
Abstract
Background: Many adults have not been screened for colon cancer, a potentially preventable cause of death.
Methods: This was a randomized controlled trial conducted between December 2008 and April 2011 to improve CRC screening in 16 rural family physician offices. Subjects due for CRC screening were randomized within each practice to 1 of 4 groups: (1) usual care; (2) physician chart reminder; (3) physician chart reminder, mailed education, CRC reminder magnet, and fecal immunochemical test (FIT) (mailed education/FIT); or (4) all the preceding plus a structured telephone call to the patient from project staff to provide education, assess interest in screening, explain the screening tests, and address barriers (mailed education/FIT plus phone call). The main outcome was completion of any CRC screening.
Results: This study enrolled 743 patients. CRC screening was completed by 17.8% in the usual care group, 20.5% in the chart reminder group, 56.5% in the mailed education/FIT group, and 57.2% in the mailed education/FIT plus phone call group. We found no effect from the chart reminder compared with usual care (odds ratio [OR], 1.2; 95% confidence interval [CI], 0.7–2.0); and a beneficial effect from the mailed education/FIT (OR, 6.0; 95% CI, 3.7–9.6) and the mailed education/FIT plus phone call (OR, 6.2; 95% CI, 3.8–9.9). Both FIT and colonoscopy rates increased significantly in both mailed education groups.
Conclusion: CRC screening rates increased significantly among patients who were overdue for screening after they received mailed educational materials and a FIT. The addition of a phone call did not further increase screening rates.
- Cancer Screening
- Colorectal Cancer
- Early Medical Intervention (Educational)
- Practice-based Research
- Randomized Controlled Trial
- Reminder Systems
- Rural Health
It has been estimated that 50% to 80% of colorectal cancers (CRCs) are preventable or effectively treated if caught early.1⇓⇓⇓⇓–6 Several organizations in the United States have guidelines for CRC screening,7⇓–9 and the National Health Service in the United Kingdom has rolled out its screening program.10 Although screening rates are increasing, only about half to two thirds of eligible individuals in the United States and the United Kingdom have been tested for CRC.3, 11⇓⇓–14 The purpose of this study was to determine which physician and patient reminder systems were most effective for improving CRC screening rates in rural practices. These interventions were designed to remind the physician about CRC screening and provide education to patients to motivate and facilitate their screening.15⇓⇓⇓–19 Taken together, these interventions were intended to create an informed, activated patient and an informed, supported physician.20,21 This study compared 3 interventions with usual care for improving CRC screening rates and tested the hypothesis that screening rates would be higher with more intensive interventions.
Methods
The study was approved by the University of Iowa Institutional Review Board. Sixteen family medicine offices in the Iowa Research Network (IRENE) participated in this study. Each office received $1,000 for providing a list of their patients in the first year and $1,000 for each of the following 2 years of participation. Local office coordinators received $200 for completing certification for working with human subjects. Patient participants provided written informed consent and received $20 for completing a baseline questionnaire. Selection and recruitment details are described in detail elsewhere.22,23
Patient Recruitment
Briefly, patient recruitment took place by mailed invitation between December 2008 and April 2010. Practices provided a total of 56,015 names of patients aged 52 to 79 years, and a random sample of 8372 were invited. Patients from each office were recruited sequentially so that all patients from a given office who were selected to receive an invitation did so within the same week. Subjects were recruited using a modified Dillman technique,24 which included a pre-notice letter with a $2 bill followed by a full packet of materials 2 weeks later. Nonresponders were sent a reminder letter 3 weeks later, followed by up to 4 reminder calls to make sure they had no questions about the study; another full packet of study materials was sent if requested.22 The invitations were mailed on practice letterhead and had the electronic signatures of all office physicians and the principal investigator.
Baseline Questionnaire
The baseline questionnaire asked about family history of CRC; whether their doctor had ever recommended CRC screening; each screening method (how recently the method was completed, reason(s) the method was used). There also were 13 questions related to barriers to screening, as well as demographic questions. The questionnaire was tested and revised after being using in a previous study of 500 participants.12,25 Although they were developed independent of another questionnaire designed to assess CRC screening behaviors, many of the questions were similar.26 The answers on the baseline questionnaire were used to determine eligibility. Subjects were considered ineligible if they reported being up to date with CRC screening by any method (fecal occult blood [FOBT] or fecal immunochemical test [FIT] in the past year, barium enema or flexible sigmoidoscopy in the past 5 years, or colonoscopy in the past 10 years).7⇓–9 Only individuals due for CRC screening were eligible for the study because it was unnecessary to encourage screening among individuals who were already up to date. Based on self-report, the average rate of being up to date with screening across offices was 54.3% (standard deviation, 14.8%). Colonoscopy was by far the most prevalent screening test among those excluded from the study (51.4% were up to date with colonoscopy; standard deviation, 14.8%), indicating that the participating practices strongly preferred colonoscopy as a screening method.
Individuals with a family history of colon cancer, ulcerative colitis, Crohn's disease, or personal history of colon cancer were not excluded. Less than 1% had a history of ulcerative colitis or Crohn's disease and less than 1% had a personal history of CRC. There were no differences in these conditions across groups.
Medical Record Review
Medical records were reviewed an average of 15 months after the initial pre-notice letter was sent (range, 13.6–19.3 months). The timing of the review was chosen to allow time for the chart reminder and other interventions to have an effect, since healthy individuals may see their physician only once each year for a health maintenance examination. The form included the number and type of office visits in the preceding 26 months, information on types and dates of all CRC screening, results of flexible sigmoidoscopy and colonoscopy, and other preventive tests.12 A team of medical record reviewers visited each office to collect the data.
Randomization of Subjects
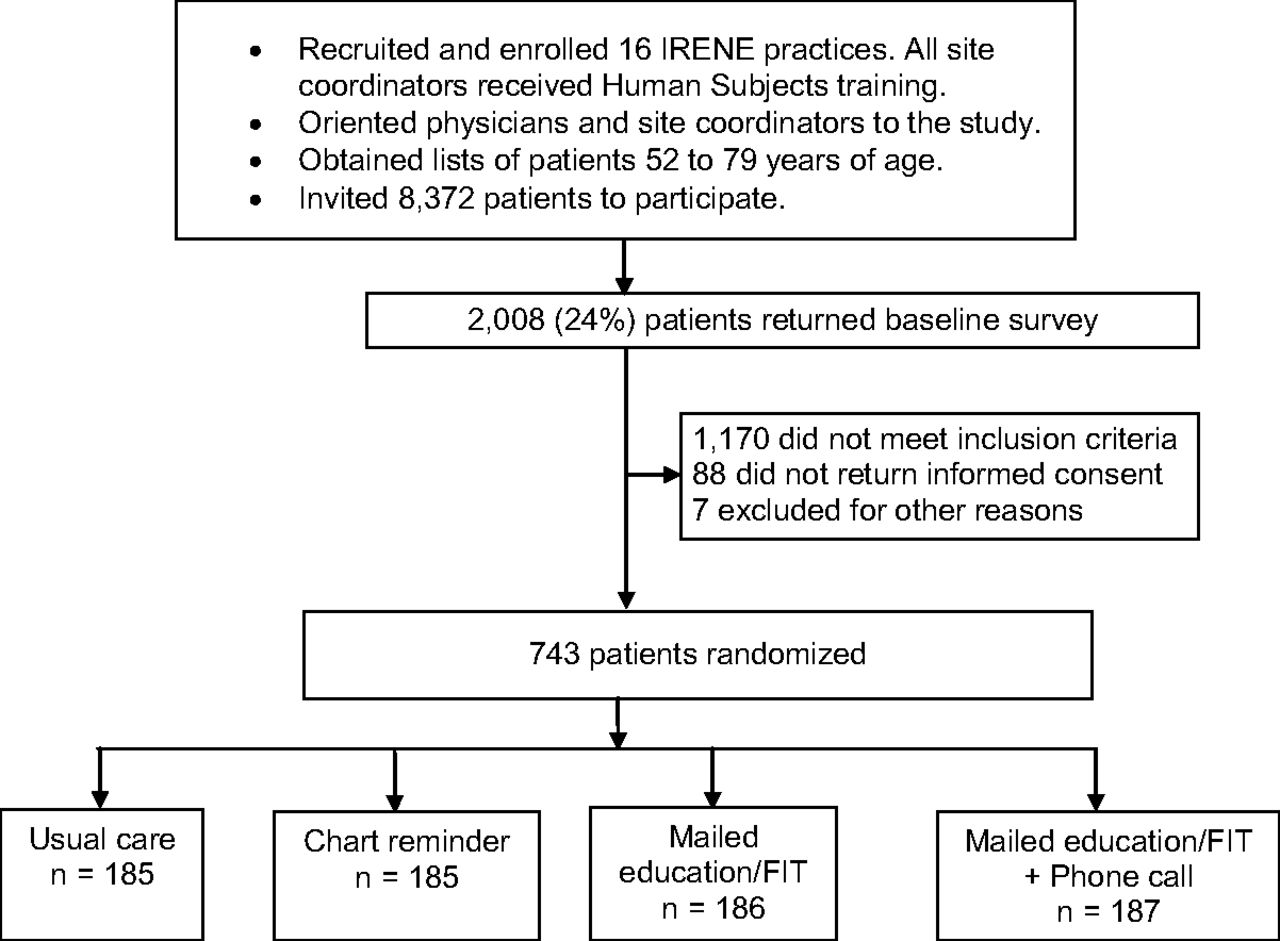
Figure 1 illustrates the recruitment procedure and study design. Of the 8372 invitation mailings, 743 patients (9%) returned a baseline survey with informed consent and met eligibility criteria. Eligible patients were randomized within each practice with equal chance in blocks of 8 to (1) usual care; (2) physician chart reminder (Figure 2); (3) physician chart reminder, written and DVD educational materials, a refrigerator magnet to remind the subject about CRC screening (Figure 3), and a FIT with a postage-paid return envelope (“mailed education/FIT”); and (4) all of the preceding items plus a structured telephone call from project staff to provide education, assess interest in screening, explain the screening tests, address barriers and preferences, and encourage screening (“mailed education/FIT plus phone call”).

Flow of patients through the colorectal cancer screening trial. IRENE, Iowa Research Network; FIT, fecal immunochemical test.
Colorectal cancer screening (CRC) reminder.
Iowans Get Screened magnet.
Randomization was performed using a computerized random number generator. For eligible patients who provided informed consent, the chart reminder was placed or programmed in the medical record for those assigned to the chart reminder groups. For offices that used paper charts (8 offices), the chart reminder (Figure 2) was on a paper Post-it note placed in the chart by the office coordinator. The office decided the best location for the chart reminder; in most cases it was on the left side when the chart is initially opened (where immunizations and medications are recorded). For offices using electronic records, the reminder was programmed. Thus, the physician chart reminder was placed in the charts of those patients who agreed to be in the study. Site coordinators signed a sheet verifying that the reminders had been placed, and at the time of medical record review the presence of the chart reminder was noted.
The mailed educational materials included multiple items: (1) the American Cancer Society monograph and a DVD,27,28 (2) the Centers for Disease Control's Screen for Life brochure,29 and (3) a magnet developed by the investigators to remind subjects about CRC screening.23 Educational materials were mailed sequentially to patients between April 2009 and May 2010. Randomizing patients within each office allowed office differences to be balanced.30
Fecal Immunochemical Tests
The Clearview ULTRA FOB FIT (Inverness, Waltham, MA) was chosen as the FOBT. It can be used in primary care offices without access to specialized pathology services. Simulation models indicate that an annual FIT is as effective as colonoscopy every 10 years for life-years gained.31 Subjects returned the FIT to the investigators, who processed them, and results were mailed to both the patient and physician.
Outcome Measures
The primary outcome was CRC screening by any method in the 15-month interval following the initial mailed invitation. The only preplanned secondary outcome was the specific method used: FOBT (3-card FOBT), FIT, barium enema, flexible sigmoidoscopy, and/or colonoscopy. The outcomes were determined by trained medical record reviewers who were blinded to the intervention.
Statistical Methods
The analysis was based on the intention-to-treat principle and included all randomized participants. Subjects in the 4 groups were compared with respect to baseline demographics, attitudinal variables related to CRC screening, and medical record review variables using standard descriptive statistics. The Pearson χ2 test was used to compare discrete outcomes. One-way analysis of variance was used to compare continuous variables. Wilcoxon rank-sum tests were used for ordinal variables and continuous variables that did not follow a normal distribution. Subjects whose charts could not be found were considered not screened. For the questions about screening barriers, an average score was calculated by summing the individual scores and dividing by the number of questions answered. Odds ratios were calculated for differences in screening rates between the intervention groups and the usual care group. The SAS Glimmix procedure was used to account for the correlation of subjects within practices. We adjusted for prespecified patient characteristics such as age, sex, educational level, insurance status, family history of CRC, physician recommendation for CRC screening, importance of CRC screening, and average barrier score at baseline. The practice effects were specified as the random intercepts in the model. All analyses were performed using SAS version 9.2 (SAS, Inc., Cary, NC).
Role of the Funding Source
Peer reviewers for the American Cancer Society provided input on study design during the grant proposal review process. The funders had no role in data collection, analysis, or interpretation of data or in writing the report or the decision to submit the manuscript for publication.
Results
Figure 1 diagrams the study flow. Baseline questionnaires were returned by 2008 individuals (24%). Of those who returned questionnaires, 838 (42%) were due for CRC screening based self-report. However, 88 did not return a signed informed consent document and 7 were ineligible for other reasons. Thus, a total of 743 participants (89%) were enrolled in the study.
The baseline characteristics of the study population (n=743) are presented in Table 1. There were no significant differences in any characteristics across the 4 groups. The mean age was 61.1 years; 386 (52%) were women, 733 (99%) were white, 273 (37%) had a high school education or less, and 51 (7%) had no insurance.
Table 2 summarizes the medical record review for the 4 groups. There were no significant differences in clinical measurements across the 4 groups. The mean body mass index was 30.9 (standard deviation, 6.8). There were 541 (73%) who had at least one office visit during the follow-up interval. Lipid tests were completed by 491 (66%) in the past 5 years. Among women, 180 of 386 (47%) had a mammogram and 17 of 88 (19%) of those who were 65 years older had a bone density test in the past 26 months. Among men, 155 of 357 (43%) had a prostate-specific antigen test completed in the past 26 months.
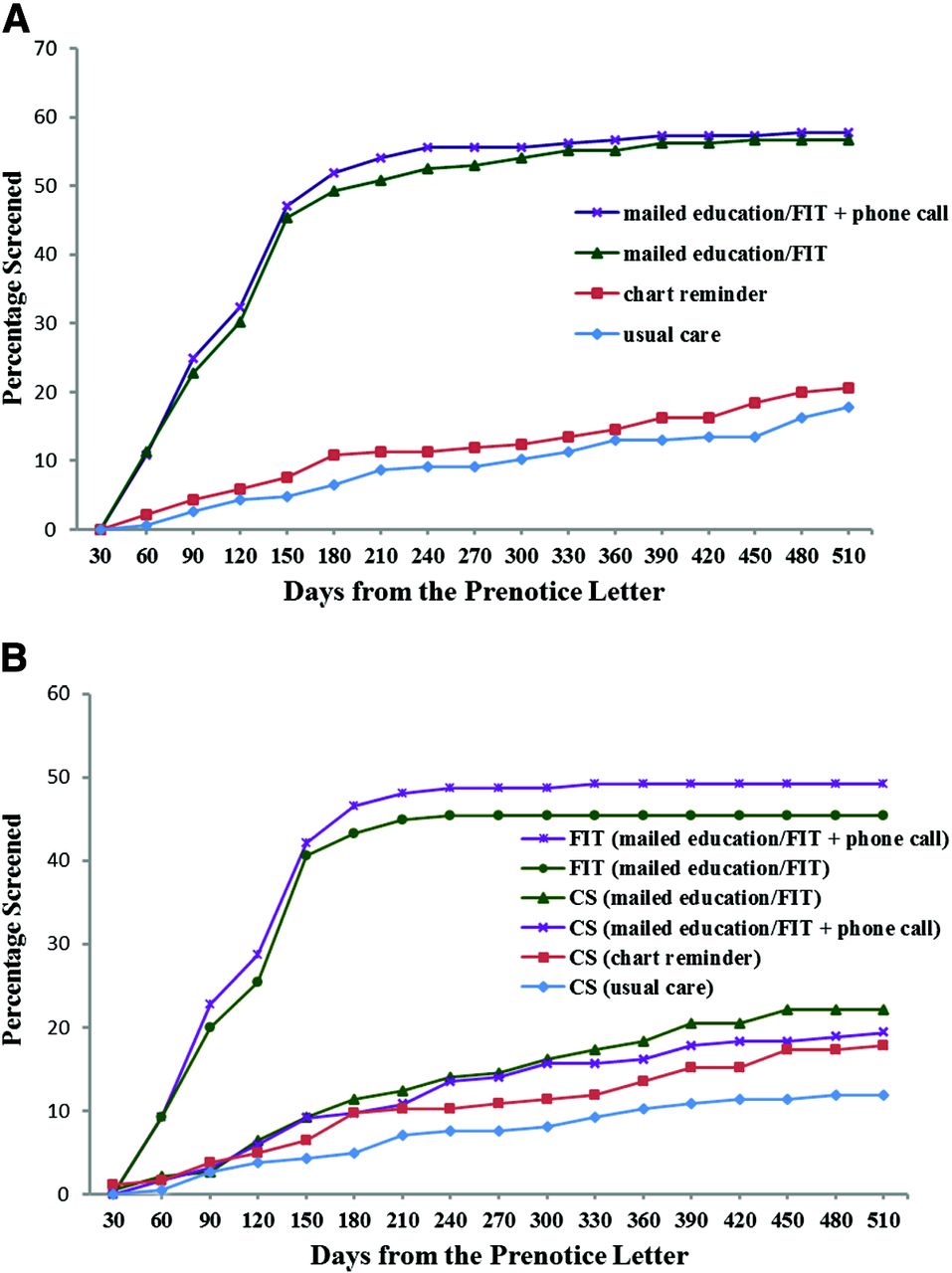
Table 3 summarizes the comparisons of the primary and secondary outcomes. For the primary outcome of any CRC tests completed, there was no significant difference between the chart reminder (38 of 185 patients; 20.5%) and usual care group (33 of 185 patients; 17.8%). The CRC screening rate in the mailed education/FIT group was 105 of 186 patients (56.5%), and in the mailed education/FIT plus phone call group was 107 of 187 patients (57.2%) (P < .0001 for each comparison when compared with usual care). Compared with usual care, the odds of being screened were significantly higher in both groups that received mailed education (mailed education/FIT: odds ratio [OR], 6.0; 95% confidence interval [CI], 3.7–9.6; and mailed education/FIT plus phone call: OR, 6.2; 95% CI, 3.8–9.9). When comparing practices using electronic reminders versus paper reminders, there was no difference in the main outcome of any CRC screening. Figure 4A shows the cumulative screening rates over time in the 4 groups. Figure 4B shows the cumulative rates of FIT or colonoscopy in each group. FIT screening was the major contributor to screening in the 2 mailed education groups.

A: Cumulative percentage screened with any method by study group. B: Cumulative percentage screened with fecal immunochemical test (FIT) or colonoscopy (CS) by study group.
Rates of colonoscopy were significantly higher than usual care in each of the 2 groups that received mailed education (22% vs 11.9%; P=.009 for mailed education/FIT vs usual care and 19.3% vs 11.9%; P=.050 for the mailed education/FIT plus phone call vs usual care). Although the 17.8% colonoscopy rate in the chart reminder group was higher than that in the usual care group, this difference did not reach statistical significance (P=.108).
Table 4 compares the intervention effects while controlling for prespecified covariables that might affect screening. The ORs for the 2 groups that received mailed education were significant and nearly identical to those found in the unadjusted analyses. Other covariables associated with CRC screening were doctor recommendation of CRC screening (as reported on the baseline questionnaire; OR, 1.7; 95% CI, 1.2–2.4), greater patient-perceived importance of CRC screening (OR, 1.8 [scores of 8–10 vs 1–7]); 95% CI, 1.2–2.5), and having a physical examination during the follow-up period (yes vs no; OR, 1.5; 95% CI, 1.03–2.1).
Discussion
In this randomized controlled trial, compared with usual care, we found that the overall CRC screening rates by any method increased significantly in the 2 groups that received nontailored, mailed patient education that included a FIT. Screening rates increased for both FIT and colonoscopy in these 2 groups, but FIT was the major contributor to screening. In addition, rates of colonoscopy increased in all groups compared with usual care but increased significantly only in the 2 groups that received mailed education. Physician chart reminders alone did not result in a statistically significant increase in overall screening or in colonoscopy. An additional telephone reminder designed to educate the patient, assess barriers, and move the patients along the stages of change toward screening32 had no beneficial effect over mailed education alone.
The effect of physician chart reminders has varied in other studies. We searched PubMed citations dated March 1987 through August 2012 that were limited to English language. Using the terms randomized trial and chart reminder and found 3 articles that assessed chart reminders to improve CRC screening.33⇓–35 In one of these studies, the use of office support systems, including chart reminders, increased the odds of completing mammography and FOBTs,33 whereas in another study, use of a Comprehensive Annotated Reminder Tool did not increase FOBT but did increase many other services targeted by the tool.34 Physician chart reminders did not improve CRC screening in another study of more than 20,000 patients.35 Two recent Cochrane reviews of physician chart reminders have shown minimal to moderate effects.36,37 Computer reminders achieved an improvement of 3.8% (interquartile range [IQR], 0.4–16.3%) for ordering tests.36 Our chart reminder increased colonoscopy testing by 5.9% over usual care (not significant), which is similar to the median improvement in the review by Shojania et al,36 but did not improve overall rates of CRC screening. Implementing reminders alone improved care by 11.2% (IQR, 6.5–19.6%); implementing reminders in addition to another intervention led to improved rates of 4% (IQR, 3–6%).37 Providing an explanation of the content on the reminder seemed to improve the effect (median, 12.0% for explanation vs 4.2% for no explanation).37 Our reminders provided a concise explanation of the need for CRC screening in asymptomatic individuals.
In contrast to many studies, our study included a usual care control group and a detailed medical record review to ascertain all CRC screening completed by patients. Nontailored existing educational materials from reputable national organizations were used because we wanted to generalize our findings to a wide range of practice settings.28,29 These materials informed individuals about the 4 major accepted methods used to screen for CRC.7⇓–9 Our refrigerator magnet and invitational mailing emphasized that CRC can occur in the absence of symptoms. The 2 groups that received mailed education plus FIT had rates of CRC screening of more than 56% in the 15 months following the initial mailing, which was significantly greater than the usual care group.
In a model that controlled for prespecified potential confounding variables, the ORs for the mailed intervention were similar to the unadjusted odds ratios. The increase in CRC screening in the 2 groups receiving mailed education resulted from both an increase in colonoscopy and return of the mailed FIT, although return of the FIT contributed substantially to the high screening rates in these groups. The popularity of the FIT in this study likely resulted from the inclusion of this test in the mailed materials and the clear directions for completion, which allowed patients to complete this test in the privacy of their home and return it to the investigators without the need for a medical appointment. Other studies have been conducted using mailed FOBTs, but, in contrast to our study, these studies have not ascertained any CRC screening using medical record review.38⇓⇓–41 Studies conducted in the context of population-based screening programs in Great Britain or the Netherlands showed that FOBTs, educational materials, and a letter signed by the patient's physician resulted in screening rates ranging from 55% to 65%.42⇓–44 Randomized controlled trials in practices where a mailed FOBT was used gave rates of returned FOBTs of 27% to 48%,45 33% to 48%,38 29% to 36%,46 and 60%.47
Although the telephone call was designed to assess patient barriers and move patients through the stages of change,32 our telephone call did not increase screening rates. This finding contrasts with a study of minority and low-income women in New York City, where telephone support increased rates of Papanicolaou tests, mammography, and CRC testing.48 Another study tested various interventions to increase screening using FOBT and randomized patients to usual care, a standard mailed intervention, a tailored mailed intervention, or a tailored intervention plus telephone reminder.38 FOBT rates increased to 44% to 48% in all intervention groups but were not significantly different from each other, indicating that, similar to our study, the telephone call had no added effect.38
We found a few practice-based studies that assessed strategies similar to ours. One study included 21,860 patients from 14 ambulatory practices in the Harvard Vanguard Medical Associates system; the patients all were overdue for CRC screening and were randomized to mailed education with 3 guaiac FOBT cards versus no mailed education. The study found overall CRC screening rates in their intervention group at follow-up to be slightly lower than the rates we found (44% for mailed group vs 38% for the group that did not receive a mailing; P < .001).35 Similar to our study, these investigators found no effect of chart reminders to physicians and the main increase in screening was due to FOBT completion.35 Ling et al49 conducted a randomized controlled trial of 10 primary physician group practices affiliated with the University of Pittsburgh. Enhanced office and patient management led to CRC screening rates of more than 50% among patients who were due for screening, and a tailored letter made no difference.49 We provided substantial support to offices with our direct-to-patient mailed education and other reminders, with final screening rates above 56% in the 2 intervention groups that received mailed education plus a FIT.
Strengths of this study include the “real-world” setting of family physician practices that randomized patients who were due for screening. These patients attended one of 16 rural family physician practices, and medical record review was used as the gold standard, in contrast to other studies that relied on self-report40,41 or did not include a usual care group.49,50 By including a usual care control group, we were able to control for secular trends in screening during the study period. The wording in the cover letter to patients was designed to be easily understood, emphasize the recommendation for screening everyone older than age 50, and explain the need for screening even in the absence of symptoms. Letters were mailed on the practice letterhead and signed by all the physicians in the practice, which may have lent credibility to the information and indicated the support of the patient's personal physician. Given the increase in colonoscopy rates in the 2 groups that received mailed education, it seems that providing written information stimulated some individuals to receive a colonoscopy. The educational materials were not tailored, eliminating significant time and expense in developing a personalized tailored intervention for each participant and making this type of intervention more easily expanded to a broader population.
Study limitations include the limited geographic area (rural Iowa), the homogeneous nature of the patient population, the inability to know what part of the complex intervention and mailed materials were responsible for improved screening rates, the lack of information about how to incorporate the intervention from an economic perspective (who will pay for this intervention), and participation bias in that individuals with no interest in CRC screening would likely not agree to participate.
Because CRC screening is not controversial and saves lives,5⇓⇓⇓–9,⇓,31,51 future studies should attempt to conduct and evaluate interventions to improve CRC screening without receiving individual informed consent, similar to the approach used by Sequist et al,35 so a nonbiased sample can be obtained. This article supports the notion that providing offices with support for CRC screening leads to improved CRC screening rates.23,35,49,52⇓–54
Interpretation
It has been estimated that 50% to 80% of CRCs could be prevented with appropriate screening.1⇓⇓⇓⇓–6 Screening rates are lower in socioeconomically disadvantaged and rural populations.55⇓–57A physician chart reminder did not increase screening compared with usual care. Each of the groups receiving mailed, nontailored educational materials plus a FIT had final CRC screening rates of more than 56%, a statistically significant improvement over usual care. This increase was largely due to return of the FIT, but colonoscopy rates increased as well. Our mailed packet included many types of education and we are not able to separate which aspects of our bundled education packet worked. The telephone call added to mailed education did not improve screening rates, but more intensive telephone interventions did improve screening in other studies.
Organizations and practices seeking to improve screening rates should consider mailing nontailored, easily understood educational materials and postage-paid returnable FITs to patients who are due for CRC screening. Our health care system should provide coverage for CRC screening that includes appropriate follow-up testing.
Notes
This article was externally peer reviewed.
Funding: Support was provided by American Cancer Society Research Scholar grant targeted-08-148-01-CPPB (BTL) and the University of Iowa Department of Family Medicine.
BTL serves as the Iowa Academy of Family Physicians Endowed Chair for Rural Research.
Conflict of interest: none declared.
Trial registration: ClinicalTrials.gov identifier: NCT01477814.
- Received for publication January 18, 2013.
- Revision received May 2, 2013.
- Accepted for publication May 6, 2013.




{kind=link}
{kind=link}
{kind=link}
{kind=link}