
Article Figures & Data
Figures
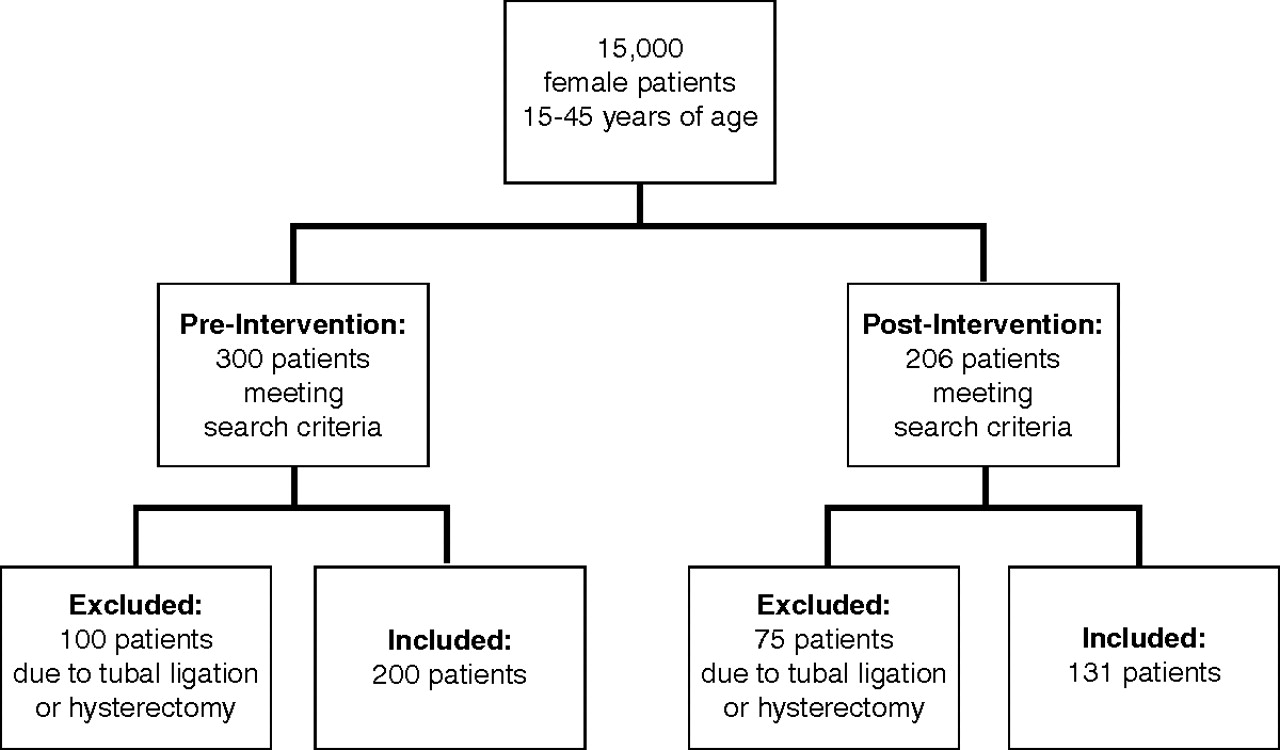
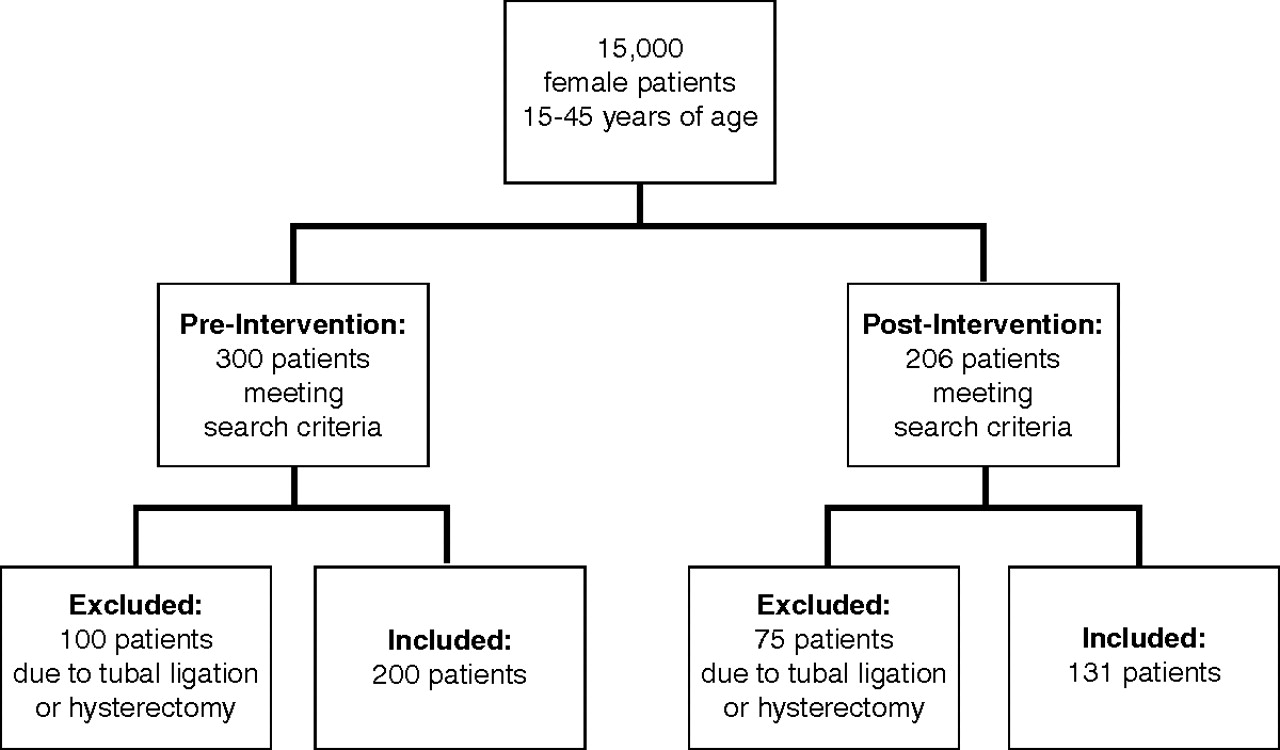
- Figure 1.
Patient inclusion and exclusion.
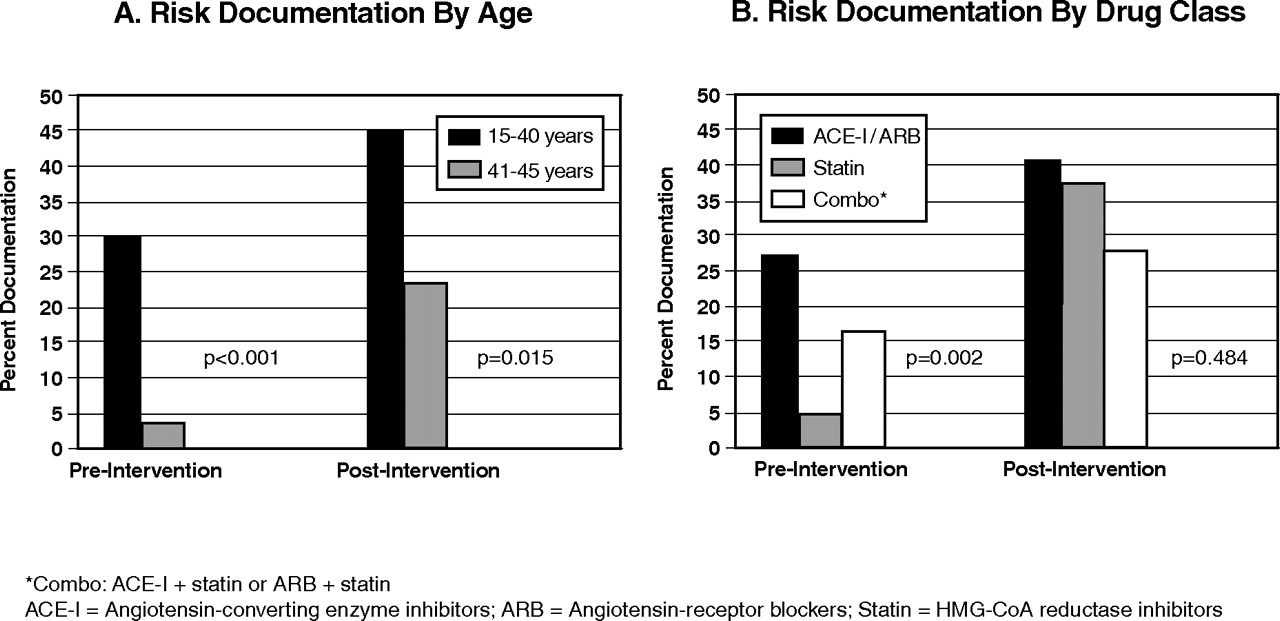
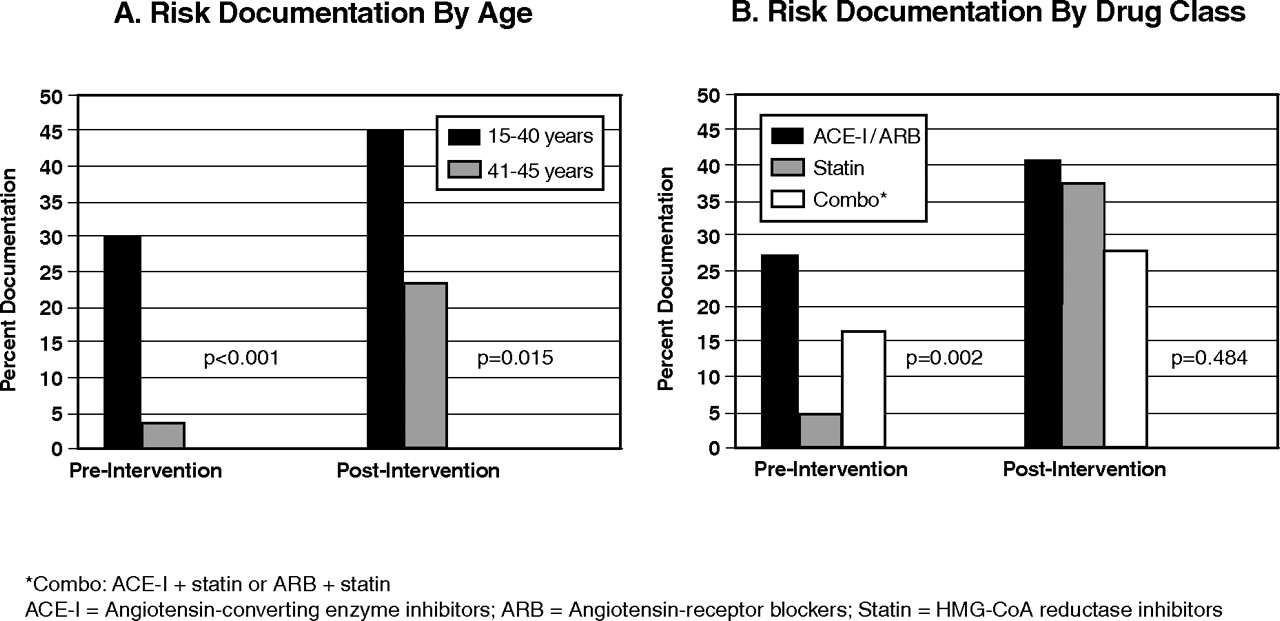
- Figure 2.
Patient characteristics affecting risk documentation.
Tables
FDA Pregnancy Category Definition A Controlled studies in women fail to demonstrate a risk to the fetus in the first trimester (and there is no evidence of a risk in later trimesters), and the possibility of fetal harm seems to be remote. B Either animal reproductive studies have not demonstrated a fetal risk but there are no controlled studies of pregnant women, or animal reproductive studies have shown adverse effect (other than a decrease in fertility) that was not confirmed in controlled studies in women in the first trimester (and there is no evidence of a risk during later trimesters). C Either studies in animals have revealed adverse effects on the fetus (teratogenic or embrocidal or other) and there are no controlled studies in women, or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus. D There is positive evidence of human fetal risk, but the benefits from use in pregnant women may be acceptable despite the risk (eg, if the drug is needed in a life-threatening situation or for a serious disease for which safer drugs cannot be used or are ineffective). X Studies in animals or human beings have demonstrated fetal abnormalities or there is evidence of fetal risk based on human experience or both, and the risk of the use of the drug in pregnant women clearly outweighs any possible benefit. The drug is contraindicated in women who are or may become pregnant. Survey Question Survey Response Correct response Before Intervention (n = 36) (n [%]) Correct response After Intervention (n = 38) (n [%]) P 1. Which pregnancy drug category are ACE-I and ARB in? a. A 15 (41.7) 22 (57.9) .176 b. B c. C* d. D* e. X f. I don’t know 2. Which pregnancy drug category is statin in? a. A 10 (27.8) 19 (50) <.065 b. B c. C d. D e. X* f. I don’t know 3. ACE-I and ARB primarily affect which fetal system if exposed during the second and third trimester? a. Lung 23 (63.9) 28 (73.7) .440 b. Cardiovascular c. Renal* d. Nervous e. I am unsure 4. There is increasing evidence that ACE-I/ARB have adverse effects to fetuses exposed during the first trimester. a. True* 19 (52.8) 33 (86.8) .650 b. False c. I am not sure 5. Statin has been shown to adversely affect fetal development in human studies. a. True 7 (19.4) 9 (23.7) .652 b. False* c. I am not sure 6. In the past several months have you prescribed an ACE-I, ARB, or statin to any women between the ages of 15 to 45? a. Yes† 8 (22.2) 10 (26.3) 1.000 b. No c. I’m not sure 7. When prescribing ACE-I, ARB, or statin, do you consider the possibility of the patients becoming pregnant while taking the drug? a. Yes, always† 24 (66.7) 31 (81.6) .678 b. Usually† c. Sometimes d. No, never 8. If you do consider possible pregnancy when prescribing ACE-I/ARB and statin, do you make an effort to document use of contraception and discussion of possible risks? a. Yes, always† 25 (69.4) 28 (73.7) .091 b. Usually† c. Sometimes d. No, never e. I don’t consider pregnancy risk when prescribing Physician Demographics 9. Gender a. Male 19 (52.85) 17 (44.7) .316 b. Female 17 (47.2) 21 (55.3) 10. Current year of residency training a. PGY-1 16 (44.4) 18 (47.4) .889 b. PGY-2 11 (30.6) 10 (26.3) c. PGY-3 8 (22.2) 9 (23.7) d. PGY-4 2 (5.6) 1 (2.6) 11. Current residency training program a. FM 13 (36.1) 12 (31.6) .770 b. IM 5 (13.9) 8 (21.1) c. FM/IM 5 (13.9) 3 (7.9) d. OB/GYN 9 (25.0) 8 (21.1) e. Transitional 3 (8.3) 7 (18.4) Characteristics Before Intervention (n = 200) (n [%]) After Intervention (n = 131) (n [%]) P Patient Age (years) .728 15 to 40 years old 124 (62.0) 84 (64.1) 41 to 45 years old 76 (38.0) 47 (35.9) Medication prescribed ACE-I 129 (64.5) 95 (72.5) .149 ARB 29 (14.5) 17 (13.0) .747 Statin 88 (44.0) 50 (38.2) .307 Disease state indication HTN 154 (77.0) 109 (83.2) .211 DM 88 (44.0) 62 (47.3) .574 HLD 90 (45.0) 56 (42.7) .735 Use of contraception* 44 (22.0) 38 (29.0) .154 Pregnancy test at prescription 5 (2.5) 4 (3.1) .744 Physician Resident training program .176 IM 102 (51.0) 59 (45.0) FM 54 (27.2) 37 (28.2) IM/FM combined program 7 (3.5) 9 (6.9) OB/GYN 5 (2.5) 0 (0) Faculty 32 (16.0) 26 (19.8) PGY of Training <.001 PGY1 0 (0) 15 (11.5) PGY2 38 (19) 39 (29.8) PGY3 60 (30.0) 43 (32.8) Graduate 2009 60 (30.0) 3 (2.3) Faculty 35 (17.5) 31 (23.7) Graduate 7 (3.5) 0 (0) ↵* Method of contraception not different between treatment groups.
ACE-I, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; statin, HMG-CoA reductase inhibitors; HTN, hypertension; DM, diabetes; HLD, hyperlipidemia; IM, Internal Medicine; FM, Family Medicine; OB/GYN, Obstetrics/Gynecology; PGY, postgraduate year.
Before Intervention (n = 200) (n [%]) After Intervention (n = 131) (n [%]) P Frequency of targeted medications prescribed ACE-I 129 (64.5) 95 (72.5) .149 ARB 29 (14.5) 17 (13.0) .747 Statin 88 (44.0) 50 (38.2) .307 Frequency of risk documentation 40 (20) 49 (37.4) <.001 ACE-I, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; Statin, HMG-CoA reductase inhibitors.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Pregnancy protection and pregnancies in women prescribed ACE inhibitors or ARBs: a cross-sectional study in primary care
- Promoting Safe Prescribing in Primary Care With a Contraceptive Vital Sign: A Cluster-Randomized Controlled Trial
- Contraceptive Methods and Informed Consent among Women Receiving Medications with Potential for Adverse Fetal Effects: A Washington, Wyoming, Alaska, Montana, Idaho (WWAMI) Region Study