
Abstract
Purpose: The purpose of this study was to determine (1) whether our review of systems (ROS) form facilitates identification of sleep complaints; (2) how frequently department physicians investigate these sleep complaints; (3) the prevalence of our family practice patients at increased risk for obstructive sleep apnea (OSA); and (4) how well ROS responses function as diagnostic tests to identify OSA risk.
Methods: We used a prospectively collected sample of consecutive adult patients undergoing preventive examinations at 2 family medicine clinics. Patients completed ROS forms and the Berlin Questionnaire to determine OSA risk level. Physicians at only one site used ROS forms during care.
Results: Two hundred forty-nine of 382 eligible patients (65%) completed forms and underwent examinations. Thirty-seven percent responded positively to sleep-related ROS questions. Physicians documented 24% of those complaints. ROS form use affected documentation (31% with use vs 5% without; P = .03). Thirty-three percent of all patients had increased OSA risk. Fifty-seven percent of high-risk patients responded affirmatively to an ROS question as opposed to 27% for those at lower risk (P < .001). ROS responses were 57% sensitive and 73% specific for increased OSA risk.
Conclusions: Sleep symptoms were common and were recognized significantly more often when our physicians used a ROS form. However, few complaints were investigated. Our current ROS sleep questions are not sufficiently sensitive to identify increased OSA risk. Physicians should prioritize evaluation of sleep dysfunction because of the association with OSA.
Obstructive sleep apnea (OSA) is a common medical disorder with potentially severe health and social consequences. Although the prevalence of OSA was once estimated at 2% to 4% of the population, that is being reconsidered. Young et al1 reviewed epidemiologic data and estimated that roughly 1 of every 5 adults has at least mild OSA and that 1 of every 15 adults has at least moderate OSA. A survey by the National Sleep Foundation2 found that 26% of the population has a high probability of having OSA. In a study conducted among primary care offices, 32% of adults were estimated to be at high risk (HR) for OSA.3 The family physician's office would seem an appropriate setting to identify and intervene with those who are at risk.
The nature of our academic clinical practice, with its preponderance of older patients who have numerous comorbid conditions, led us to explore the prevalence of HR for OSA. We also sought to determine how well we were identifying those with sleep complaints overall and those with OSA in particular.
The American Academy of Sleep Medicine clinically defines OSA as the occurrence of daytime sleepiness, loud snoring, witnessed breathing interruptions, or awakenings caused by gasping or choking in the presence of at least 5 obstructive respiratory events per hour. An alternative definition is the presence of 15 or more events per hour of sleep in the absence of sleep-related symptoms. This frequency of obstruction has a greater association with cardiovascular disease risk.4
It is important to identify and treat persons with OSA because of its associated medical conditions, occupational hazards, and social consequences. Predisposing conditions associated with OSA include age, obesity, male sex, hypertension, and snoring.5 The consequences of untreated OSA may include cardiovascular disease and conditions such as myocardial infarction,6,7 congestive heart failure,8 cerebrovascular accident,9 resistant hypertension,10 and cardiac arrhythmia,11 as well as cognitive dysfunction,12 depression,13 diabetes,14 and motor vehicle accidents.15 Treatment of OSA patients with continuous positive airway pressure may also help treat hypertension,16 depression,17 cognitive dysfunction,18 and systolic dysfunction.19
Guidelines of the Institute for Clinical Systems Improvement suggest evaluating patients who have suspicious signs or symptoms, during routine health maintenance examinations, or who have comorbid conditions, which include cardiovascular disease, coronary artery disease, atrial fibrillation, hypertension, obesity, type 2 diabetes, or a large neck circumference.5
The objectives of this study were to determine (1) whether the use of a patient-completed review of systems (ROS) form facilitated the identification of patients with sleep complaints in our practice; (2) how frequently our physicians completed evaluations for patients with identified sleep complaints; (3) the prevalence of patients at increased risk of OSA; and (4) how well positive ROS items functioned as diagnostic tests for identification of those at HR for OSA.
Methods
Patients and Settings
A sample was generated from consecutive patients, 18 years of age or older, who presented for a general medical examination (GME) (ie, preventive health examination or complete physical) during the 6-week period between March 16 and March 30, 2009, at 2 primary care sites of Mayo Clinic in Arizona. During the study period, a total of 25 resident and faculty physicians saw patients at site 1 (including the 7 physician investigators) and 7 faculty physicians saw patients at site 2.
We excluded patients who had an established diagnosis of OSA or previous sleep complaint work-up. We also excluded patients whose clinical documentation indicated the visit was used for an acute purpose rather than preventive services.
Questionnaires
At our 2 clinical sites, the doctors in one office used a patient-completed ROS questionnaire to try to identify symptoms. At the other clinical site, physicians were expected to conduct an oral ROS with patients and document it. Two items specifically address sleep complaints: “Are you tired much of the time?” and “Do you frequently have trouble sleeping (insomnia)?” We sought to determine whether either of these questions was adequately sensitive to identify patients at increased risk for OSA.
We could not consider referring every patient for polysomnography. Instead, the Berlin Questionnaire was used as a surrogate screening tool and responses were compared with ROS items. The Berlin Questionnaire is a validated instrument that consists of 10 questions in 3 categories that determine risk for OSA.20 In category 1, HR is defined as persistent symptoms reported in response to 2 or more questions about snoring. Category 2 measures wake-time sleepiness, drowsy driving, or both, with persistent occurrences classified as HR. The presence of hypertension or obesity is determined in category 3, and patients were considered at HR if they met criteria in 2 of 3 categories.
The Berlin Questionnaire was validated in a study enrolling 744 adults who presented for unrelated problems at 5 primary care sites. One hundred of these patients underwent polysomnography. A finding of HR on the Berlin Questionnaire predicted an Apnea-Hypopnea Index score >5, with 86% sensitivity and 77% specificity, a positive predictive value of 89%, and a positive likelihood ratio of 3.79.20
To assess whether clinical behaviors might be affected by what each doctor knew or believed about OSA, we asked noninvestigator faculty and resident physicians to complete the Obstructive Sleep Apnea Knowledge and Attitudes (OSAKA) questionnaire. This validated instrument not only measures factual knowledge with 18 questions but also subjects' views about the importance of OSA as a clinical disorder and confidence with identifying and managing patients.21
Data Collection
Scheduled patients received paperwork by mail to complete at home before their visits. This included a cover letter discussing the project, a Berlin Questionnaire, and the standard ROS form.
The Berlin Questionnaires were collected by front desk personnel when the patients arrived at the site. Physicians were not aware of patients' responses. At site 1, where physicians routinely used the ROS form, it was photocopied for use in the study. Patients took the original ROS form into the examination room when meeting with their physician. At site 2, the ROS questionnaire had not been used in routine clinical care. The original was collected for study purposes and was not available to physicians. At both sites, patients who did not bring in the paperwork were offered an opportunity to complete it. Noninvestigator physicians were not notified in advance regarding this project.
Demographic information from patients and physicians was recorded, as were responses to questionnaires. Investigators reviewed patients' electronic medical records for documentation of evaluation or intervention related to a sleep complaint. We decided to exclude from this analysis the clinical behaviors by investigators of ordering testing for sleep complaints to eliminate bias.
Informed consent for use of patient data was implied by completion of the questionnaires and provided orally when patients turned in completed forms to front desk staff. This project was approved by the Mayo Clinic Foundation Institutional Review Board for Human Subject Research. The need for written informed consent was waived.
Statistical Analysis Plan
For the primary question of interest, the associations between the Berlin Questionnaire responses (HR vs low risk [LR]) and the related ROS items (positive vs negative for sleep problems) were assessed using the Fisher exact test. This analysis considered a “yes” response to either ROS question as positive for sleep problems. Supplementary analysis consisted of logistic regression modeling of HR with the Berlin Questionnaire using each of the 2 questions as independent variables. We computed sensitivity, specificity, and positive and negative predictive values of the ROS questions using the Berlin Questionnaire as the comparative standard.
Additional analysis used descriptive statistics (ie, frequencies and relative frequencies for categorical data; means and SDs, medians, minimums, maximums, and ranges for continuous data.) Associations between categorical variables were investigated with 2-way tables and the associated Fisher exact test or the χ2 test. Associations between categorical variables and continuous variables were investigated with side-by-side box plots using the analysis of variance technique and pair-wise comparisons between groups (when multiple groups were being compared) or with the 2-sample t test. Using 2-sided P values, statistical significance was set at P ≤ .05.
Sample Size and Power Analysis
We anticipated a total of 450 to 600 GME visits would be scheduled at the 2 clinical sites during the study period. We predicted a 50% participation rate, for a total of 225 to 300 patients, with an estimated 25% incidence of increased risk for OSA based on patients' responses to the Berlin Questionnaire.
With 250 patients, of whom 25% (63 patients) were expected to be HR according to the Berlin Questionnaire, the primary analysis (using the Fisher exact test with a 2-sided type 1 error) would have 80% power, assuming that 20% of the Berlin LR patients reported sleep problems in ROS responses and 40% of Berlin HR patients reported sleep problems in ROS responses.
Results
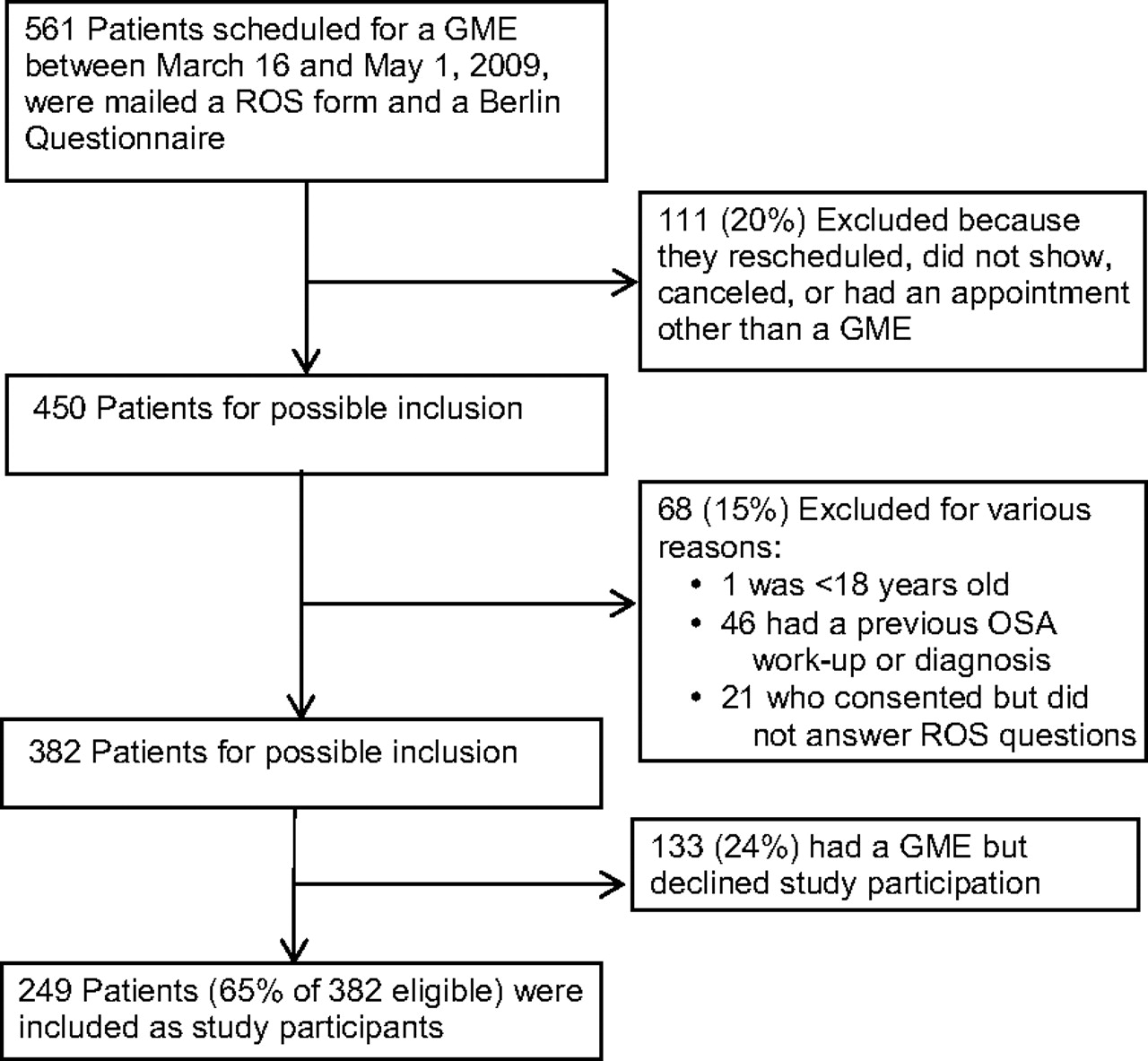
A total of 561 patients had GME appointments scheduled between March 16, 2009, and April 30, 2009 (Figure 1). After applying exclusion criteria, the study participants comprised 249 patients from the 382 eligible, for a 65% response rate. One hundred eighty-four (74%) were enrolled from site 1 (from its 25 attending and resident physicians) whereas 65 patients (26%) were enrolled from site 2 (where 7 attending physicians practiced).

Subject enrollment, accrual, and exclusion criteria. GME indicates general medical examination; OSA, obstructive sleep apnea; ROS, review of systems.
The demographic characteristics of patients are summarized in Table 1. The median age was 65 years (intraquartile range, 55–75 years). Most patients were women, were mildly overweight, and many had hypertension. No significant differences among any patient demographic characteristics were found by clinical site.
Characteristics of Primary Care Patients with Possible Sleep Disorders (n = 249)
A summary of physicians' responses to OSAKA items is presented in Table 2. Twenty-two (88%) of 25 noninvestigator physicians completed the questionnaire. Seventy percent or more of physicians answered correctly 13 of 18 OSAKA knowledge questions. For 8 of the 18 questions, correct answers were provided by more than 90% of the respondents. All respondents knew that women who have OSA may present with fatigue alone, that loss of upper-airway muscle tone contributes to OSA, that untreated OSA is associated with automobile crashes, and that cardiac arrhythmia may be associated with OSA.
Self-Reported Knowledge of and Attitudes About Obstructive Sleep Apnea Held by 22 Primary Care Physicians
In terms of attitudes, OSA was reported to be either very or extremely clinically important to 82% (18 of 22) of the physicians. Sixteen of the 22 physicians (72%) also reported feeling confident in their ability to identify patients with OSA. No differences were observed in OSA knowledge or attitudes of physicians either by clinical practice site or by status (faculty vs resident).
Patient Responses to ROS Questions
In response to the ROS question about tiredness (“Are you tired much of the time?”), 25% (63 of 249) patients responded in the affirmative, whereas 23% (58 of 249) admitted to “frequently having trouble with sleep (insomnia).” Of all 249 patients, 92 (37%) marked “Yes” to one question (or both) and were considered to have a sleep complaint.
Physicians' Recognition, Documentation, and Management of Sleep Problems
When the behavior of the investigators was excluded from analysis (10 positive patient responses were excluded), physicians documented a sleep complaint (indicated by a positive ROS response) 24% of the time (20 times out of 82 positive responses). Inquiries by physicians about excessive sleepiness (25% [5 of 20 patients with a recognized sleep complaint]), the presence of snoring (10% [2 of 20]), or witnessed apnea (10% [2 of 20]) were infrequently documented. There was no documentation of direct inquiries about impaired driving.
ROS form use was significantly associated with an increased rate of sleep complaint documentation. There was a 5% documentation rate (1 of 20) of ROS sleep complaints completed by site 2 physicians versus a 31% rate (19 of 62) at site 1 (Fisher exact test, P = .03). Despite use of the ROS form, about two-thirds of patients at site 1 who had sleep complaints did not have them addressed in visit documentation.
Eighty-two of 227 patients (36%) indicated sleep complaints on ROS forms. Nine of these 82 patients (11%) received further investigations. Four were suspected of having a sleep-related breathing disorder and had overnight oximetry. The remaining 5 had other interventions, such as metabolic work-ups for fatigue symptoms, or were treated or referred for depression.
Physician Characteristics and Sleep Complaint Recognition or Interventions
Physicians who recognized and documented sleep complaints did not differ in their knowledge or attitudes from those who did not. There was no statistically significant association between increased OSA knowledge or attitudes and the rate of ordering interventions.
Patient Responses to Berlin Questionnaire Items
One hundred thirty-four of the 249 patients (54%) admitted that they snored but believed that they did so quietly (Table 3). Among snorers, 59% snored frequently and loudly enough to bother others. They rarely were noted to have apnea. About one-third of the patients reported feeling frequently fatigued after sleeping overnight or reported feeling excessively tired during the day. One-third (33% [81 of 249]) of the patients were at increased risk for OSA based on Berlin Questionnaire responses (95% CI, 26.7–38.3).
Responses of Patients to 10 Berlin Questionnaire Items Regarding Sleep Dysfunction*†
Characteristics of Patients at Increased Risk for OSA
Patients who were HR according to the Berlin Questionnaire were significantly more likely than those at LR to be overweight (mean BMI, 29 vs 25.4; P < .001); have hypertension (73% [59 of 81] HR vs 30% [51 of 168] LR; P < .001); have diabetes (16% [13 of 81] HR vs 5% [8 of 168] LR; P = .003); or have a history of cerebrovascular accident or a transient ischemic attack (7% [6 of 81] HR vs 1% [2 of 168] LR; P = .009). There was no gender difference between risk groups.
Relationships between ROS Sleep Items and Patients at Increased Risk for OSA
There was a significant association between a positive response to an ROS question and being at increased risk of OSA according to the Berlin Questionnaire. Forty-six of 81 Berlin Questionnaire HR patients (57%) marked an ROS question affirmatively compared with only one-fourth (27% [46 of 168]) of Berlin Questionnaire LR patients (P < .001). However, ROS questions had a sensitivity of only 57% (95% CI, 45–68) and a specificity of 73% (95% CI, 65–79) for Berlin HR. For an undifferentiated patient, the positive predictive value of a positive ROS question indicating HR per the Berlin Questionnaire was 50% (95% CI, 39–61). The negative predictive value for ROS items compared with the Berlin Questionnaire as the standard was 78% (95% CI, 70–84).
Logistic regression analysis showed that a patient who responded positively to the question “Are you tired much of the time?” had 3.8 times greater odds of being at increased risk for OSA than a patient who responded negatively (95% CI, 2.1–6.9). Responding in a positive manner to the question “Do you have frequent trouble sleeping (insomnia)?” did not confer as much risk of being HR per the Berlin Questionnaire (odds ratio, 2.7; 95% CI, 1.5–4.9). Answering one or both ROS questions positively created a positive likelihood ratio of 2.1, whereas answering negatively to both produced a negative likelihood ratio of 0.6. If the pretest probability of being at HR for OSA in our primary care setting is 33%, a positive ROS response would increase the posttest probability to 51%. Negative responses to both questions decreased the posttest probability of disease to 23%.
Discussion
Sleep problems are common among primary care patients. Alattar et al22 surveyed 1934 adult patients in 5 family practice offices. More than half reported excessive daytime sleepiness. Up to a third reported symptoms of OSA. Sleep complaints were significantly associated with hypertension, depression, and pain syndromes.
In our study, 37% of patients reported a sleep complaint on a self-completed ROS form. The rate of patients being HR on the Berlin Questionnaire was 33%, which confirms rates found in another study in a primary care setting.3 Using the STOP (snoring, daytime tiredness, observed apnea, and high blood pressure) Questionnaire, Chung et al23 found that 28% of patients receiving preoperative evaluation were at increased risk for OSA. The prevalence of OSA risk seems to be greater in medical settings than in the community.2 These patients frequently present to health care providers, which should help provide opportunities to identify and treat them.
The ability to identify patients at risk for OSA in a busy primary care setting has proven to be difficult.24 There is no clear consensus on what interventions work well in case-finding.25 The Institute for Clinical Systems Improvement guidelines5 suggest that the health maintenance visit is a good opportunity to evaluate patients. Guidelines recently published by the Adult Obstructive Sleep Apnea Task Force of the American Academy of Sleep Medicine provide similar recommendations.4 A 2009 American Medical Association House of Delegates Resolution endorsed the view of OSA as a major public health issue, called for a national education campaign, and encouraged research and increased physician knowledge about OSA.26 The importance of identifying and treating those with OSA to avoid the serious associated medical consequences cannot be overemphasized.
In our study, during GME visits physicians identified and evaluated only a minority of patients who had sleep concerns, even when they had a completed ROS form in front of them. This may be because of the multiple competing agendas interacting during the “complete physical” visit: discussing and providing preventive services, addressing chronic disease management problems, and evaluating acute care issues. We were pleased to see that use of the ROS form had a positive impact, significantly increasing sleep complaint documentation from 5% to 31%; however, pragmatically its effect was not sufficient. The majority of symptomatic patients still did not have their complaints recognized, documented, or addressed with further history-taking or interventions.
Although there were significant associations between a patient endorsing an ROS item and being at increased risk for OSA, the sensitivity of our 2 ROS questions was poor. Half the patients who were HR per the Berlin Questionnaire answered neither ROS question positively. Most likely, many patients believe that snoring and fatigue are “normal” for them. The positive predictive value of an ROS item marked in the affirmative, indicating HR per the Berlin Questionnaire, was only 50%. Neither positive nor negative likelihood ratios created by ROS responses provide any substantial increase or decrease the posttest probability of disease. Thus, we need to redesign the ROS form so that it can better facilitate recognition of OSA symptoms and lead to higher rates of evaluation.
Some previous studies have cited a lack of understanding of OSA among primary care physicians,27 but we do not believe that this is true in our practice. According to OSAKA data, our physicians were highly knowledgeable about OSA, and most expressed confidence in their ability to identify and manage patients. There was no difference in the knowledge or attitudes of physicians by whether they did or did not recognize and document sleep complaints. There seems to be a gap between factual knowledge (a mean score of nearly 80% correct on the OSAKA) and appropriate clinical behaviors. Other factors related to the clinical encounter may be responsible for the low rates of documentation of our patients' sleep complaints and subsequent investigation. It is noted that our physicians' mean scores for their confidence in identification and management of patients who have sleep apnea are lower than that of their attitudes about the importance of identification of OSA.
In the past little emphasis has been placed on educating medical students, resident physicians, or practicing doctors about sleep apnea. We are encouraged by the fact that the opportunity of a Certificate of Added Qualification in Sleep Medicine is now available through the American Board of Family Medicine.28
Strengths and Limitations
Few studies of OSA screening tools have been completed in primary care settings with undifferentiated patients. Most have used referred patients in tertiary care settings. We investigated the utility of a real-world, simple tool (our ROS form) for indentifying sleep complaints and compared this to the Berlin Questionnaire, a validated instrument that could be easily incorporated into daily clinical practice.
We cannot make inferences about cause and effect because this was not a randomized trial. Though we did provide operational definitions for record review as to what constituted “documentation” of a sleep complaint and what behaviors were “investigations,” we did not determine interrater reliability or cross check each others' audits. We were also aware of the identity of the primary care physician of each patient. Each of these issues could have introduced an opportunity for bias.
Although we examined behaviors in one department at a single institution, we believe our findings are generalizable to the difficulties encountered at other busy primary care practices. Prioritizing evaluation of sleep complaints is difficult. However, lack of documentation about sleep complaints does not prove that they were not addressed. Other concerns may have had priority.
Even when sleep complaints are investigated, follow-up is problematic. Martinez et al,29 in a review of patients sent for overnight oximetry from a general internal medicine practice, found that one-third of those with abnormal results did not receive a subsequent referral to sleep medicine specialists. Unfortunately, only 30% of patients referred for further evaluation actually followed through.
Future Research
Our ROS form is undergoing modifications. We hope this will lead to improvement in rates of recognition. We also identified a cohort of patients at HR for OSA who might benefit from evaluation, and they have been contacted. Potentially, one-third of our entire adult patient population could benefit from further investigation. Identifying the most effective and efficient methods to accomplish this will be the subject of further study.
Conclusions
Patients in our practice were frequently at HR for OSA. Although it was helpful for patients to complete an ROS form (ie, it produced a statistically significant increase in the rate of identification of sleep complaints), having the ROS form completed did not make a truly significant clinical impact on physician behavior. The form itself might be modified to elicit symptoms more specific to OSA (eg, presence of snoring and excessive daytime sleepiness), but more interventions may be necessary to identify patients with OSA. Case-finding during routine preventive health examinations may not always be practical given the competing agendas patients and physicians bring to these encounters. Efforts may need to focus on encouraging patients to vocalize their sleep complaints in general and on educating about personal susceptibility for OSA in particular. Good physician knowledge and appropriate attitudes about OSA did not translate into high rates of documentation or clinical investigation. These findings demonstrate the need to fully address any sleep concern and to prioritize it during the clinical encounter. Doing so may indeed be the best opportunity for engaging the patient and making a meaningful impact both on daily function and long-term health.
Acknowledgments
We wish to thank James M. Parish, MD, Division of Pulmonary Medicine, Mayo Clinic, Scottsdale, Arizona, for his editorial assistance and content expertise.
Notes
This article was externally peer reviewed.
Funding: Funding for statistical analysis was provided by grant no. 09-000694, a Small Project Grant from Mayo Clinic, Scottsdale, AZ. Funding for editorial support through the Section of Scientific Publications was provided by the Department of Family Medicine, Mayo Clinic, Scottsdale, AZ.
Prior presentation: Presented as a poster at the annual spring conference of the Society of Teachers of Family Medicine, Vancouver, British Columbia (April 24–28, 2010).
Conflict of interest: none declared.
- Received for publication August 24, 2010.
- Revision received October 24, 2010.
- Accepted for publication November 1, 2010.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Obstructive Sleep Apnea: Preoperative Screening and Postoperative Care
- Fatal Consequences: Obstructive Sleep Apnea in a Train Engineer
- Content Usage and the Most Frequently Read Articles by Issue in 2011
- Is Insomnia an Independent Predictor of Obstructive Sleep Apnea?
- Sleep and the Family Doctor: Time to Lead