuals, and those at the lowest and highest extremes of the income spectrum. Logistic regression models of rare events indicated that past substance use along with sexual orientation and family income were related to attempted deception when controlling for other factors.
Conclusion: Results suggest that attempted physician deception may be more common than previously believed. Practicing physicians should attempt to use risk factor information presented within this study, albeit very cautiously. This study identifies general characteristics of young people who might divert medications but notes that only a small minority of any patient group will do so. Awareness should not equal bias in the treatment of these patients; instead, it should reinforce the need for careful clinical interviewing and the utilization of prescription drug monitoring programs and local law enforcement databases.
Despite intensified regulations and enhanced efforts to securely store, distribute, and closely monitor pharmaceutical products, prescription medication misuse has grown significantly in recent years. Among adolescents and young adults, pharmaceuticals now trail only marijuana and alcohol in terms of substance use.1 Findings from Monitoring the Future indicate that 7.9% of US high school seniors have misused prescription pain medications in the past year,1 and according to the National Survey on Drug Use and Health, use among young adults is even higher (9.8%).2 These actions are not without consequences; pharmaceutical misuse and abuse contributes to an estimated 1.3 million emergency department visits each year.3 While there is clear evidence that large quantities of pharmaceuticals are reaching unintended users,4,5 adequate detail about the routes of drug diversion is lacking.
Pharmaceutical diversion takes many forms. Patients may retain a portion of a needed prescription to sell, give away, or use themselves for recreational purposes.6,7 Theft from the supply chain or patients,4 fraudulently altered prescriptions,8 stolen prescription pads,9 international travelers,4 and “rogue on-line pharmacies”10 all likely partially contribute to the problem. Unethical or irresponsible prescribing practices remain a leading contributor11,12; “pill mills,” pain clinics, and unethical employees of pharmacies are of particular concern.12⇓–14 However, most ethical physicians focused on their own practice are likely more concerned with the final form of drug diversion—physician deception. Physicians must be concerned that some patients are “doctor shopping” to obtain prescriptions from multiple physicians for a single malady4,15 or that they are feigning or exaggerating symptoms to obtain a prescription for which they have no legitimate need. Unfortunately, this concern can negatively influence the regular practice of medicine because suspicions may lead to the undertreatment of pain in patients who are not feigning or exaggerating symptoms.11,13
This study focused on physician deception, broadly defined as any dishonesty on the part of the patient directed at gaining access to pharmaceuticals (including complete fabrication of pain and symptoms, exaggeration of actual pain or symptoms, or attempts to obtain medications for an already treated illness). Physician deception includes patients attempting to gain access to an unneeded category of drugs, stronger doses, more dosages, or a stronger than needed pharmaceutical. Virtually all studies focusing on patient-based drug diversion fail to directly assess physician deception. They either quantify the proportion of patients that misuse or divert their own medication16 or focus on abusers or traffickers who were identified by law enforcement or health care providers.4,6,17 Extant analyses also are largely limited to case or cohort studies,18 self-reports of identified heavy users,6 and analysis of records.19 As a result, our knowledge of pharmaceutical diversion may be overly reliant on the experiences of heavy users, and little is known about those involved in physician deception who avoid medical or legal repercussions.
A better picture of physician deception may originate from large random samples of the population that include successful “patients.” As such, we collected survey data from 2349 randomly selected individuals from a group with high rates of alcohol, marijuana, and prescription abuse to determine the prevalence of, and motives for, physician deception. Detailing factors linked to attempted deception will likely assist physicians who have traditionally received little direct training in assessing the truthfulness of patients. This may be particularly important because many of those inappropriately seeking medications may have honed their deceptive skills after attempting to deceive multiple physicians. Our study offers insights and suggests situations in which physicians may need to heighten their suspicions, but we stress that no traits are absolutely linked to deceptive behavior, nor should physicians underprescribe medications with abuse potential simply because a patient matches a profile associated with physician deception.11
Methods
Data
In 2012, a self-administered paper survey was administered to 2349 students in 15 randomly selected high-enrollment courses (>100 students) and 25 randomly selected moderate-enrollment courses (30 to 99 students) at a large university in the southeastern United States (institutional review board protocol H13032). Low-enrollment, laboratory, online, and physical education courses were excluded from the sampling frame. A single research assistant administered the survey in each course, and students in multiple courses were only eligible to participate once. No attempts were made to collect data from absent students. In total, 80.4% of the students initially enrolled in the selected courses completed the survey; we were unable to obtain records of withdrawals after the end of the first week of classes, withdraws, or medical and military leaves (these ineligible individuals were not removed from the denominator, and the reported response rate is a conservative estimate). Those unwilling to participate were instructed to return a blank survey; less than 50 students selected this option.
The selection process yielded a diverse and representative sample. The sample was 48.4% male, 68.9% white, 24.4% black, and 2.8% Hispanic; a total of 4.0% fell into other racial categories (Asian, Native American, other). These demographic characteristics largely resemble those of the university's overall population (48.5% male, 65.5% white, 25.0% black, and 4.2% Hispanic). The mean age of those in the sample was 20.06 years, and the median family income category was $75,000 to $99,999.
Measures
Physician Deception
Two questions assessed whether respondents had attempted to deceive a physician to obtain a pharmaceutical. Participants were asked, “Have you ever attempted to get a prescription from a physician for a medication that you did not need and intended to abuse?” and “Have you ever attempted to get a prescription from a physician for a medication that you did not need and intended to sell?” Those answering yes to either question were categorized as having attempted to deceive a physician for a prescription. Self-reported deviance and substance use measures such as these have been shown to be a valid way of assessing behavior in the field of criminology and better at quantifying behaviors that inconsistently result in arrest.20⇓⇓⇓⇓–25 With regard to substance use, studies pairing self-reported behavior with biological specimens typically indicate a high concordance between the 2 measures.26⇓⇓–29 Of the 2349 respondents, 93 (4.0%) admitted to having attempted to deceive a physician. A large portion of those attempting to deceive a physician (39.8%) attempted to do so for both purposes, but the 2 motives also were examined separately: 82 (3.5%) reported deception for the purpose of abuse and 48 (2.0%) reported deception to sell.
Demographics and Predictor Variables
Among the demographic measures included are age; sex; race (collapsed to white, black, and other); athletic participation; Greek affiliation (sorority/fraternity); employment status; marital status; housing situation; and family income (measured on a 9-option ordinal scale). These are characteristics that a physician is likely to easily observe and that patients, regardless of whether motivated by an underlying medical condition or to inappropriately obtain pharmaceuticals, are likely to answer honestly. Participants' self-reported sexual orientation and drug use (tobacco, alcohol, marijuana, misuse of pharmaceuticals [operationalized by collapsing separate items that quantified prescription as stimulant, pain killer, and sedative misuse]) also were recorded. Although these variables are typically accurately reported on anonymous surveys,22,30 patients may not as honestly report drug use to physicians31,32 as they do the aforementioned demographic characteristics. Initial analyses (Table 1) used dichotomous user/nonuser substance use measures, whereas later regression models incorporated continuous frequency variables (days used in the past month).
Analytic Strategy
To identify the traits most associated with attempting physician deception, the number and percentage of respondents in each demographic category who reported ever having attempted to deceive a physician for pharmaceuticals for any reason, having done so for abuse, and having done so for financial reasons were examined. Next, the rates of attempted physician deception among recreational users of alcohol, marijuana, and pharmaceuticals were contrasted with nonusers of those respective substances. The 3 dependent variables then each were regressed onto demographic characteristics to determine which factors are predictive of physician deception, controlling for all others. Because physician deception is somewhat rare among the population, traditional logistic regression models are inappropriate because they may both bias standard errors and significantly underestimate the probability of the outcome reported by a very small portion (< 5%) of the sample, regardless of sample size.33
Therefore, we used King and Zeng's 33,34 correction for binary analyses in which the “events” occur far fewer times than the “nonevents.” Their methodology was designed with outcomes such as wars, political conflicts, and infectious diseases outcomes in mind, but it has utility for the study of rare drug use behaviors.35 King and Zeng34 suggested incorporating a correction factor (ie, Pr (Yi = 1) ≈ π̃i + Ci where Ci = (0.5 − π̃i) π̃i x0V(β̃) x′0) since Pr (Yi = 1) ≠ π̃i with rare events). This rare event correction prevents the significant underestimation of the probability of the event that could occur with standard logistic regression models and also yields appropriate standard errors. The results from these models (estimated using Stata version 10; StataCorp., College Station, TX) can be interpreted in the same way as traditional logistic regression models but are appropriately considered more conservative than alternative analyses.36
Alcohol, marijuana, and recreational pharmaceutical use were added to a second rare events logistic regression model for each outcome so that the relationships of each characteristic with the outcomes could be evaluated independent of substance use. Predicted conditional probabilities of physician deception are graphically depicted to elucidate the complex relationship between income and physician deception.
Results
The percentage of each demographic group that has attempted to deceive a physician to obtain a prescription is displayed in Table 1. A χ2 test indicated that a significantly larger portion of men (4.8%) than women (3.1%) reported deception. The difference also was seen for both motives, although it is proportionally larger for selling (2.7% of men, 1.4% of women). Whites and blacks reported similar rates for each outcome, but a significantly larger portion of those in the “other” race category reported deception (7.8%). Additional analyses indicated that deception in this group was most frequently reported by those identifying as Hispanic or Native American (approximately 1 in 7 have attempted deception) and was reported by no Asian or Indian respondents. There seems to be no relationship between age and attempted deception within the age range of this sample. Urban residence and marital status were similarly unrelated to the outcomes (data not shown).
A significantly larger portion of student athletes reported deception. Twice the percentage of athletes reported attempted deception for the purpose of abuse (7.2% vs 3.3% of nonathletes) and 4 times the percentage reported attempted deception to obtain pharmaceuticals to sell (5.6% vs 1.8% of nonathletes). Greek affiliation (sorority/fraternity) was associated with deception for the purpose of selling (3.5% vs 1.8%) but not for personal abuse. Deception also seems to be strongly associated with sexual orientation. Of those who self-identify as lesbians, gay, bisexual, or transgender (LGBT), 14.1% reported attempted physician deception. All reported attempting deception for abuse, and 10.9% of LGBT respondents reported attempting deception to obtain pharmaceuticals to sell. Because of the small number of LGBT respondents, a cell within the contingency table used to calculate χ2 values would have <5 expected cases. Therefore, for this row of Table 1 only, Fisher exact test was used to assess significance.
Employment status was associated with each outcome. In each case, a significantly larger portion of those with full-time employment reported deception. An interesting relationship between family income and deception also emerged. The income groups that reported the highest rates of attempted deception were the lowest (<$10,000 annually; 9.2%) and the highest categories (≥$175,000; 9.0%); the lowest rates of deception were reported by the 4 middle groups (from $50,000 to $149,999). This pattern held true for both individual motives, although the high-income group's higher rate of attempted deception for financial purposes was not as pronounced as it was for the abuse motive.
Attempted physician deception was reported very rarely by nonusers of alcohol (1.0%) and marijuana (0.8%) compared with alcohol and marijuana users (4.4% and 6.2%, respectively). However, use of alcohol was associated only with deception for the purpose of abuse and not with deception for the purpose of selling. As would be expected, self-reported pharmaceutical abuse was strongly associated with physician deception. The percentage of pharmaceutical misusers who reported attempted physician deception was 8 times that of nonrecreational users for each outcome. Of pharmaceutical misusers, 9.5% reported attempted deception, 8.6% reported deception for the purpose of their own use, and 4.7% reported deception to obtain pharmaceuticals to sell. Thus, it seems that although it is somewhat rare in the general population, physician deception is practiced by approximately 1 of every 10 individuals who have recreationally used a pharmaceutical. The behavior is even more common among recent pharmaceutical misusers (11.4%).
Rare events logistic regression models are presented in Table 2. Because the low and high extreme income categories were most closely associated with attempted physician deception, both a linear and quadratic term were incorporated into the model to account for the apparent curvilinear relationship. In the first model, sexual orientation (b = 1.32; odds ratio [OR], 3.75), full-time employment (b = 1.15; OR, 3.16), other race (b = 0.79; OR, 2.19), and income (linear coefficient b = −0.56; OR, 0.57; quadratic coefficient: b = 0.06; OR, 1.06) were significantly associated with an increased likelihood of reporting attempted deception, whereas sex, age, and Greek affiliation were not. As expected, income seems to have a curvilinear relationship with the outcome. Alcohol, marijuana, and recreational pharmaceutical use are added to the second model. With the exception of “other” race, all significant variables in the first model retained significance at the 0.05 level. Alcohol (b = 0.17; OR, 1.19) and pharmaceutical misuse (b = 0.034; OR, 1.40) were also significant in this model.
The third model examines attempted deception only for the purpose of abuse. Before the inclusion of substance use, sexual orientation (b = 1.45; OR, 4.28), full-time employment (b = 1.29; OR, 3.63), other race (b = 0.90; OR, 2.47), and income (both the linear and quadratic terms) had significant associations with attempted deception. Each of these and pharmaceutical misuse (b = 0.35; OR, 1.42) had significant associations with the dependent variable after the inclusion of the 3 forms of substance use. The same variables (sexual orientation, full-time employment, other race, and income) were associated with physician deception for the purpose of selling in the fifth model. Once substance use was added, both income terms were reduced to marginal significance. Pharmaceutical misuse (b = 0.38; OR, 1.46) and athletic participation (b = 1.04; OR, 2.83) were also significant in the final model.
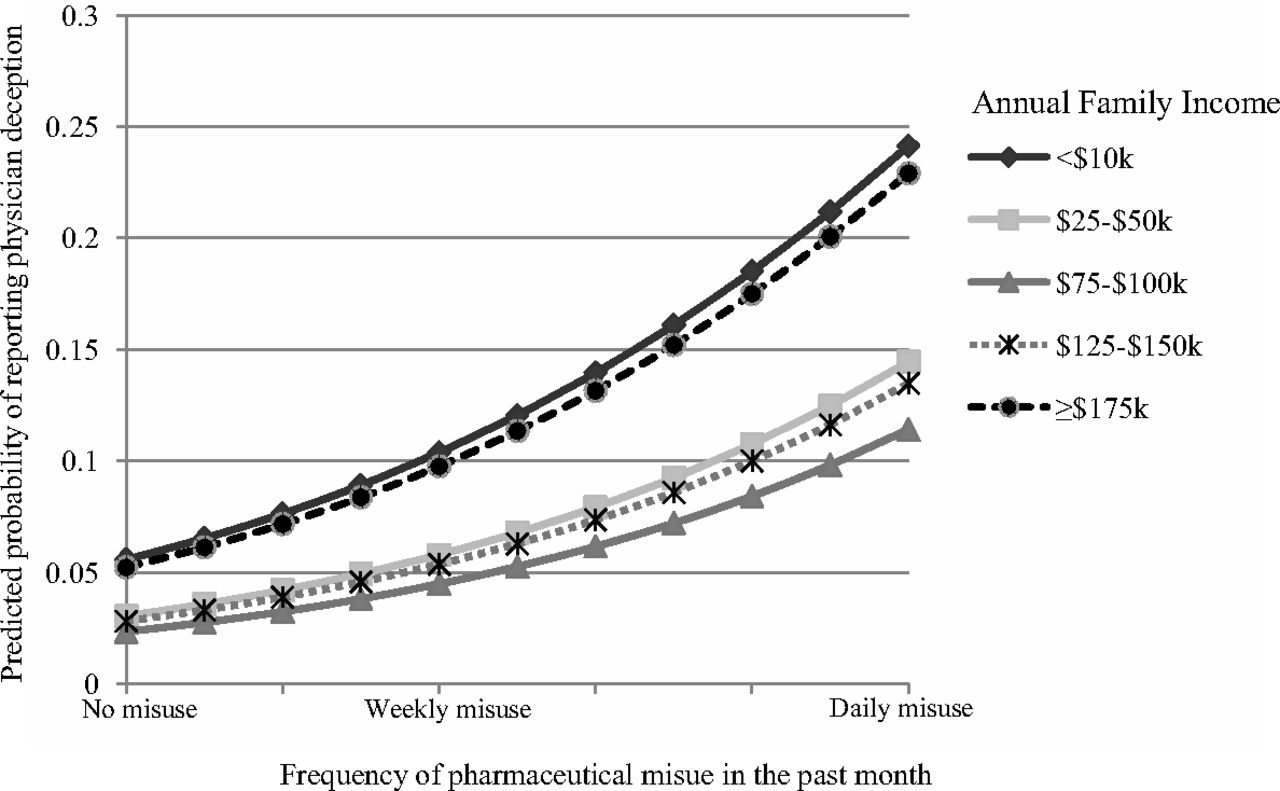
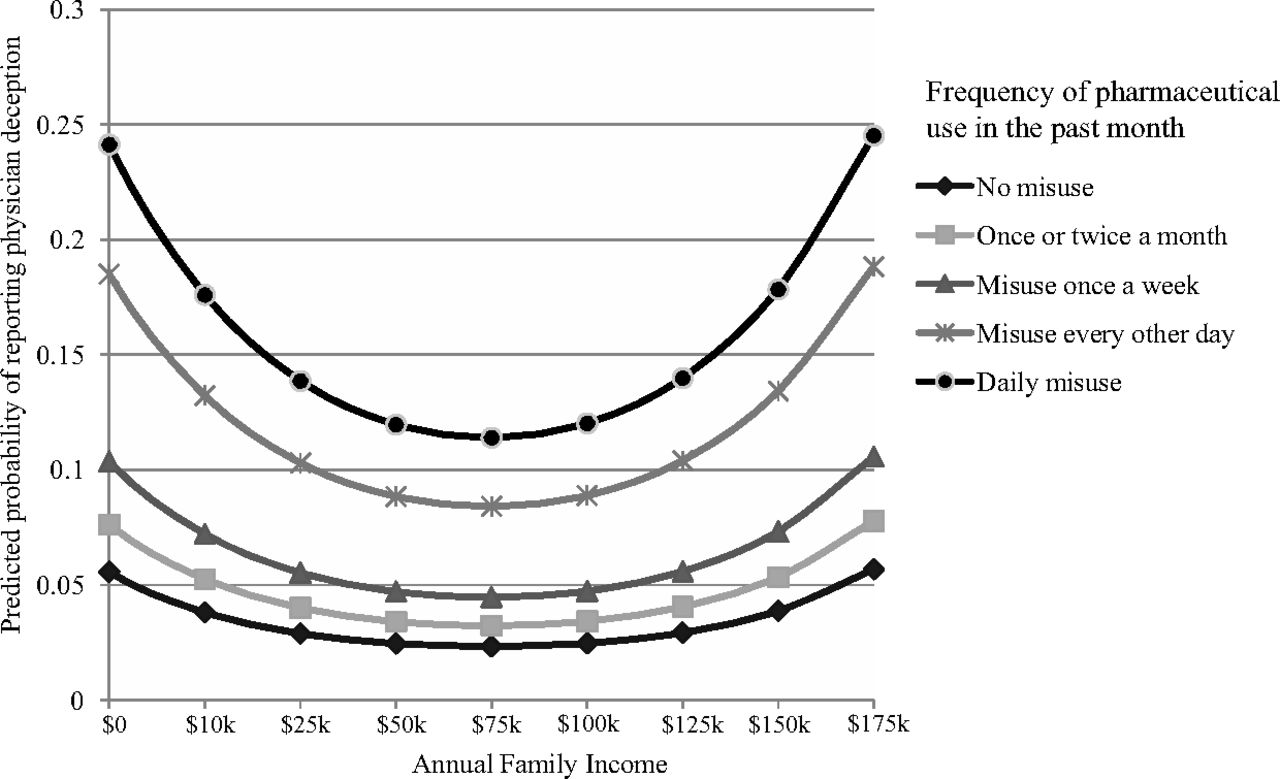
To better clarify the relationship between income and attempted deception to obtain pharmaceuticals, Figures 1 and 2 display the predicted probability of attempted deception at various pharmaceutical misuse and income levels, respectively. In each, all other predictor variables were held constant at their mean. The figures clearly depict 2 key findings: the predicted probability of attempted deception increases with the frequency of pharmaceutical misuse and is at its highest at the extremes of the income measure. Those with moderate family incomes have the lowest likelihood of attempted deception, whereas the poor and the affluent are most likely to report attempted deception.
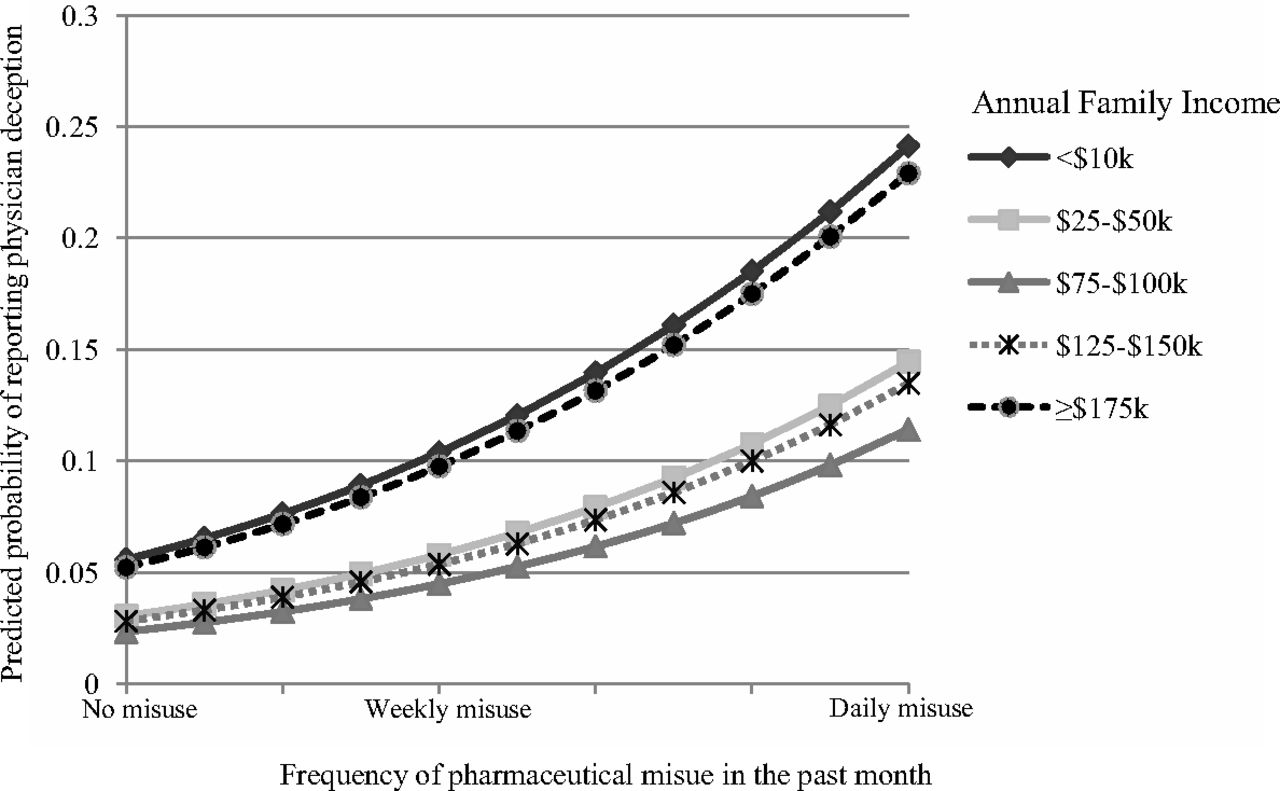
Predicted probability of physician deception across a range of pharmaceutical misuse.

Predicted probability of physician deception across a range of family incomes.
The respondents who did report deception were asked whether they had ever been successful at using deception to obtain a pharmaceutical that they did not need. Unfortunately, the option choices were worded in a way that only yielded limited information. Of the 93 attempting deception, 29 (31.2%) were always unsuccessful and 64 (68.8%) were successful “at least once.” This form of measurement fails to differentiate between successful respondents who only attempted deception once, those who were virtually always successful, and those who might have only been successful in 1 of 10 attempts. Ideally, the survey would have included follow-up items related to how often they had attempted deception, the percentage of times they were successful, and how many different physicians they had attempted to deceive. As a result of these limitations and because physicians need insight into those trying to deceive them, our focus remains attempted deception rather than successful deception.
Discussion
Several key findings emerged from the analysis. Those who reported attempted physician deception were more likely to be male, Hispanic or Native American, and identify as LGBT. Our analysis also suggests that those at the extremes of family income distributions are most likely to attempt to obtain unneeded prescriptions. Those living in extreme poverty or an upper-middle class or above household were far more likely to report attempted deception than those in the middle 90% of incomes. Thus, it seems that physicians may not only need to be additionally cautious when prescribing abused medications to those living below the poverty line but also to those with extensive financial resources and likely those with quality health insurance. However, no measure of health insurance coverage or quality exists in the data set to assess the relationship between insurance and deception.
A history of substance use, both licit and illicit, seems to be one of the strongest predictors of attempted physician deception, but 4 demographic predictors remained important after controlling for substance use: race, sexual orientation, employment status, and income. As would be expected, physicians should consider substance users to be more likely to feign symptoms for medications. Our study suggests that alcohol users are 5 times more likely to attempt to get pharmaceuticals to abuse and twice as likely to attempt to get pharmaceuticals to sell. Marijuana users and pharmaceutical misusers are each 8 times more likely to report each behavior than nonusers. The finding that marijuana use and pharmaceutical misuse are near equal indicators of attempted deception (independent of controls) suggests that they can be equally useful to the physician in identifying potential deceptive patients. While deceptive patients would most certainly deny a history of pharmaceutical misuse, they may admit marijuana use, particularly given its increased acceptance in recent years.37,38
Our research suggests that the profile of the deceiver is distinct from that of a pharmaceutical misuser. While misusers are more likely to be white,39⇓–41 attempted deceivers are more likely to be Hispanic or Native Americans. Also, while use is higher in rural areas,40,42 attempted deception was not associated with the size of participants' home communities. Deceivers were more likely to be male, as is the case for pharmaceutical misusers more generally,43 and our income findings mirror a previous study that noted pharmaceutical misuse was lowest within homes earning $40,000 to $75,0000 annually.44
Although this study provides the first detailed profile of patients attempting physician deception using a random sample of young adults, it is not without limitations. Young adulthood is associated with high rates of substance use, illicit behaviors, and dishonesty, but attempted physician deception is unlikely limited to this demographic. Future research should attempt to ascertain whether the rates noted in this study are mirrored in other age groups and nonuniversity populations. Furthermore, attempts to replicate the study should be made to determine whether the results presented here are generalizable to other regions and cultures and whether they remain consistent over time and to extend measurement to include items assessing the recency and frequency of attempted deception, specific drugs of interest, how physicians are selected before attempting deception, rates of attempted deception at specific locations, and rates of success. In addition, detailed interviews with those engaging in physician deception may shed light on the techniques and strategies frequently used and assist physicians in identifying behavioral markers for deception. Because deceivers did so both to acquire pharmaceuticals for their own use and to sell, we caution physicians to approach these cases carefully given the potential for violence associated with severe addictions and the drug trade. Although this study did not inquire about whether deceivers also were willing to use threats, coercion, or violence to obtain pharmaceuticals, this is a crucial area for future research to help ensure the safety of physicians, medical staff, and other patients.
Practicing physicians should attempt to use the information presented within this study but should do so cautiously. Each of the demographic and substance use factors highlighted in the Results was significantly associated with deception but not ubiquitously and definitively linked to the behavior. The predictive utility of each explanatory model was below that which is associated with laboratory tests with which physicians may be familiar. This is not unexpected; criminology research typically only accounts for <20% of the variance in deviant behaviors.45 The etiology of honesty, intended behaviors, and actual behaviors can be challenging to evaluate, and predictive models are only tools that assist in the identification of potential issues. Even among those with each of the identified risk factors, the majority will be seeking necessary care rather than attempting physician deception. Thus, these findings should be used only to heighten suspicions and not definitively classify an individual as a deceptive patient. This information should always be used in unison with careful clinical interviewing. A profile consistent with deception and a suspicious interview should reinforce the need to check prescription drug monitoring programs and local law enforcement databases before proceeding. Once more, physicians should bear in mind that our study only identifies general characteristics of young people who might divert medications (eg, Hispanic or Native American, male, LGBT, low or very high income, and a history of alcohol and marijuana use) but that only a small minority of any patient group will do so. Awareness should not equal bias in the treatment of these patients.
While only a portion of medications used recreationally reach users via legitimate US prescriptions, diversion through physician prescription remains an issue. Pill mills and ill-intentioned physicians play a role, but as Hurwitz11 notes, the number of diverted medications clearly indicates that the problem is not limited to a few “bad apple” physicians. We suggest that the overwhelming majority of physicians are well intentioned but may each contribute marginally to the problem when deceived by a “doctor shopper” or an existing patient seeking stronger medications, larger quantities, and stronger doses. The compounding of these minor amounts of overprescribing, in combination with pill mills, likely accounts for much of the overall problem. The traits linked to attempted deception were carefully explored so legitimate physicians may be appropriately vigilant and avoid inadvertently contributing to recreational pharmaceutical use. Results suggest that substance users, sexual minorities, and those at extremes of the income distribution are more likely to engage in deception, but practitioners should only consider these factors as risks for deception, continuing to view and treat patients as individuals, as is ethically appropriate. The proliferation of prescription drug monitoring programs13 will likely continue help reduce diversion via pill mills and “doctor shoppers,” but they are not likely to identify situations where overprescribing is slight or infrequent. As such, legitimate physicians remain the front line and should equip themselves with every tool available, such as the presented profile of a deceiver, to limit their practice's contribution to the pharmaceutical diversion problem.
Notes
This article was externally peer reviewed.
Funding: This study was supported in part by funds from the Office of the Vice President for Research and the Jack N. Averitt College of Graduate Studies at Georgia Southern University. The office and college had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Conflict of interest: none declared.
- Received for publication March 28, 2014.
- Revision received June 10, 2014.
- Accepted for publication June 16, 2014.




{kind=link}
{kind=link}