
Article Figures & Data
Figures
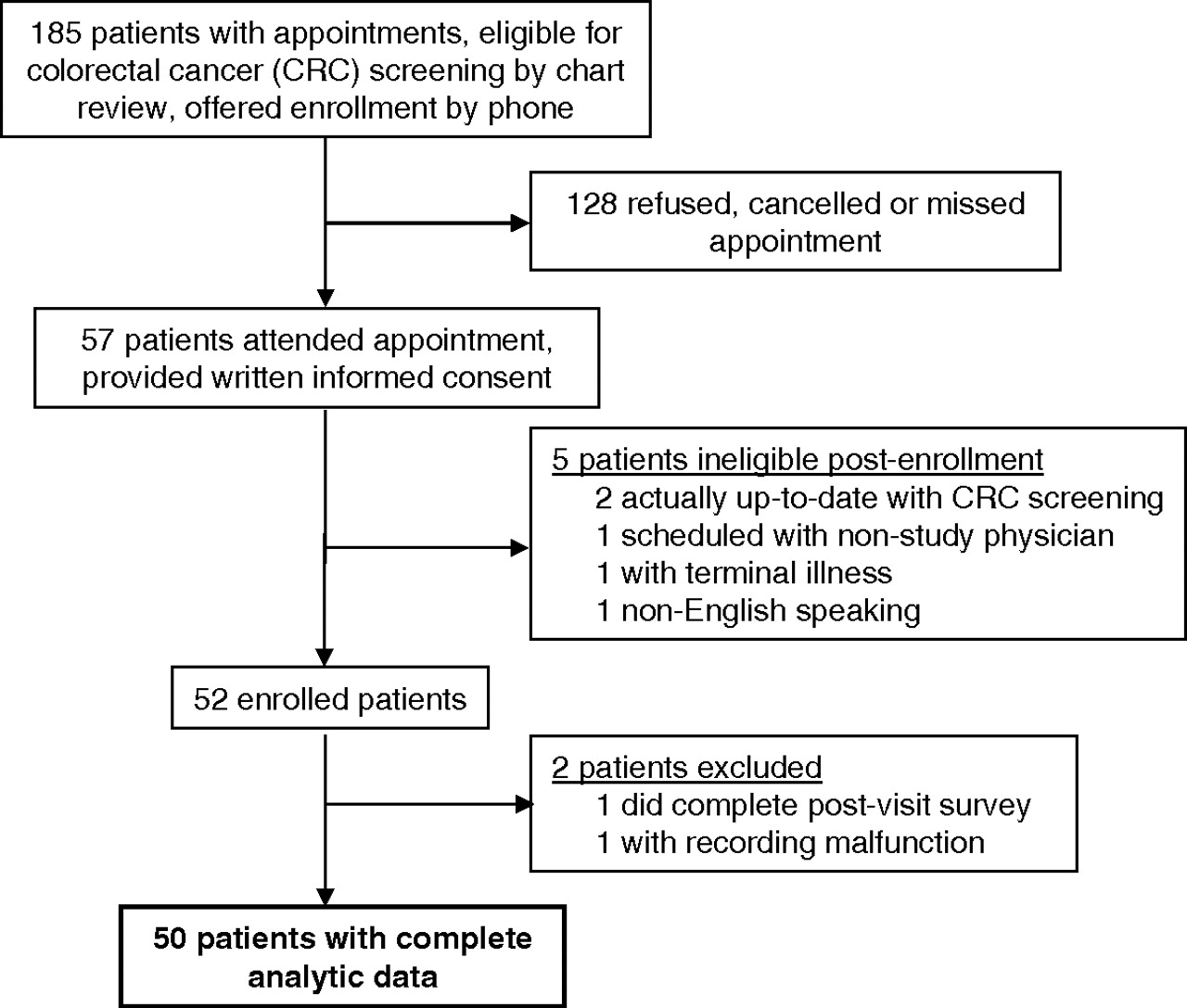
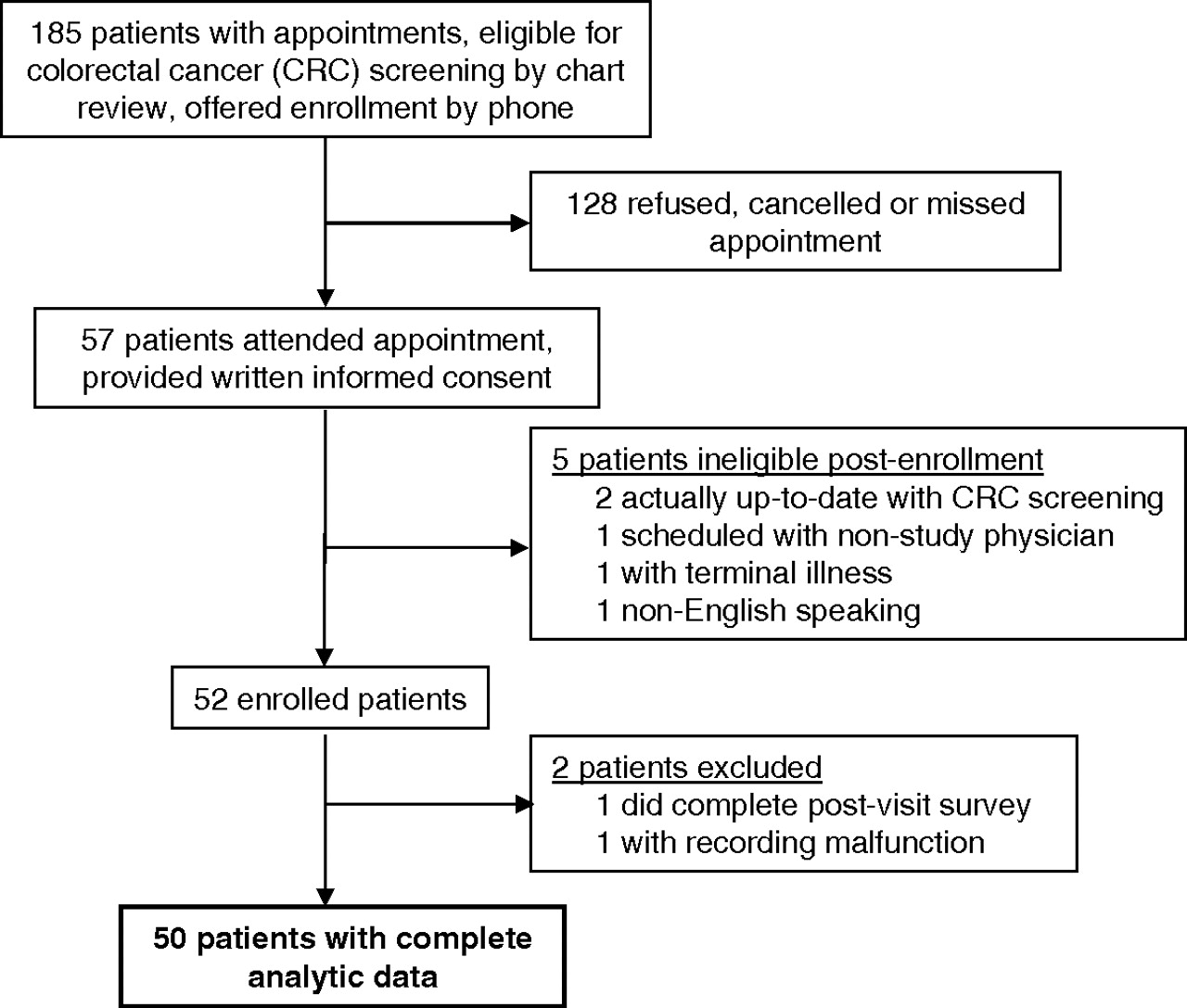
- Figure 1.
Flow of study patients.
Tables
Characteristic Age, years (mean [SD]) 57.3 (6.2) Female 66 (33) Race/ethnicity Non-Hispanic white 29 (58) African American 13 (26) Hispanic 5 (10) Other 3 (6) Education High school, GED, or less 8 (16) Some college (no degree) 24 (48) Graduated from college 18 (36) Household income ($) <20,000 12 (24) 20,00–49,999 7 (14) 50,000–84,999 16 (32) ≥85,000 12 (24) Missing 3 (6) Self-reported health status Poor 1 (2) Fair 14 (28) Good 20 (39) Very good 11 (22) Excellent 4 (8) Current smoker 18 (36) Baseline stage of readiness with regard to colonoscopy Precontemplation 10 (20) Contemplation 28 (56) Planning 12 (24) -
Values provided as n (%) unless otherwise indicated.
-
GED, general educational development.
-
Characteristic Who initiated CRC screening conversation Provider 27 (71) Patient 11 (29) Discussion of specific tests General discussion but no specific test mentioned 2 (5) Specific tests discussed 36 (95) Colonoscopy 36 (95) Flexible sigmoidoscopy 15 (39) Fecal occult blood testing 12 (32) CT colonography 2 (5) Discussion of behavioral constructs Benefits of screening 20 (53) Common patient-level barriers 11 (29) Patient's risk and susceptibility to CRC 14 (37) Patient self-efficacy to complete screening Provider explored patient's confidence 0 Provider referred to prior successful behaviors 0 Provider reframed prior failures 0 Provider specified next steps 7 (18) Providers expressed confidence in patient 0 One or more behavioral constructs 26 (68) Two or more behavioral constructs 17 (45) -
Values provided as n (%) unless otherwise indicated.
-
CRC, colorectal cancer; CT, computed tomography.
-
- Table 3.
Associations Between Conversation Content and Measures of Behavioral Constructs to Colorectal Cancer Screening After the Visit (n = 50)
Behavioral Construct (Sample SD of Scale Measure After Visit) β (95% CI)* (Adjusted Mean Difference) Perceived benefits (SD, 0.86) No discussion of CRC screening Ref Any discussion −0.02 (−0.35 to 0.31) No discussion of CRC screening Ref Screening discussed but not benefits −0.04 (−0.40 to 0.32) Benefits discussed 0.00 (−0.39 to 0.38) Perceived barriers† (SD, 0.63) No discussion of CRC screening Ref Any discussion 0.00 (−0.15 to 0.15) No discussion of CRC screening Ref Screening discussed but not barriers 0.04 (−0.12 to 0.21) Barriers discussed −0.11 (−0.32 to 0.10) Perceived risk/susceptibility (SD, 0.94) No discussion of CRC screening Ref Any discussion 0.39 (0.09–0.68) No discussion of CRC screening Ref Screening discussed but not risk/susceptibility 0.37 (0.04–0.70) Risk/susceptibility discussed 0.42 (0.13–0.72) Self-efficacy to undergo CRC screening (SD, 0.70) No discussion of CRC screening Ref Any discussion −0.06 (−0.42 to 0.29) No discussion of CRC screening Ref Screening discussed but not next steps −0.06 (−0.42 to 0.30) Next steps specified −0.08 (−0.52 to 0.37) Intention to undergo CRC screening (SD, 0.78) No discussion of CRC screening Ref Any discussion 0.42 (0.11–0.73) No discussion of CRC screening Ref Screening discussed but no constructs 0.44 (0.12–0.75) One or more constructs addressed 0.41 (0.05–0.77) -
↵* β coefficients estimate adjusted mean differences (vs reference category) in construct-specific after-visit scale scores using analysis of covariance models to adjust for measures of the relevant behavioral construct, health status (fair/poor vs. good/very good/excellent), and annual household income (<$50,000 vs. ≥$50,000) before the visit. Confidence intervals are corrected for within-physician clustering by use of robust standard errors.
-
↵† Higher numbers on the barriers scale indicate greater perceived barriers, so negative coefficients imply lower perceived barriers after versus before the visit.
-
CRC, colorectal cancer.
-
- Table 4.
Colorectal Cancer Screening Test Planning, Ordering, and Completion by Whether and How Providers Discussed Colorectal Cancer Screening
Outcome Overall CRC Screening Discussion P No Discussion Screening Discussed Without Addressing Behavioral Constructs One or More Constructs Addressed Advancement in stage of readiness to undergo CRC screening (N = 40)* 22/40 (55) 1/8 (13) 8/11 (73) 13/21 (62) .03 CRC screening ordered (N = 50) 31/50 (62) 0/12 (0) 9/12 (75) 22/26 (85) <.001 CRC completed (N = 50) 17/50 (33) 0/12 (0) 8/12 (67) 9/26 (35) .001 -
Values provide as n/N (%).
-
↵* Defined as more advanced stage of readiness with regard to a CRC screening test after the visit (compared with before the visit); the analysis for this outcome was restricted to the 40 patients who did not report on questionnaires before the visit that they were planning to undergo fecal occult blood testing and colonoscopy.
-
CRC, colorectal cancer.
-
- Table 5.
Adjusted Association between Provider Conversation and Advancement in Stage of Readiness and Colorectal Cancer Screening Completion
Independent Variable OR (95% CI)† Advancement in stage of readiness (n = 40*) No discussion of CRC screening 1.0 (ref) Any discussion of CRC screening 12.7 (1.3–682.0) No discussion of CRC screening 1.0 (ref) Screening discussed without addressing behavioral constructs 14.5 (1.04–986.6) One or more constructs addressed 11.0 (1.06–602.2) CRC screening completed (n = 50) No discussion of CRC screening 1.0 (ref) Any discussion of CRC screening 10.0 (1.4-∞) No discussion of CRC screening 1.0 (ref) Screening discussed without addressing behavioral constructs 33.2 (3.6-∞) One or more constructs addressed 5.8 (0.7-∞) -
↵* Analyses for this outcome was restricted to the 40 patients who did not report on questionnaires before the visit that they were planning to undergo fecal occult blood testing and colonoscopy during. Advancement in stage of readiness is defined as more advanced stage of readiness with regard to one of these tests post-visit as compared to pre-visit.
-
↵† Odds ratios were estimated using exact logistic regression and adjusted for health status (fair/poor vs good/very good/excellent), annual household income (<$50,000 vs ≥$50,000), and stages of readiness before the visit with regard to fecal occult blood testing and colonoscopy. The upper 95% CI may be unbounded in the setting of zero cells (i.e., when no patients completed CRC screening in the absence of CRC screening discussions).
-
CRC, colorectal cancer.
-




{kind=link}