
Article Figures & Data
Figures
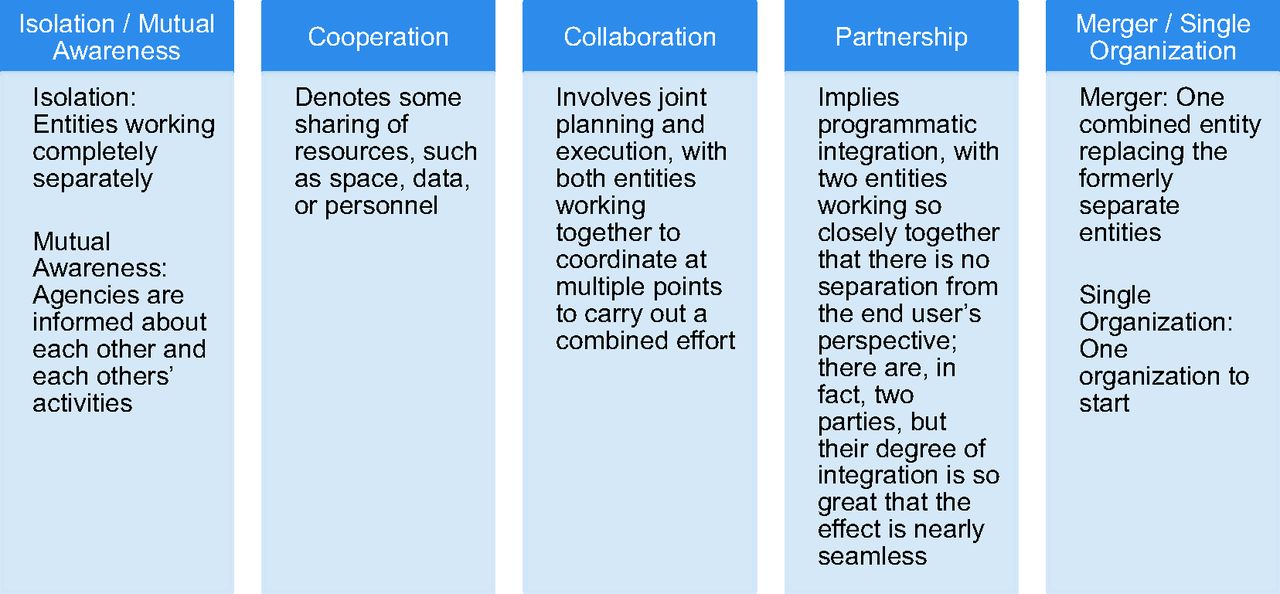
- Figure 1.
Relationships at the organizational level.
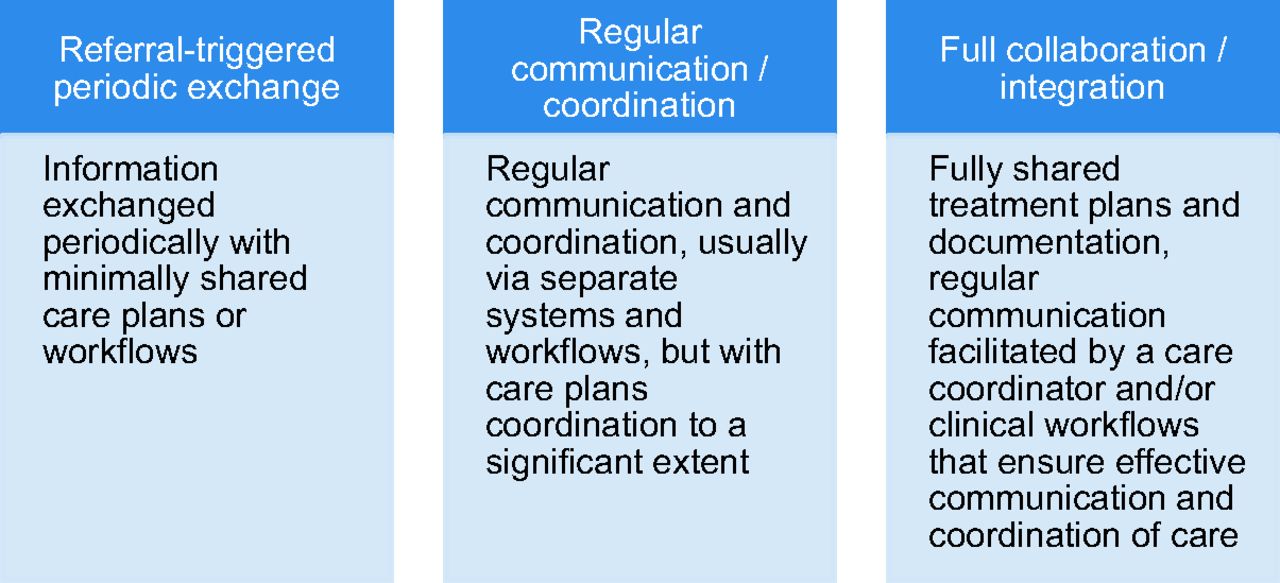
- Figure 2.
Relationships at the interpersonal level.

Tables
Research Questions Primary Data Type Description of Data Data Collection Process How do the ACT practices make the changes required to integrate care for patients? Documents Documents include grant applications, reports to TCHF, E-mail communications, innovator presentations, and documents from innovators (scheduling templates, educational materials). Documents are collected throughout the study period and during observation visits. The Program Office and grantees share documents freely. What factors enable and impede efforts to integrate care for patients, with particular attention to teamwork, information exchange, and shared decision making? Online diaries Members from each innovation team report their implementations experiences biweekly via an online journal that is shared with other members of their team and the evaluation team. The evaluation team identified 5 to 7 people on each grantee team, including practice members, to post diary entries. Each team has a private online diary room. Diary keepers were asked to post every 2 weeks. Evaluators interact with diary keepers to encourage posting. Observation visits Two-day visits with each innovation site to observe care delivery. During visits, 2 to 3 evaluators observed the care delivery process by shadowing clinicians, clinical support staff, and nonclinical support staff. This included observing huddles and other team meetings. Interviews Informal and semistructured interviews are conducted with the innovators, clinic members, and eventually patients. The evaluation team has informal discussions with innovators during meetings convened by the Program Office. In addition, we conduct semistructured interviews with 8 to 10 practice members during observation visits. Survey A survey was completed by each innovation team to collect information about each organization (eg, ownership, staffing patterns, turnover, panel characteristics). The evaluation team distributed surveys to one person at each ACT innovation site who worked with members of the practice to complete the information. Information was returned to us and data reviewed. Questions were clarified with teams as needed. TCHF, The Colorado Health Foundation.
- Table 2. ACT Innovator Site Characteristics Prior to Implementation (e.g., September 2011)
ID Practice Characteristics Patient Characteristics, % Type* Ownership Location† FTE, n (%) Annual Patient Visits (n) Female Sex, % Age (years) Race/ethnicity Insurance/Payer Mix Primary Care Clinicians Behavioral Health Providers ≤18 19–44 45–64 ≥65 White Black Hispanic Other Medicare Medicaid Commercial Uninsured 1 Single specialty FQHC, private Rural 6 (6) 2 (2) 31,200 54 19 35 40 6 65 0 35 0 10 25 35 30 2 Multispecialty FQHC, hospital system Urban 5 (3.15) 4 (0.9) 8,372 68 0 0 38 62 62 9 2 27 57 10 2 31 3 Multispecialty Clinician Urban 14 (10) 0 (0) 31,720 55 16 32 26 26 86 1 10 3 24 10 62 4 4 Mental health CMHC, nonprofit Rural 0 (0) 9 (6.9) 7,904 46 28 37 30 5 84 1 8 7 3 40 29 28 5 Multispecialty Clinician Urban 22 (13.6) 0 (0) 47,476 54 12 42 30 16 85 1 13 1 13 4 64 19 6 Single specialty FQHC, hospital system Urban 9 (9) 2 (1.4) 17,680 59 40 30 20 10 38 39 14 9 9 48 8 35 7 Single specialty Clinician Urban 6 (4.8) 0 (0) 15,600 55 10 41 36 13 88 1 9 2 4 0 91 5 8 Mental health CMHC, nonprofit Urban 0 (0) 26 (22.8) 4,732 42 0 50 47 3 74 5 9 12 1 58 1 14‡ 9 Multispecialty HMO, hospital system Urban 20 (18.7) 0 (0) 298,168 58 12 33 34 21 59 8 13 20 27 0 73 0 10 Single specialty Clinician Rural 2 (2) 0 (0) 4,680 55 22 17 25 36 60 0 40 0 6 5 69 20 11 Multispecialty FQHC, private Urban 11 (11) 2 (2) 14,924 63 41 37 17 5 41 1 4 54 7 30 7 56 ↵* Type is primary care unless noted otherwise.
↵† Determined using rural-urban commuting area codes: urban focused or rural focused (which includes all rural classifications).
↵‡ The total does not add to 100% because 26% of the organization's revenue comes from grants and contracts.
ACT, Advancing Care Together; CMHC, community mental health center; HMO, health maintenance organization; FQHC, federally qualified health center; FTE, full-time equivalent.
- Table 3. Characteristics of ACT Innovations, Including Key Evidence-based Integration Strategies
ID Description Providers Involved* Systematic Screening† Shared Medical Record‡ Spatial Arrangement§ Interpersonal Relations¶(Approach to Integration) 1 A CMHC is adding a full-time substance abuse counselor to an FQHC. They will develop a hybrid tool for substance abuse and depression and use the SBIRT model with every adult patient. They will provide CAC training to 3 staff members for dual credentialing. MD, DO, PA, NP MA, LAC Navigator, health coach Yes (PHQ9 and 4 questions on substance use, including smoking, alcohol, drugs) No Co-located Referral-triggered 2 A postdoctoral psychology training program is partnering with an FQHC that serves seniors to implement enhanced, computerized cognitive and psychological screening. The team will implement and track clinical use of the screening, provide a summary report to clinicians, provide follow-up treatment as requested, and monitor care pathways. MD, NP PhD, PsyD, postdoctoral trainees (PhD, PsyD), student interns (MA) No Yes Co-located Referral-triggered Regular communication and coordination 3 This privately owned primary care practice is automating behavioral health screening by implementing a kiosk and electronic tablets for use at check-in. This innovation expands current screening materials. The practice will work with information technology partners to develop coding necessary to integrate data into their EHR. MD, DO, PA, NP PhD Yes (PHQ2; PHQ9 if PHQ2 is positive) No Mostly separate Referral-triggered 4 A CMHC is developing a new integrated care clinic; this included building a new facility and bringing on a primary care team. They are using systematic screening and developing a Personal Health Profile (PHP) that extracts selected information from two separate behavioral health and medical EHRs to provided information about patients' behavioral and physical health needs at the point of care. MD, NP MD (psychiatry), PsyD, LPC, MSW, LCSW Yes (PHQ9, GAD7, AUDIT, DAST) No Co-located Regular communication and coordination Full collaboration and integration 5 Three private practices—a pediatric practice, family medicine clinic, and behavioral health center—are collaborating on this project. The behavioral health center is expanding services into family practice by delivering trainings on integration, developing a collaborative care schedule to increase consultations and warm hand-offs, and implementing systematic screening. MD, NP PhD, PsyD, LMFT, LPC, LCSW, CAC Yes (PHQ2; PHQ9 if PHQ2 is positive) No Mostly separate Referral-triggered Regular communication and coordination 6 A research team is working with an FQHC to develop a screening tool that assesses patients' behavioral health needs and treatment preferences. Clinic staff are implementing this tool in a practice with an onsite behavioral health provider and patient navigators, with the goal of establish consistent screening and referral of patients to their preferred treatment. MD, NPPhD, postdoctoral trainees (PsyD) Navigator No Yes Co-located Referral-triggered Regular communication and coordination 7 This privately owned primary care practice is partnering with a CMHC to hire, train, and supervise a co-located behavioral health provider. They are also expanding health coach services. The practice is exploring ways to finance and sustain these services. MD, DO, PA, chiropractic MSW, LSW Health coach Yes (PHQ2; PHQ9 if PHQ2 is positive) Yes Co-located Referral-triggered Regular communication and coordination Full collaboration and integration 8 This is a partnership between an FQHC system, a substance abuse treatment center, and a CMHC. The CMHC is the site of the intervention. They are embedding a primary care team, including a physician's assistant, medical assistant, care coordinator, and substance abuse counselor, into 3 CMHC locations of care. PA MD (psychiatry), LSW, LPC, LCSW, BA, CAC, LAC Care manager Yes (access to PC; brief screen for depression, anxiety, and substance use, including smoking, alcohol, drugs; if positive PHQ9, AUDIT, DAST, GAD7) No Co-located Referral-triggered Regular communication and coordination Full collaboration and integration 9 This system is co-locating behavioral health providers in primary care clinics to provide patients with solution-focused interventions and facilitate referral to other organizational resources (eg, long-term therapy, case management). These behavioral health providers also provide some consultations to medical clinicians upon request. MD, PA, NP PhD No Yes Co-located Referral-triggered Regular communication and coordination 10 This solo, privately owned primary care practice is partnering with a nonprofit mental health center to embed a behavioral health provider into the practice. The practice will employ systematic screening and develop referral protocols. The behavioral health provider will provide therapy for patients with poorly controlled chronic diseases. MD, MSW Yes (PHQ2; substance use, including smoking, alcohol, drugs; domestic violence) Yes Co-located Referral-triggered Regular communication and coordination Full collaboration and integration 11 This FQHC will increase screening and behavioral health services for newly identified pregnant women by adding a psychology fellow. The fellow will screen patients, offer brief therapy, and follow-up with patients, as needed. All eligible patients receive a follow-up screen at six weeks postpartum. MD, PA, NP PhD, Post-doctoral trainees (PhD, PsyD), student interns (MA) Yes (PHQ9, GAD7, AUDIT) Yes Fully shared Regular communication and coordination Full collaboration and integration ↵* Types of providers involved included medical doctor (MD); doctor of osteopathy (DO); physician assistant (PA); nurse practitioner (NP); clinical psychologist (PhD); doctor of psychology (PsyD); masters-level psychologist (MA); bachelors-level therapist (BA); masters of social work (MSW); licensed social worker (LSW); licensed professional counselor (LPC); licensed clinical social worker (LCSW); licensed marriage and family therapist (LMFT); licensed addictions counselor (LAC); certified addictions counselor (CAC).
↵† Uses a method to identify members of the clinic population who need or may benefit from behavioral health services. We report the behavioral health screenings used because 9 of the 11 innovations occurred in primary care settings that already had systematic protocols for detecting needs around common medical conditions (eg, diabetes). Behavioral health screenings included the 2-item Patient Health Questionnaire (PHQ2), and the 9-item Patient Health Questionnaire (PHQ9) (for depression); the Alcohol Use Disorders Identification Test (AUDIT); the Drug Abuse Screening Test (DAST); and the 7-item Generalized Anxiety Disorder Screen (GAD7).
↵‡ One record was used to record both physical and behavioral health information.
↵§ See Peek and colleagues5 for definitions.
↵¶ See Figure 2 and Peek and colleagues5 for definitions. If an innovator uses multiple approaches, the predominant interpersonal relationship strategy is italicized.
ACT, Advancing Care Together; CMHC, community mental health center; EHR, electronic health record; FQHC, federally qualified health center; SBIRT, Screening, Brief Intervention, and Referral to Treatment.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Examining the incidence of acute stress in pediatric trauma patients
- Large-Scale Implementation of Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
- Approaches to Behavioral Health Integration at High Performing Primary Care Practices
- Designing health information technology tools for behavioural health clinicians integrated within US-based primary care teams
- From Our Practices to Yours: Key Messages for the Journey to Integrated Behavioral Health
- Understanding Care Integration from the Ground Up: Five Organizing Constructs that Shape Integrated Practices
- Advancing Care Together by Integrating Primary Care and Behavioral Health
- Electronic Health Record Challenges, Workarounds, and Solutions Observed in Practices Integrating Behavioral Health and Primary Care
- REACH of Interventions Integrating Primary Care and Behavioral Health
- When Frontline Practice Innovations Are Ahead of the Health Policy Community: The Example of Behavioral Health and Primary Care Integration
- Designing Clinical Space for the Delivery of Integrated Behavioral Health and Primary Care
- Integrating Behavioral Health and Primary Care: Consulting, Coordinating and Collaborating Among Professionals
- Content Usage and the Most Frequently Read Articles by Issue in 2013
- Correction to "Integrating Behavioral and Physical Health Care in the Real World: Early Lessons from Advancing Care Together"
- Re: Integrating Behavioral and Physical Health Care in the Real World: Early Lessons from Advancing Care Together
- Patient-Centered Research Happens in Practice-based Research Networks