
Abstract
We describe a case of peripheral intravenous catheter fracture occurring during a routine training exercise. The supervising instructor immediately placed a venous tourniquet proximal to the insertion site and urgently transported the patient to the hospital. The missing catheter segment was identified within the median cubital vein under ultrasonography and was removed by venous cutdown under local anesthesia. An investigation determined that reinsertion of the needle into the advanced catheter likely caused the fracture and that application of a tourniquet may have prevented embolism of the fractured segment. Our literature review suggested that peripheral intravenous catheter fracture is likely vastly underreported, with only one prior case identified in the English literature. Action was taken following the event to educate all Israeli Defense Force medical providers regarding both proper preventive measures and recognition and treatment of catheter fracture should it occur. This case highlights the importance of health care providers being aware of the possibility of catheter fracture, as well as steps to take to prevent and mitigate its occurrence.
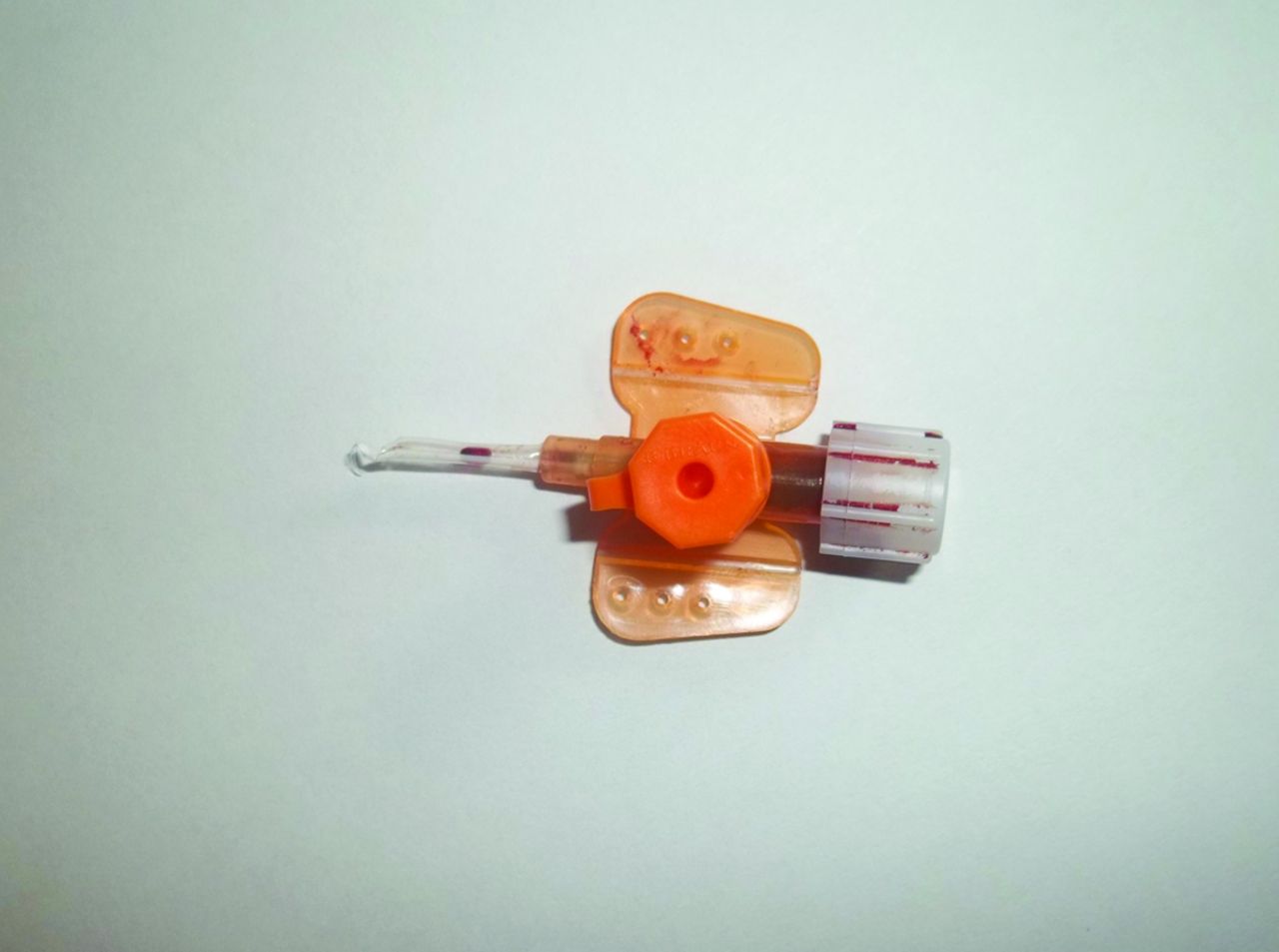
A 19-year-old military emergency medical technician encountered difficulty removing a 14-gauge peripheral intravenous (IV) catheter (Vasofix Safety, Braun Melsungen AG, Melsungen, Germany) during a routine training exercise. The device, which had been inserted at the antecubital fossa, was successfully withdrawn under the instructor's supervision. It was immediately recognized, however, that a large piece of the catheter had been torn off: only 1.5 cm of the 5-cm-long catheter were recovered (Figure 1). The instructor immediately placed a venous tourniquet proximal to the insertion point. Physical examination revealed a distinct cord-like object palpable under the skin at the insertion point. The patient was transported urgently to the hospital, where ultrasonography identified a foreign body within the median cubital vein. The object was removed by venous cutdown under local anesthesia and was identified as the missing catheter fragment. The patient had an uneventful recovery and was discharged from the hospital the next day.

The 1.5-cm proximal part of the intravenous catheter retrieved in the field.
Catheter fracture is a known complication of intravascular placement of plastic catheters; the first report we identified was by Turner et al1 in 1954, and numerous others have followed. The majority of these reports relate to the use of central line catheters, with catheter fragments ranging from 3.5 to 72 cm in length and resulting in a range of complications including sepsis, perforation, thrombosis, dysrhythmia, and myocardial infarction.2,3 Surprisingly, although the use of over-the-needle type peripheral IV catheters dates back to 1957,4 with wide-spread use beginning in the 1970s, to our knowledge embolism of fragments from fractured peripheral IVs has been reported in the English literature only by Singh et al.5
Following the incident, an after-action investigation was conducted. The findings suggested that the probable cause of the catheter fracture was partial transection from either trying to reinsert the needle into the already advanced catheter or advancing both catheter and needle with the needle partially withdrawn. This may have been further complicated by the anatomic curve in the vein at the antecubital fossa. In either case, attempts to remove the catheter likely completed the transection, leaving the intravascular distal fragment.
Actions taken by the Israeli Defense Force Surgeon General's Headquarters following the incident included revising the safety guidelines for peripheral IV insertion. Emphasis was placed on avoiding reinsertion of a needle into a catheter that was advanced even partially off the needle; this turned out to be especially important when using a 14-gauge IV catheter because it was found to tear up to two thirds of the catheter's circumference in a single puncture. Emphasis also was placed on the immediate application of a proximal venous tourniquet at first suspicion of catheter fracture to minimize the likelihood of fragment embolism, even when the broken-off catheter tip is not visualized or palpated.
Fortunately, the rapid recognition and response by the supervising instructor likely prevented any major complications from occurring. Because these types of events are probably significantly underreported, it is essential that health care providers who insert peripheral IV lines be familiar with the potential risk of catheter fracture and the proper emergency interventions required once it occurs.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication March 13, 2013.
- Revision received May 20, 2013.
- Accepted for publication May 21, 2013.




{kind=link}