
Article Figures & Data
Figures
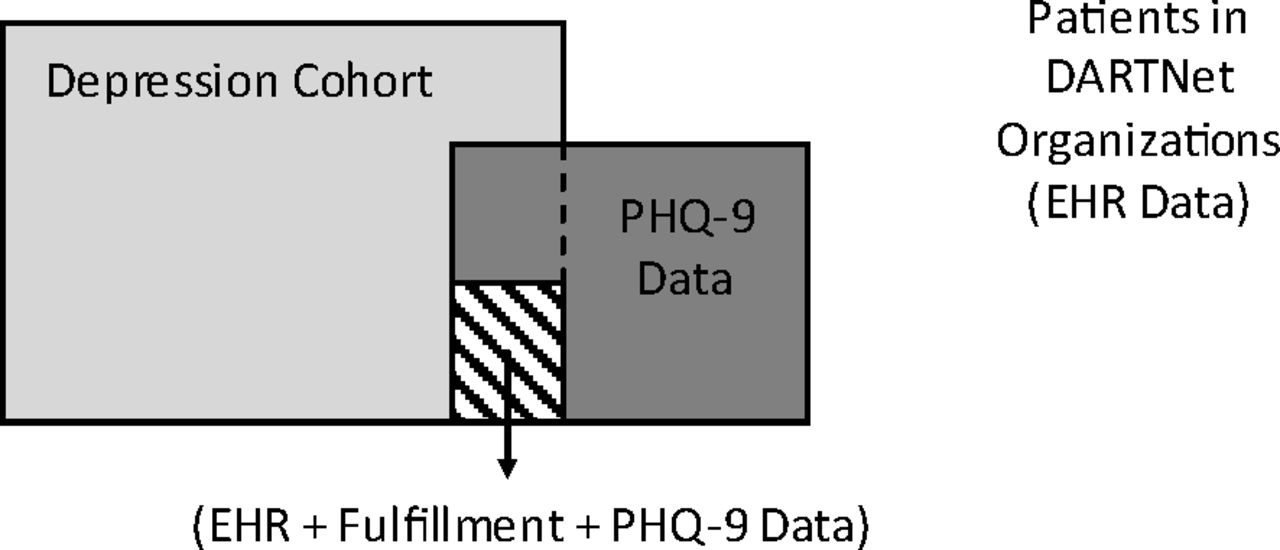
- Figure 1.
Conceptual diagram of the DARTNet population, data sources, and study cohorts. EHR, electronic health record; PHQ-9, 9-item Patient Health Questionnaire.
Tables
EHR EHR + Fulfillment EHR + Fulfillment + PHQ-9 Episodes, n 81,028 46,131 284 Subjects, n 61,464 37,416 259 Episodes per subject Mean 1.3 1.2 1.1 Median 1.0 1.0 1.0 Range 1–11 1–6 1–5 Demographic characteristics of episodes Age at start of episode (years) Mean 57.71 63.18 52.47 Median 59.00 67.00 53.00 Range 13–89 13–89 16–88 Age group Adolescent, 13–18 years 1649 (2.04) 472 (1.02) 7 (2.46) Adult, 19–64 years 44,208 (54.56) 19,197 (41.61) 192 (67.61) Older adult, ≥65 years 35,171 (43.41) 26,462 (57.36) 85 (29.93) Female sex 56,547 (69.79) 30,818 (66.81) 204 (71.83) Clinical characteristics of episodes Length of episode (days) Mean 655.53 701.03 759.47 Median 436.00 477.00 626.00 Primary diagnosis of episode* 296.2x 9305 (11.48) 5437 (11.79) 9 (3.17) 296.3x 7107 (8.77) 5528 (11.98) 7 (2.46) 300.4x 11,319 (13.97) 6922 (15.01) 22 (7.75) 311.x 53,297 (65.78) 28,244 (61.23) 246 (86.62) Episode severity† Unspecified 7819 (47.64) 5365 (48.93) 3 (18.75) Mild 2934 (17.88) 2436 (22.22) 4 (25.00) Moderate 3043 (18.54) 1394 (12.71) 5 (31.25) Severe without psychosis 539 (3.28) 378 (3.45) 1 (6.25) Severe with psychosis 225 (1.37) 200 (1.82) 0 (0.00) Severity missing 1852 (11.28) 1192 (10.87) 3 (18.75) Type of episode at start Index 60,361 (74.49) 37,222 (80.69) 258 (90.85) Recurrent 20,667 (25.51) 8909 (19.31) 26 (9.15) Episode end type Full 70 (0.09) 68 (0.15) 0 (0.00) Partial 72 (0.09) 47 (0.10) 0 (0.00) Continuation/unknown 80,886 (99.82) 46,016 (99.75) 284 (100.0) All data provided as n (%) unless otherwise indicated.
↵* Code from the International Classification of Diseases, Ninth Revision (ICD-9).
↵† Among ICD-9 codes 296.2 or 296.3; severity levels defined as 0–4 (no depression), 5–9 (minimal), 10–14 (mild), 15–19 (moderate), and 20–27 (major).21 Scores from item 9 (suicidality) of the 9-item Patient Health Questionnaire (PHQ-9) were characterized by raw scores indicating frequency of suicidal thoughts in the past 2 weeks: 0 (none), 1 (several days), 2 (more than half the days), or 3 (nearly every day).
EHR, electronic health record; PHQ-9, 9-item Patient Health Questionnaire.
- Table 2. Treatment Utilization Patterns during Antidepressant Exposure for Episodes Receiving an Antidepressant within 30 Days of Depression Diagnosis
EHR EHR + Fulfillment EHR + Fulfillment + PHQ-9 Episodes, n 81,028 46,131 284 Episodes receiving an AD within 30 days, n 17,385 (21.46) 996 (2.16) 23 (8.10) AD Utilization AD used to treat episode SSRI 12,697 (73.03) 750 (75.30) 17 (73.91) SNRI 2146 (12.34) 111 (11.14) 4 (17.39) TCA 393 (2.26) 29 (2.91) 0 (0.00) Buproprion 1581 (9.09) 52 (5.22) 0 (0.00) MAOI 5 (0.03) 0 (0.00) 0 (0.00) PP 316 (1.82) 16 (1.61) 1 (4.35) Tetracyclics 247 (1.42) 38 (3.82) 1 (4.35) Days to first AD Rx Mean 1.14 6.98 7.61 Median 0.00 2.00 0.00 Persistence* Mean 37.87 158.67 150.04 Median 30.00 91.00 90.00 Adherence† Mean 1.26 1.00 0.95 Median 1.00 1.00 1.00 Other psychotropic medications prescribed Anxiolytics 2243 (12.90) 290 (29.12) 4 (17.39) Antipsychotics 1806 (10.39) 77 (7.73) 4 (17.39) Stimulants 456 (2.62) 11 (1.10) 0 (0.00) Narcotic analgesics 311 (1.79) 40 (4.02) 0 (0.00) Data provided as n (%) unless otherwise indicated.
↵* Persistence: days between first and last prescription.
↵† Adherence: medication possession ratio.
AD, antidepressant; EHR, electronic health record; MAOI, monoamine oxidase inhibitor; PHQ-9, 9-item Patient Health Questionnaire; PP, phenylpiperazine antidepressant; Rx, prescription; SNRI, serotonin-noradrenergic reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant.
- Table 3. Nine-Item Patient Health Questionnaire (PHQ-9) Instruments Collected in DARTNet Practices
All DARTNet Patients Depression Cohort Depression Cohort + Fulfillment Data Available PHQ-9s collected, n 4900 1892 309 Patients with at least one PHQ-9, n 2969 1019 259 PHQ-9s collected per patient, n Mean 1.7 1.9 1.2 Median 1.0 1.0 1.0 Range 1–32 1–32 1–5 Age at time of first PHQ-9 (years) Mean 49.1 51.1 53.2 Median 49.0 51.0 54.0 Range 1–89 15–89 16–89 Age group Adolescent (13–18 years) 76 (2.56) 22 (2.16) 8 (3.09) Adult (≥19 years) 2768 (93.23) 997 (97.84) 251 (96.91) Female sex 2005 (67.53) 707 (69.38) 186 (71.81) PHQ-9 total score information Mean 8.9 9.1 9.2 Median 8.0 8.0 8.0 Range 0–27 0–27 0–27 Score ranges 0–4 (no depression) 1,448 (32.05) 544 (30.49) 67 (29.13) 5–9 (minimal) 1,215 (26.89) 517 (28.98) 63 (27.39) 10–14 (mild) 883 (19.54) 349 (19.56) 47 (20.43) 15–19 (moderate) 544 (12.04) 202 (11.32) 29 (12.61) 20–7 (severe) 428 (9.47) 172 (9.64) 24 (10.43) PHQ-9 item 9 (suicidality) information Score Mean 0.4 0.5 0.3 Median 0.0 0.0 0.0 Range 0–3 0–3 0–3 Specific scores 0 (no thoughts in past 2 weeks) 2,807 (69.43) 1,027 (63.71) 243 (81.00) 1 (thoughts on several days) 913 (22.58) 449 (27.85) 32 (10.67) 2 (thoughts on more than half the days) 201 (4.97) 92 (5.71) 18 (6.00) 3 (thoughts nearly every day) 122 (3.02) 44 (2.73) 7 (2.33) Data provided as n (%) unless otherwise indicated.
PHQ-9, 9-item Patient Health Questionnaire.
- Table 4. Baseline Severity of Illness and Suicidality Measurement Using the 9-Item Patient Health Questionnaire (PHQ-9) and Electronic Health Record Data among Depressed Patients in DARTNet Practices
Depression Cohort Depression Cohort + Fulfillment Data Available PHQ-9s collected, n 1440 192 Episodes with at least one PHQ-9, n 738 169 Patients with at least one PHQ-9, n 670 149 Baseline severity of illness measurement Episodes with a baseline PHQ-9,* n 135 22 Days between index depression diagnosis and closest PHQ-9, n Mean −8.9 −5.3 Median 0.0 0.0 Range −116 to 6 −116 to 5 Baseline PHQ-9s collected Before index diagnosis date (T−120 to T−1) 26 (19.26) 2 (9.09) On index diagnosis date 99 (73.33) 16 (72.73) After index diagnosis date (T+1 to T+7) 10 (7.41) 4 (18.18) Baseline severity of illness levels ICD-9 severity level Level 1 (mild) 8 (10.96) — Level 2 (moderate) 11 (15.07) — Level 3 (severe without psychosis) 0 (0.00) — Level 4 (severe with psychosis) 0 (0.00) — PHQ-9 severity level 0–4 (no depression) 25 (18.52) 0 (0.00) 5–9 (minimal) 39 (28.89) 5 (22.73) 10–14 (mild) 31 (22.96) 8 (36.36) 15–19 (moderate) 23 (17.04) 3 (13.64) 20–27 (severe) 17 (12.59) 6 (27.27) Baseline suicidality measurement ICD-9 suicidality Ideation 0 (0.00) 0 (0.00) Suicide attempt 0 (0.00) 0 (0.00) None 135 (100.0) 22 (100.0) PHQ-9 item 9 (suicidality) score Mean 0.4 0.6 Median 0.0 0.0 Range 0–3 0–3 Specific scores 0 (no thoughts in past 2 weeks) 76 (73.08) 14 (63.64) 1 (thoughts on several days) 20 (19.23) 4 (18.18) 2 (thoughts on more than half the days) 6 (5.77) 3 (13.64) 3 (thoughts nearly every day) 2 (1.92) 1 (4.55) Data provided as n (%) unless otherwise indicated.
↵* Baseline PHQ-9 was defined as the closest total PHQ-9 score within 120 days before and 7 days after the index depression diagnosis date.
ICD-9, International Classification of Diseases, Ninth Revision.
- Table 5. Depression Response and Suicidality Measurement Using 9-Item Patient Health Questionnaire (PHQ-9) and Electronic Health Records (EHR) Data among Depressed Patients in DARTNet Practices
Depression Cohort Depression Cohort + Fulfillment Data Available PHQ-9s collected, n 1,440 192 Episodes with at least one PHQ-9, n 738 169 Patients with at least one PHQ-9, n 670 149 Depression response measurement Episodes with a response PHQ-9, n 684 149 Response PHQ-9s per episode, n Mean 1.8 1.1 Median 1.0 1.0 Range 1–28 1–4 Days between index depression diagnosis and closest PHQ-9, n Mean 796.8 802.5 Median 545 630 Range 8–3327 2–2934 Response PHQ-9s collected after depression diagnosis (days) 7–60 107 (15.64) 17 (11.41) 61–90 19 (2.78) 1 (0.67) >90 558 (81.58) 131 (87.92) Depression response measurement ICD-9 severity level Level 5 (partial response) 1 (0.10%) 0 (0.00%) Level 6 (full/complete response) 1 (0.10%) 0 (0.00%) PHQ-9 severity level (lowest response) <10 (partial response) 464 (67.84%) 96 (64.43%) <5 (full/complete response) 272 (39.77%) 53 (35.57%) Days between baseline and lowest response PHQ-9 Mean 71.1 42.0 Median 37.0 42.0 Range 10–378 29–55 Change in PHQ-9 scores (baseline to lowest) Mean 5.1 3.0 Median 3.0 3.0 Range −3 to 19 1–5 Ranges of change −5 to −1 point 8 (9.88%) 0 (0.00%) 0–5 points 42 (51.85%) 2 (100.0%) 6–10 points 14 (17.28%) 0 (0.00%) >10 points 17 (20.99%) 0 (0.00%) ≥50% 45 (55.56%) 0 (0.00%) Baseline ≥10 and response <10 29 (35.80%) 2 (100.0%) Emergent suicidality measurement ICD-9 suicidality Ideation 2 (0.29%) 1 (0.67%) Suicide attempt 1 (0.15%) 1 (0.67%) None 681 (99.56%) 147 (98.66%) PHQ-9 item 9 (suicidality) Mean 0.6 0.2 Median 0.0 0.0 Range 0–3 0–3 Specific scores 0 (no thoughts in past 2 weeks) 317 (53.01%) 124 (84.35%) 1 (thoughts on several days) 212 (35.45%) 14 (9.52%) 2 (thoughts on more than half the days) 48 (8.03%) 5 (3.40%) 3 (thoughts nearly every day) 21 (3.51%) 4 (2.72%) Emergence vs. resolution of suicidality (for episodes with baseline and response PHQ-9 item 9) Episodes Episodes with baseline suicidality = 0 and emergent suicidality >0 10 (16.67) 0 (0.00) Episodes with baseline suicidality >0 and emergent suicidality = 0 8 (13.33) 0 (0.00) Data provided as n (%) unless otherwise indicated.
ICD-9, International Classification of Diseases, Ninth Revision.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Requirements and access needs of patients with chronic disease to their hospital electronic health record: results of a cross-sectional questionnaire survey
- Time to Remission for Depression with Collaborative Care Management (CCM) in Primary Care
- Monitoring Suicidal Patients in Primary Care Using Electronic Health Records
- Primary Care Research Conducted in Networks: Getting Down to Business