
Abstract
Background: Physician feelings of ineffectiveness and family-related barriers hamper childhood obesity discussions. Physicians desire appealing, time-efficient tools to frame and sensitively address obesity, body mass index, physical activity, nutrition, and portion size. Our university design-led coalition codeveloped tools and games for this purpose.
Methods: In this feasibility study, we evaluated physician-level counseling of 9- to 12-year-old children and their parents/caretakers using Fitwits MD (Carnegie Mellon University School of Design, Pittsburgh, PA), a brief, structured intervention with flashcards and take-home games. Residency-based physicians in three low- to mid-level socioeconomic urban offices provided self-report data over 8 months through surveys, comment cards, and interviews.
Results: We recruited 33 physicians and 93 preadolescents and families. Child-centered key messages resulted in 7-minute conversations, on average. For those physicians who used Fitwits MD, 96% felt improved comfort and competence and 78% noted barrier reduction.
Conclusions: Fitwits MD improved residency-based physician self-efficacy and emphasized important health education topics regarding office-based childhood obesity discussions with preadolescents and parents/caretakers.
Though the health dilemma of excess weight is widely known, not all physicians and families discuss childhood obesity in a forthright, understandable way. Many physicians perceive the following as barriers: time pressure; insufficient training for nutrition-based and body mass index (BMI) counseling; treatment futility; home and neighborhood environments that undermine recommendations; and insufficient reimbursement, support services, and patient educational materials. Clinicians under-utilize BMI. Often, families do not perceive that a problem exists and may not be motivated, have low literacy and numeracy skills, or have aversion to the term “obesity” and to perceived criticism of parenting skills.1–5 For these reasons, we co-developed counseling tools and games to communicate weight-related concerns and health guidance.
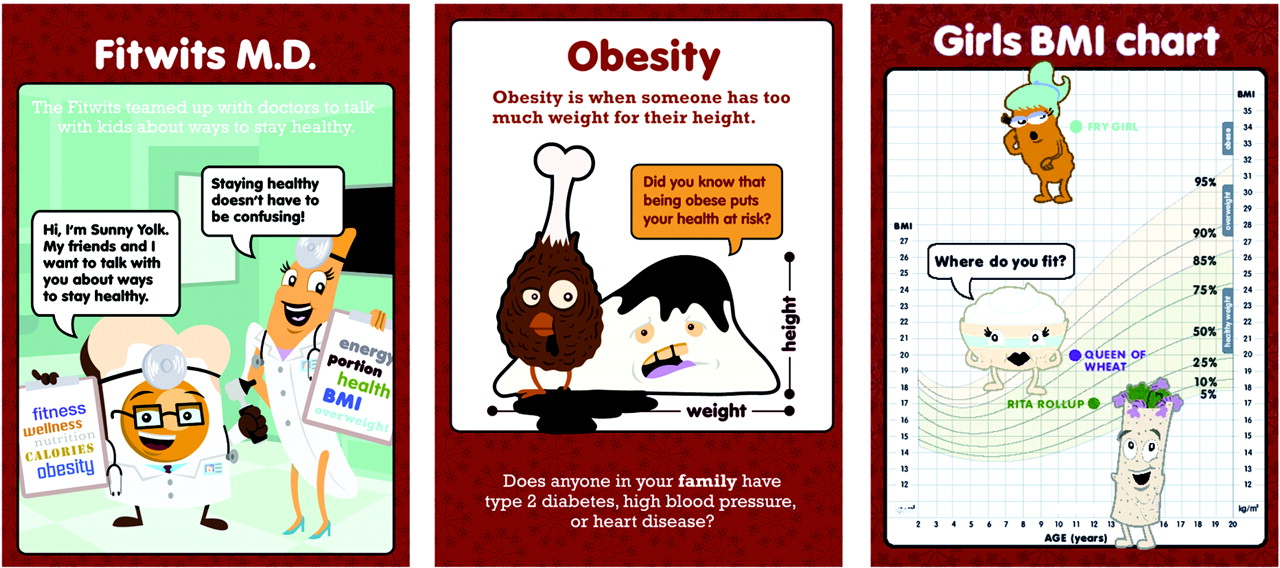
In June 2008, a Carnegie Mellon University design team led seven physicians and two registered dietitians through a participatory design workshop. The resulting Fitwits MD flashcards included a simple definition of obesity, BMI charts with Fitwits and Nitwits characters and color-coded ranges, and friendly interrogatives about personal and family history. Self-management cues include 60 minutes of daily exercise, foods and beverages containing large amounts of sugar and fat, healthy alternatives, and a hand-based portion guide (Figure 1; http://www.fitwits.org). In addition, we provided to families the Fitwits School take-home games.6

The Fitwits MD flashcards use simple visual representations with accompanying health terms. The cards use characters called the “Fitwits and Nitwits” to clarify body mass index charts, ask open-ended questions, and give self-management information.
Methods
Residency-based physicians in three western Pennsylvania low- to mid-level socioeconomic urban offices provided self-report data mid-November 2008 through July 2009. We recruited convenience samples of physicians, parents/caretakers, and 9- to 12-year-old children presenting for well child/minor illness visits, regardless of BMI. The Carnegie Mellon University and University of Pittsburgh institutional review boards approved all study procedures.
Fitwits team residents trained physicians using flashcards, best-evidence recommendations, and games practice in a 1-hour training session. Absent physicians were provided with one-on-one instruction. Participants were instructed to use Fitwits MD in lieu of traditional office discussions. We used a pre- and posttest observational design. Before training, physicians completed a 10-question survey with Likert-scale questions and comment areas concerning comfort and competence levels, patient health education, perceived discussion length, and physician barriers. Questions after the study period included percentage of intervention use; Likert scale change in comfort, competence, and barrier reduction; and perceived discussion length. Physicians completed open-ended comment cards after each office visit intervention. In-depth audio-recorded and transcribed interviews with randomly selected physicians provided additional qualitative data. The comment cards and interviews were analyzed by two evaluation team coders (DJA, IKJ). Quantitative data were analyzed using SPSS software, version 14.0 (SPSS Inc., Chicago, IL).
Results
Ninety-three families participated. Of 39 eligible physicians, 33 (13 in postgraduate year 2, 11 in postgraduate year 3, two fellows, and seven faculty) were recruited, 32 completed the study, and eight were interviewed. At baseline, almost all physicians reported that they discussed obesity prevention (93.8%), nutrition (87.9%), and exercise (97.0%); only 21.2% discussed portion size. More than half of physicians reported feeling somewhat to very comfortable (59.4%) and competent (62.6%). All physicians identified barriers, notably time (51.5%) and parent/child issues (54.7%).
After the intervention (Table 1), 40.7% of physicians used Fitwits MD at half or more visits, whereas 21.9% did not use it. Physicians who used Fitwits MD reported increased comfort (96.2%), enhanced competence (96.3%), and fewer barriers (77.7%). The average perceived discussion time doubled from 3.6 minutes before the intervention to 7.0 minutes using Fitwits MD. Interviewed physicians appreciated the nonjudgmental characters, visual cues, portion size demonstrations, bidirectional fun conversations, and the standardized intervention for all patients, not just obese children. Ninety-three comment cards indicated children's excitement about the games and that Fitwits MD facilitated discussion about fast food and soda consumption, family meals, activity levels, and screen (TV, video and computer) time.
Results of Postintervention Physician Survey Questions for Well Child Visits with 9- to 12-Year-Old Children (N = 32)
Discussion
Brief tools are needed to guide childhood obesity counseling.1,7 In this feasibility study, the Fitwits MD intervention improved residency-based physicians' comfort and competence levels and reduced barriers. Visual literacy, simplified health terms, child-centered messages, and take-home games encouraged physicians to invest in the health of patients ages 9 to 12 years, regardless of BMI. Three built-in components emphasized important health education topics: BMI charts, the term “obesity” simply defined, and hand-based portion sizes.3–6 Limitations included some differences in survey questions before and after the intervention, some bias from leading questions, sample size, lack of validity or reliability of measures, a control group, and data from experienced clinicians. Future research will address these limitations and assess health outcomes.
Acknowledgments
We thank Lindsey Detwiler Barton, RD, Megan McQuaide Montag, RD, Stephen A. Wilson, MD, MPH, and design and additional physician participants for help with developing the Fitwits tool; Fitwits office champion and resident teams: Laura Macbeth MPH, CHES, Melissa Williams, Rosia L Williams, RN, Stacey L. Brown, MD, Jill Haltigan, MD, Kristen A. Scopaz, MD, and Michelle N. Stalter, DO. Contributions to data analysis were provided by Chrissy A. Lopez. Amy Haugh, MLS, and Jennifer L. Middleton, MD, MPH, reviewed the manuscript, and Paula Preisach helped with manuscript preparation.
Notes
-
This article was externally peer reviewed.
-
Current affiliation: Thomas Jefferson University, School of Population Health, Philadelphia, PA (DJA); and Ambler Medical Associates, Ambler, PA (SKF).
-
Funding: This study was funded by The Heinz Endowments, the St. Margaret Foundation, and the Allegheny County Medical Society Foundation.
-
Conflict of interest: none declared.
- Received for publication November 18, 2010.
- Revision received March 15, 2011.
- Accepted for publication March 21, 2011.




{kind=link}