
Article Figures & Data
Figures
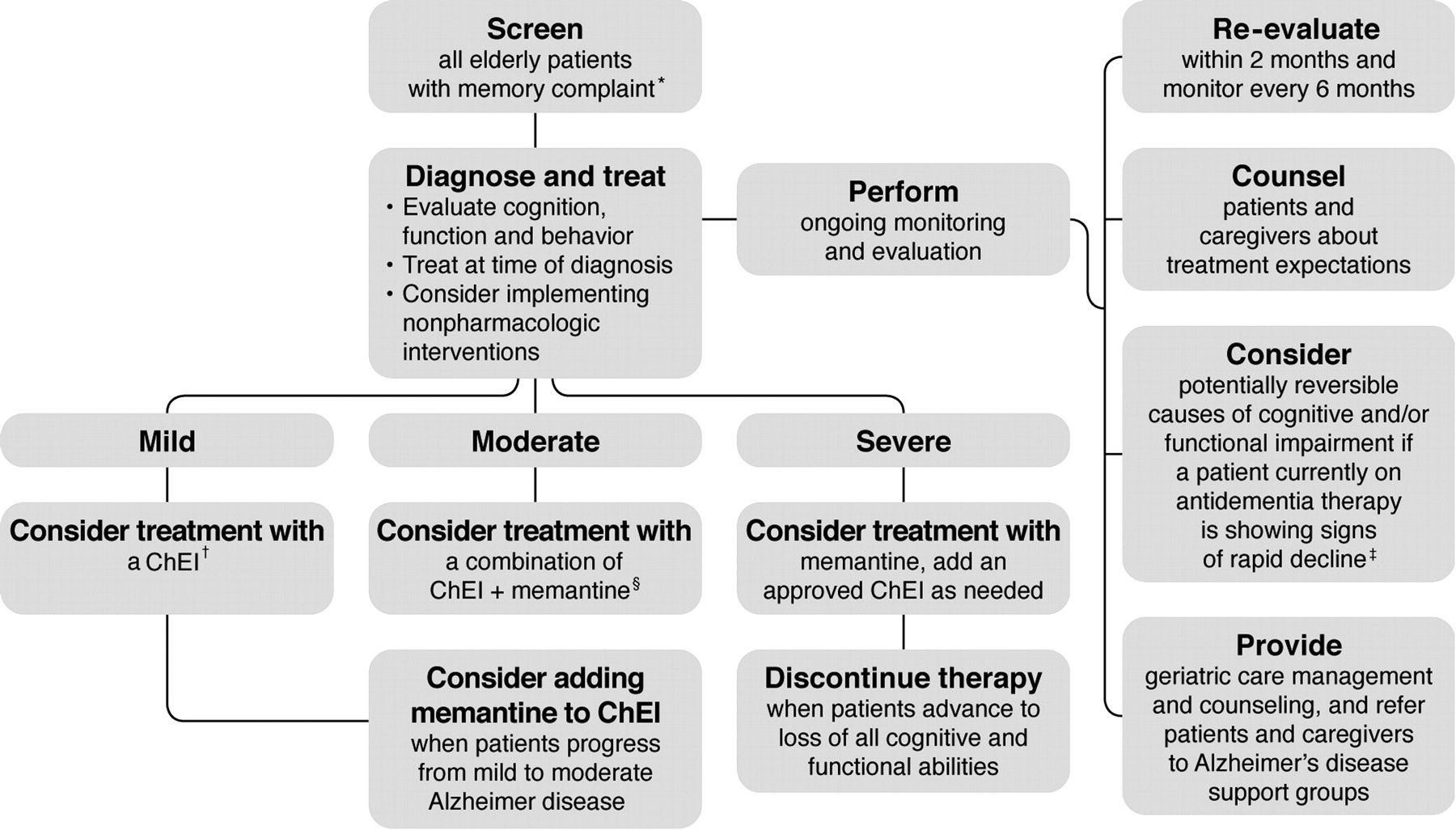
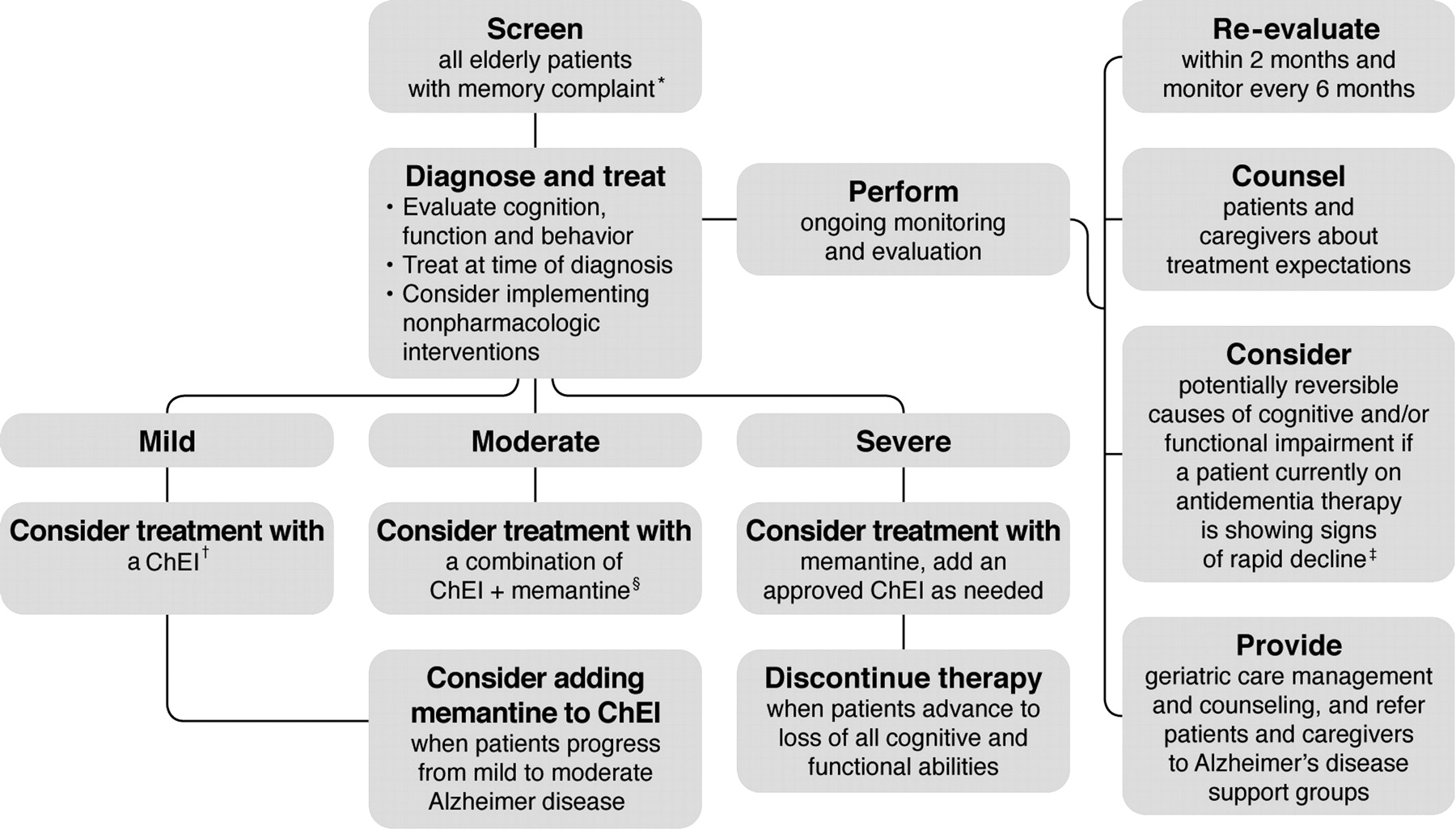
- Figure 1.
Treatment and management of Alzheimer disease. *Memory complaint may be raised by family or caregiver. All patients aged ≥75 years should be screened regardless of clinical presentation. †Cholinesterase inhibitors (ChEIs) are included for mild to moderate Alzheimer disease, excluding donepezil, which is indicated for mild, moderate, and severe Alzheimer disease. ‡Possible causes include medical comorbidities, the effects of other drugs, behavioral disturbances, or delirium. §Memantine is indicated for the treatment of moderate to severe Alzheimer disease. (This treatment algorithm is derived from recommendations published in Ref. 56. Reproduced with permission from RG Stefanacci. Reinforcing the value of combination therapy to treat moderate to severe alzheimer's disease. Phys Week 2009;26(9). © 2009 Physician's Weekly, LLC.)
Tables
- Table 1. Cholinesterase Inhibitors and Memantine for the Treatment of Cognitive Deficits in Patients with Alzheimer Disease (AD)6,59
Drug Approved Indication Suggested Dosage Side Effects Additional Notes/Caution Cholinesterase inhibitors Donepezil (Aricept) Mild to moderate AD Once daily, beginning with 5 mg/day, which can be increased to 10 mg/day (maximum dosage) after 4 weeks AEs are mild and include nausea, vomiting, and diarrhea Gastrointestinal-related AEs can be reduced if medication taken with food
Some patients exhibit an initial increase in agitation, which subsides after first few weeks of therapySevere AD Rivastigmine (Exelon) Mild to moderate AD Oral: Twice daily, beginning with 1.5 mg
Transdermal patch: Once daily, 4.6 or 9.5 mg
The target dose is 9.5 mg/24 hr per patch (a 10 cm2 patch) and requires a simple one-step dose titration to the therapeutic dose
There is a higher-dose patch (20 cm2) available, delivering 17.4 mg/24 hr; however, it is currently an unapproved treatment in the United States. Lack of approval was based on it having similar efficacy to the 10 cm2 patch, but with a tolerability profile comparable to that of the capsule formulationAEs include nausea, vomiting, diarrhea, weight loss, headaches, abdominal pain, fatigue, anxiety, and agitation
Gastrointestinal-related AEs are less prominent with the patch: the 9.5 mg/24 hr patch provides efficacy similar to that of the highest dose of capsules, with 3 times fewer reports of nausea and vomitingHigher dosages are more efficacious than lower dosages
No laboratory monitoring is requiredGalantamine (Razadyne) Mild to moderate AD Twice daily, beginning with 4 mg
After 4 weeks, dosage is increased to 8 mg twice daily
An increase to 12 mg twice daily can be considered on an individual basis after assessment of clinical benefit and tolerability
Also available in an extended-release formulation that can be taken once dailyMost common side effects are nausea, vomiting, and diarrhea Gastrointestinal-related AEs can be minimized by titrating the dosage gradually and taking the medication with meals NMDA antagonist Memantine (Namenda) Moderate to severe AD Twice daily, beginning with 5 mg, increasing the dose to 10 mg twice daily over 3 weeks AEs include fatigue, pain, hypertension, headache, constipation, vomiting, back pain, somnolence, dizziness Moderate to severe AD may respond better with memantine/donepezil combination versus donepezil alone AE, adverse event; NMDA, N-methyl D-aspartate.
- Table 2. Nonpharmacologic Interventions for Reducing Behavioral Disturbances in Alzheimer Disease (AD)6,95
Symptom Response Indecisiveness Reduce choices
Disorientation Provide the patient with a predictable routine (eg, exercise, meals, and bedtime should be routine and punctual)
Avoid relocation; if necessary bring familiar items
Allow the patient to dress in his or her own clothing and keep possessions
Use calendars, clocks, labels, and newspapers for orientation to time
Use color-coded or graphic labels (eg, on closets, table service, drawers) as cues for orientation in the home environment
Hallucinations Do not be overly concerned if they are not distressing to the patient
Consider antipsychotic agents where necessary, but fully inform family and caregivers of the risks/benefits of these medications
Delusions Redirect and distract the patient
Consider using antipsychotic medications
Repetitiveness Answer decisively, then distract
Lack of motivation Ensure tasks are simple so that the patient can complete them; break up complex tasks into smaller steps
Before performing all procedures and activities, explain them to the patient in simple language
Wandering (usually occurs later in the disease, ie, moderate to severe AD) Register the patient in the Alzheimer's Association Safe Return Program
Secure the environment with complex handles
Equip doors and gates with safety locks
Inform neighbors
Agitation Use distraction and redirection of activities to divert the patient from problematic situations
Reduce excess stimulation and outings to crowded places (overexposure to environmental stimuli can lead to agitation and disorientation)
Use lighting to reduce confusion and restlessness at night
Avoid glare from windows and mirrors, noise from a television, and household clutter
Accident-prone Provide a safe environment (eg, no sharp-edged furniture, no slippery floors or throw rugs, no obtrusive electrical cords)
Install grab bars by the toilet and in the shower
Ensure that comorbid conditions are optimally treated Consider using a day care program for patients with AD Antipsychotic drugs Atypical antipsychotic agents Recommended uses: control of problematic delusions, hallucinations, severe psychomotor agitation, and combativeness General cautions: diminished risk of developing extrapyramidal symptoms and tardive dyskinesia compared with typical antipsychotic agents Warning: atypical antipsychotic agents can cause an increased risk of cerebrovascular events (including stroke) in elderly patients with dementia-related psychosis Risperidone (Risperdal) Initial dosage: 0.25 mg/day at bedtime; maximum dosage: 2–3 mg/day, usually twice daily in divided doses Comments: current research supports use of low dosages; extrapyramidal symptoms may occur at 2 mg/day Olanzapine (Zyprexa) Initial dosage: 2.5 mg/day at bedtime; maximum dosage: 10 mg/day, usually twice daily in divided doses Comments: generally well tolerated Quetiapine (Seroquel) Initial dosage: 12.5 mg twice daily; maximum dosage: 200 mg twice daily Comments: more sedating; beware of transient orthostasis Typical antipsychotic agents Recommended uses: control of problematic delusions, hallucinations, severe psychomotor agitation, and combativeness; second-line therapy for patients who cannot tolerate or who do not respond to atypical antipsychotic agents General cautions: current research suggests that these drugs be avoided if possible because they are associated with significant, often severe side effects involving the cholinergic, cardiovascular, and extrapyramidal systems; there is also an inherent risk of irreversible tardive dyskinesia, which can develop in 50% of elderly patients after continuous use of typical antipsychotic agents for 2 years Warning: typical antipsychotic agents can cause an increased risk of cerebrovascular events (including stroke) in elderly patients with dementia-related psychosis Haloperidol (Haldol), fluphenazine (Prolixin), thiothixene (Navane) Dosage: varies by agent Comments: anticipated extrapyramidal symptoms; if these symptoms occur, decrease dosage or switch to another agent; avoid use of benztropine (Cogentin) or trihexyphenidyl (Artane) Trifluoperazine (Stelazine), molindone (Moban), perfenazine (Trilafon), loxapine (Loxitane) Dosage: varies by agent Comments: agents with “in-between” side-effect profile Mood-stabilizing (anti-agitation) drugs Recommended uses: control of problematic delusions, hallucinations, severe psychomotor agitation, and combativeness; useful alternatives to antipsychotic agents for control of severe agitated, repetitive, and combative behaviors General cautions: see comments about specific agents Trazodone (Desyrel) Initial dosage: 25 mg/day; maximum dosage: 200 to 400 mg/day in divided doses Comments: use with caution in patients with premature ventricular contractions Carbamazepine (Tegretol) Initial dosage: 100 mg twice daily; titrate to therapeutic blood level (4–8 μg/mL) Comments: monitor complete blood cell count and liver enzyme levels regularly; carbamazepine has problematic side effects Divalproex sodium (Depakote) Initial dosage: 125 mg twice daily; titrate to therapeutic blood level (40–90 μg/mL) Comments: generally better tolerated than other mood stabilizers; monitor liver enzyme levels; monitor platelets, prothrombin time, and partial thromboplastin time as indicated Anxiolytic drugs Benzodiazepines Recommended uses: management of insomnia, anxiety and agitation General cautions: regular use can lead to tolerance, addiction, depression and cognitive impairment; paradoxic agitations occurs in about 10% of patients treated with benzodiazepines; infrequent, low doses of agents with a short half-life are least problematic Lorazepam (Ativan), oxazepam (Serax), temazepam (Restoril), zolpidem (Ambien), triazolam (Halcion) Dosage: varies by agent See general cautions Nonbenzodiazepines Buspirone (BuSpar) Initial dosage: 5 mg twice daily; maximum dosage: 20 mg 3 times daily Comments: useful only in patients with mild to moderate agitation; may take 2 to 4 weeks to become effective Antidepressant drugs Recommended uses: see comments on specific agents General cautions: selection of an antidepressant is usually based on previous treatment response, tolerance and the advantage of potential side effects (eg, sedation vs activation); a full therapeutic trial requires 4–8 weeks; as a rule, dosage is increased using increments of initial dose every 5–7 days until therapeutic benefits or significant side effects become apparent; after 9 months, dosage reduction is used to reassess the need to medicate; discontinuing an antidepressant over 10–14 days limits withdrawal symptoms. Note: patients with depression and psychosis require concomitant antipsychotic medications. Tricyclic antidepressant agents Desipramine (Norpramin) Initial dosage: 10–25 mg in the morning; maximum dosage: 150 mg in the morning Comments: tends to be activating (eg, reduces apathy); lower risk for cardiotoxic, hypotensive and anticholinergic effects; may cause tachycardia; blood levels may be helpful Nortriptyline (Pamelor) Initial dosage: 10 mg at bedtime; anticipated dosage range: 10–40 mg/day (given twice daily) Comments: tolerance profile is similar to that of desipramine, but nortriptyline tends to be more sedating; may be useful in patients with agitated depression and insomnia; therapeutic blood level “window” of 50–150 ng/mL (190–570 nmol/L) Heterocyclic and noncyclic antidepressant agents Nefazodone (Serzone) Initial dosage: 50 mg twice daily; maximum dosage: 150–300 mg twice daily Comments: effective, especially in patients with associated anxiety; reduced dose of coadministered alprazolam (Xanax) or triazolam by 50%; monitor for hepatotoxicity Buproprion (Wellbutrin) Initial dosage: 37.5 mg every morning, then increase by 37.5 mg every 3 days; maximum dosage: 150 mg twice daily Comments: activating; possible rapid improvement of energy level; should not be used in agitated patients and those with seizure disorders; to minimize risk of insomnia, give second dose before 3pm Mirtazapine (Remeron) Initial dosage: 7.5 mg at bedtime; maximum dosage: 30 mg at bedtime Comments: potent and well tolerated; promotes sleep, appetite, and weight gain SSRIs Recommended uses: may prolong half-life of other drugs by inhibiting various cytochrome P450 isoenzymes General cautions: typical side effects include sweating, tremors, nervousness, insomnia or somnolence, dizziness, and various gastrointestinal and sexual disturbances Fluoxetine (Prozac) Initial dosage: 10 mg every other morning; maximum dosage: 20 mg every morning Comments: activating, very long half-life; side effects may not manifest for a few weeks Paroxetine (Paxil) Initial dosage: 10 mg/day; maximum dosage: 40 mg/day (morning or evening) Comments: less activating but more anticholinergic than other SSRIs Sertraline (Zoloft) Initial dosage: 25–50 mg/day; maximum dosage: 200 mg/day (morning or evening) Comments: well tolerated; compared with other SSRIs, sertraline has less effect on metabolism of other medications Citalopram (Celexa) Initial dosage: 10 mg/day; maximum dosage: 40 mg/day Comments: well tolerated; some patients experience nausea and sleep disturbances Fluvoxamine (Luvox) Initial dosage: 50 mg twice daily; maximum dosage: 150 mg twice daily Comments: exercise caution when using fluvoxamine with alprazolam or triazolam Reproduced with permission from Cummings JL, et al. Am Fam Physician 2002; 65:2525 to 2534. © 2002 American Academy of Family Physicians.6
SSRI, selective serotonin reuptake inhibitor.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Antidepressant and antipsychotic prescribing in primary care for people with dementia
- Brave New Psychiatry and the Idealization of Nonplaces: A Critical Discourse Analysis
- Antipsychotics for agitation in dementia
- Les antipsychotiques pour lagitation dans les cas de demence
- Management of non-cognitive symptoms associated with dementia
- Content Usage and the Most Frequently Read Articles by Issue in 2012
- Focus on Clinical Practice: Improving the Quality of Care