
Abstract
Pectus excavatum (PE) is a posterior depression of the sternum and adjacent costal cartilages and is frequently seen by primary care providers. PE accounts for >90% of congenital chest wall deformities. Patients with PE are often dismissed by physicians as having an inconsequential problem; however, it can be more than a cosmetic deformity. Severe cases can cause cardiopulmonary impairment and physiologic limitations. Evidence continues to present that these physiologic impairments may worsen as the patient ages. Data reports improved cardiopulmonary function after repair and marked improvement in psychosocial function. More recent consensus by both the pediatric and thoracic surgical communities validates surgical repair of the significant PE and contradicts arguments that repair is primarily cosmetic. We performed a review of the current literature and treatment recommendations for patients with PE deformities.
- Pectus Excavatum
- Chest Wall Deformities
- Congenital Defects
- Cardiovascular Disorders
- Musculoskeletal and Connective Tissue
- Review
Pectus chest deformities are among the most common major congenital anomalies found in patients in the United States. They occur in approximately 1 of every 300 to 400 white male births.1–3 Men are afflicted 5 times more often than women.2,4 The condition is uncommon among African Americans and Latinos.2,5 Pectus excavatum (PE) with sternal depression is approximately 6 times more common than pectus carinatum (protrusion).4,5 The cause of PE remains unknown. Approximately 40% of patients with pectus deformities have family members who also have deformities, although a direct genetic link has not been identified.4,6–8 Disturbances in the growth of the sternum and costal arches, as well as biomechanical factors, are suspected in the pathogenesis.1,2,4,6,9–11 The involved cartilages can be fused, deformed, or rotated. Intrinsic abnormality of the costochondral cartilage is suggested by the significant occurrence of PE among patients with connective tissue disorders, such as Marfan syndrome.4,6,8,12 There is also a high percentage of scoliosis associated with the disorder.6–8,12 Abnormalities of the cartilages removed during surgery have also been reported, including stress/strain deformation and abnormal collagen content.1
PE can be present at birth but is most frequently recognized during early childhood. During rapid adolescent growth, many patients experience a marked increase in the severity of the depression until full skeletal maturity is achieved.5,13–20 In severe cases or those in which depressions directly impinge on the right ventricle, PE is more than a cosmetic deformity.21–24 Many patients do not undergo repair during childhood and subsequently experience progressive a worsening of symptoms and cardiopulmonary function with increasing age.18–20,24–26
One theory for the worsening of symptoms that is experienced with age is that the chest wall is very compliant in infancy but, with aging, a steady decline in compliance is experienced and it becomes relatively stiffer compared with the lungs. In adults the loss of elasticity and flexibility of the chest can lead to cardiac symptoms with only moderate exertion.8,26 A similar phenomena is also seen in patients with scoliosis as they age.6,7 Publications regarding the surgical management of adult patients with pectus deformities are few, but have increased significantly during the past few years with greater recognition of the physiologic and psychologic impact of the disease.8,18,19,24,26–36 Despite well-documented reports to the contrary, the longstanding misconception persists that PE is a cosmetic defect with no physiologic consequences. This misconception has resulted in patients reaching adulthood with uncorrected defects. Some patients will develop cardiopulmonary symptoms for the first time as they age and others will experience a worsening of symptoms they have endured for years.
Clinical Features
The PE depression most frequently involves the lower sternum and cartilages but can be extensive with varying degrees of rotation and asymmetry.1,2,8,12 Deformities are seen in many different configurations, the most common being a cup-shaped concavity. These are generally well defined, deep, and involve the lower end of the sternum with the depression of costal cartilages 4 through 7 (Figure 1). Patients can also have a significant extensive depression with involvement of the upper costal cartilages, creating a more severe, broad form of concavity (Figure 2A and B).2,8,36,37

Patient with a more focal classic “cup-shaped” or “bowl-shaped” pectus excavatum deformity.

A: Patient exhibiting a broad, more extensive pectus excavatum deformity. B: Patient with Marfan's syndrome and extensive pectus excavatum deformity.
Symptoms
Patients with PE can present with many different symptoms. The symptoms often vary in severity and their effect on patient's daily activities. The severity of the defect does not necessarily correlate with the severity of symptoms. Many patients are asymptomatic at a younger age but start experiencing symptoms as they enter their teens.14,18,19,24,36 This may be because of a worsening of the defect or an increase in exercise and physical activity. The most consistently expressed symptoms are dyspnea with exercise and loss of endurance. A list of the common symptoms of PE is provided in Table 1.3,8,13,14,17,18,30,36,38
Most Frequent Symptoms of Pectus Excavatum Noted by Patients
Despite multiple studies evaluating cardiac and pulmonary function, there has been no conclusive or consistent demonstration of physiologic impact correlating with the symptoms of PE. Anatomic abnormalities, including decreased thoracic volume and cardiac compression, are thought to explain the physiologic effects noted by patients.17,36,37 The increased work of breathing from a partially restricted chest wall with impaired oxygen delivery to working muscles as the result of decreased venous return to the right heart may also play a role.16,17,23 Sternal compression is suspected to decrease thoracic volume, which can reduce the SVO2, exercise tolerance, tidal volume, and vital capacity, causing dyspnea and a decrease in endurance with compensatory tachypnea during exercise.13,16,39–41 Cardiac compression can also reduce stroke volume and cardiac output in severe deformities, causing accelerated fatigue and compensatory tachycardia.16,17,22–24,40 A systolic cardiac murmur is sometimes heard and mitral valve prolapse is found in as many as 25% of patients.4,5,31 The percentage of pectus patients with mitral valve prolapse seems to increase with age.3,31 Resolution of the mitral valve prolapse with release of the chest wall entrapment is seen in more than half of patients after surgery.8,15,17,31 Dysrhythmias can also be seen, including first-degree heart block, right bundle branch block, and Wolff Parkinson-White syndrome.8,17,42
The psychosocial issues surrounding body image among teenagers can be significant, life-altering, and occasionally life-threatening.8,36,37 Poor body image and impaired psychosocial function is an enormously important concern for surgical repair.36,37 Children and adolescents with potentially visible physical differences may be at risk for body image and interpersonal difficulties.27 Psychological research about patients with disfigurement confirm disturbance of the body schema and altercation of the individual's self-representation.34 Surgical repair of PE can significantly improve the difficulties with body image and limitations on physical activity that are experienced by patients.20,36,37,43 These results should prompt physicians to consider the physiologic and psychological implications of PE just as they would any other physical deformity known to have such consequences. In a multicenter investigation, geographically dispersed children and adults demonstrated a marked effect of the chest deformity on perceived ability to exercise, which was consistently improved with surgical correction.19,20,35,37,43 The importance of these concerns to the child and family should not be underestimated by physicians.36,44
Investigation as to the cause of exercise intolerance and perceived limitation of ability have yielded mixed results, and whether surgical repair corrects these deficits is controversial.12,19,22,25,37,41,43 Malek et al22 and Malek and Marelich41 performed a comprehensive meta-analysis on publications reporting postoperative cardiopulmonary results among PE patients. The critical finding of the study was that surgical repair improved cardiovascular function by more than ½ standard deviation. The patient's personal testimony has been the most convincing evidence for repair. The majority of patients with symptoms reported significant improvement after repair. These findings, along with current ongoing investigations, further the argument that surgical repair of PE is indicated for symptomatic patients regardless of physiologic testing and is more than primarily cosmetic.
Evaluation
The presentation of a patient with PE warrants a thorough workup to access the significance of the defect. This workup does not necessarily include every possible physiologic test, but can include those necessary to determine whether the patient should be referred to a surgeon for a discussion of repair options.
Radiographic Evaluation
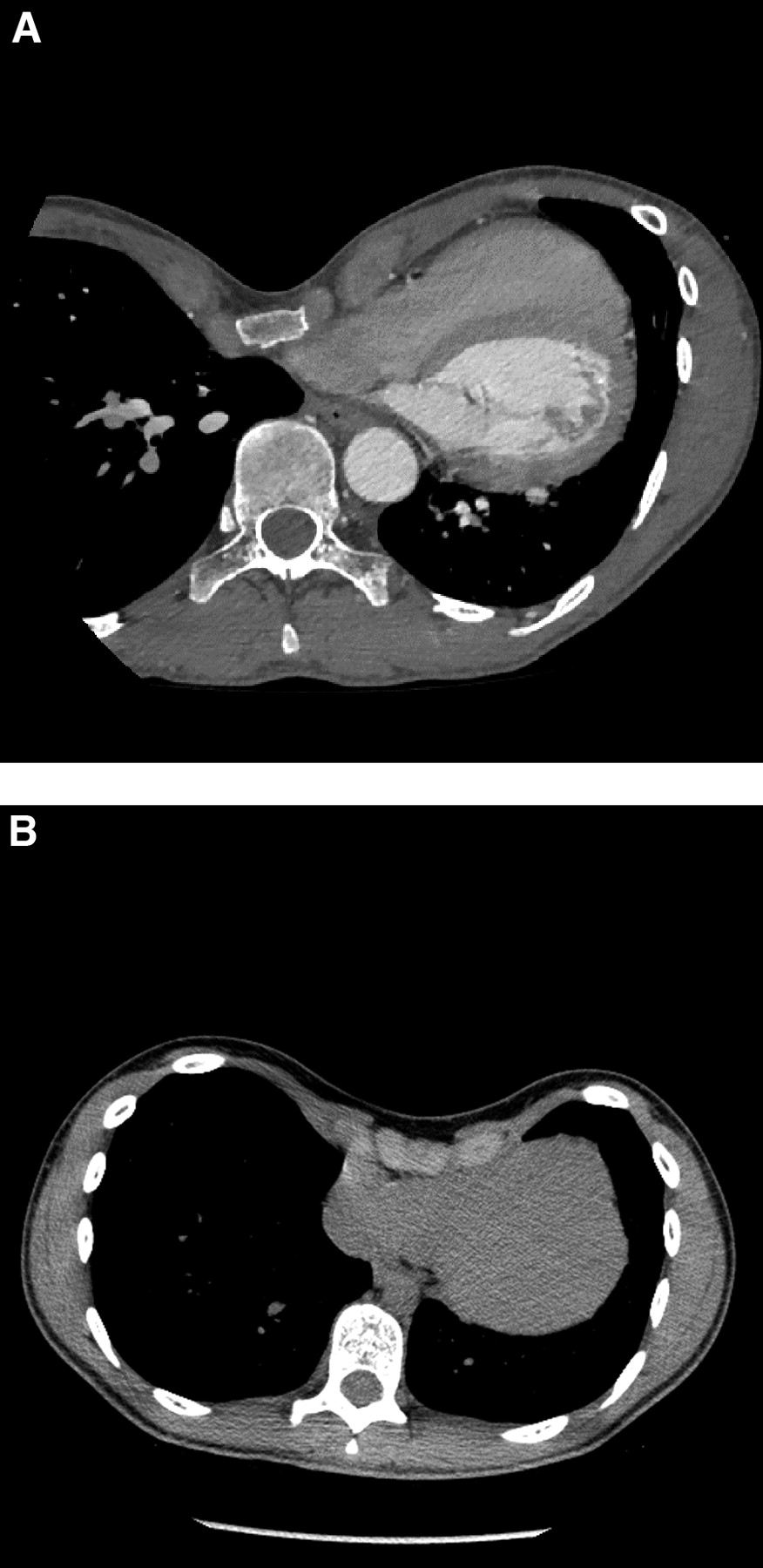
Imaging for anatomic assessment and documentation of the chest dimensions is important and remains a mainstay of the anatomic evaluation of PE. A noncontrast computerized tomographic (CT) scan is useful to access the deformity of the bony and cartilaginous skeleton in a 3-dimensional view, which clearly reveals any cardiac compression (Figure 3a) or cardiac displacement (Figure 3B). Magnetic resonance imaging can be used instead of CT scan to reduce radiation exposure but bony detail is better seen by a CT scan.8,17,25 An index of severity can be calculated by measuring the inner width of the chest (at the lowest level of the pectus defect) and dividing it by the distance between the posterior surface of the sternum (at the lowest part of the defect) and the anterior surface of the spine.17,28,45 The severity index for healthy people is 2.52.8,45 In general, an index of ≥3.1 is considered severe.2,3,5,8,13,14,17–19,25,46,47

Computerized tomographic scans of the chest showing left-sided heart displacement (A) and right ventricular compression (B) by severe pectus excavatum deformity.
Electrocardiogram
Documentation of any dysrhythmias should be done with a 12-lead electrocardiogram.
Transthoracic or Transesophageal Echocardiogram
It may be useful to perform an echocardiogram because the depressed sternum may compress the right atrium and right ventricle, interfering with diastolic filling of these structures.36 Mitral valve prolapse is commonly seen among patients with PE and should also be documented if it is present. Evaluation of the aortic root and valve is also critical in patients with suspected or confirmed Marfan syndrome.
Pulmonary Functions
Both static and exercise pulmonary function tests may be useful in eliciting a physiologic effect of the PE defect on the patient. Static pulmonary function tests are the least sensitive but may show a significant decrease in forced vital capacity and maximal ventilatory volumes, which indicate restrictive airway disease. Patients may also have evidence of mild obstructive airway disease. In general, most patients with significant PE will still have a normal or low-normal static pulmonary function test.
Cardiopulmonary Exercise Testing
Cardiopulmonary exercise testing can also be used to show significant physiologic effects of the PE. The amount of oxygen that can be delivered to the tissues with exercise can be examined. A decrease in the O2 pulse (mL/beat) and amount of oxygen that could be delivered (Vo2 L/min and Ve L/min) may be significantly below predicted values in patients with PE.24,36 Low-normal and below-normal values indicate that surgical correction could benefit the patient.22,24,25,36,48 Figures 4 and 5 show the cardiopulmonary exercise testing Vo2/heart rate and Vo2/ CO2 finding from a symptomatic PE patient before and after an operation.
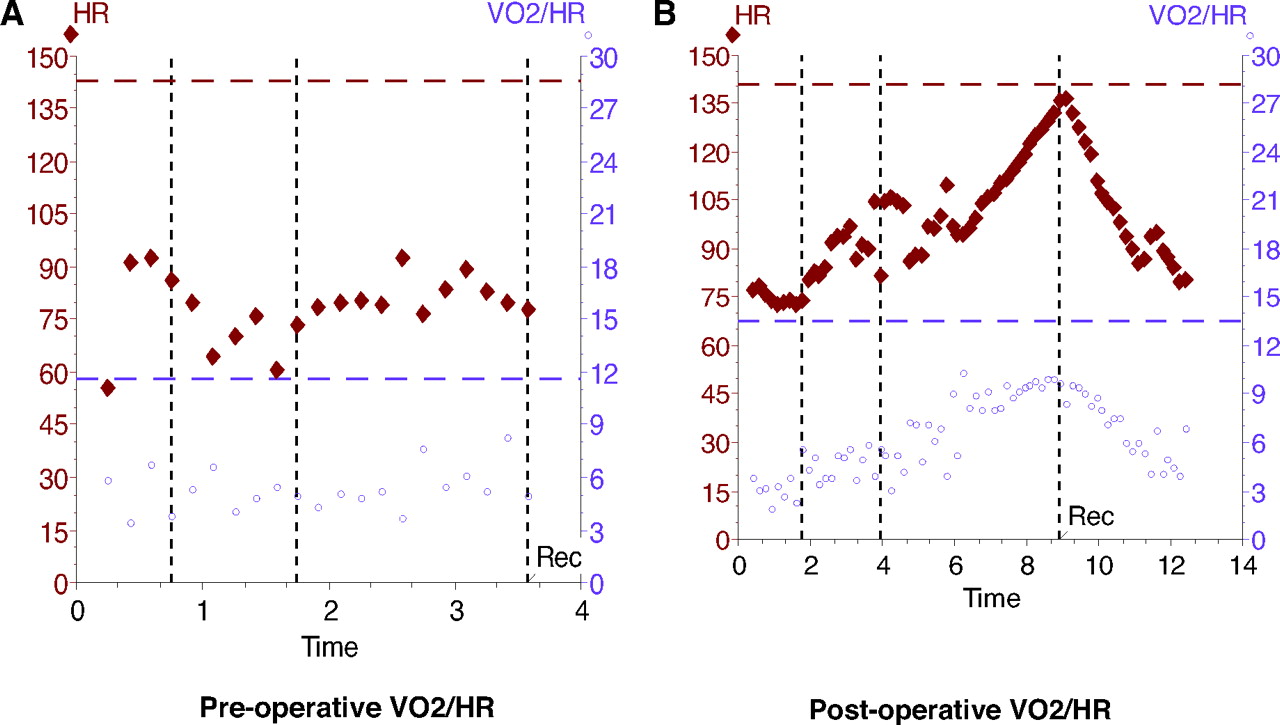
Cardiopulmonary exercise testing VO2/heart rate study from a symptomatic PE patient before (A) and after (B) operation.

Cardiopulmonary exercise testing VO2/CO2 study from a symptomatic PE patient, before (A) and after (B) operation.
Indications for Surgery
The primary care physician needs to have a good understanding of the disease and realize the importance of the deformity. Surgical correction of PE can be performed safely with minimal risk. Referral for consideration of surgical treatment for severe cases should be made. Operation for correction of PE is readily accomplished in teenagers, who are close to the age of skeletal maturity.5,29,36,38,47 The timing for surgery is problematic in the younger child.8,14,36,46,47,49 Currently, most surgeons will wait for patients to reach the adolescence or early teenage years to perform repair. Repair during the later stages of teenage growth allow the patient to complete their growth and have a lower chance of recurrence. Younger children with significant cardiopulmonary compromise may also be candidates for repair depending on the severity of their symptoms; however, repair at too early of an age can result in improper growth of the chest wall and other complications, including recurrences.3,29,30,36,49 Adult repair is also feasible and has been reported in patients as old as 78 years.18,19,24,26,29,30,32,50
In general, referral to a surgeon for consultation should occur when a patient demonstrates any of the criteria listed in Table 2. Most patients will be considered for surgical correction if they demonstrate at least 2 of the listed criteria.36 Others may need to be followed closely to watch for progression or worsening of the defect and symptoms as they age.
Criteria for Surgical Referral
Surgical Repair
Surgical repair of PE has evolved significantly during the past 50 years. There are a variety of techniques that have been successfully used, but the 2 most common methods include modifications of the open approach, first described by Ravitch,14,21 and the Nuss, or minimally invasive, approach.
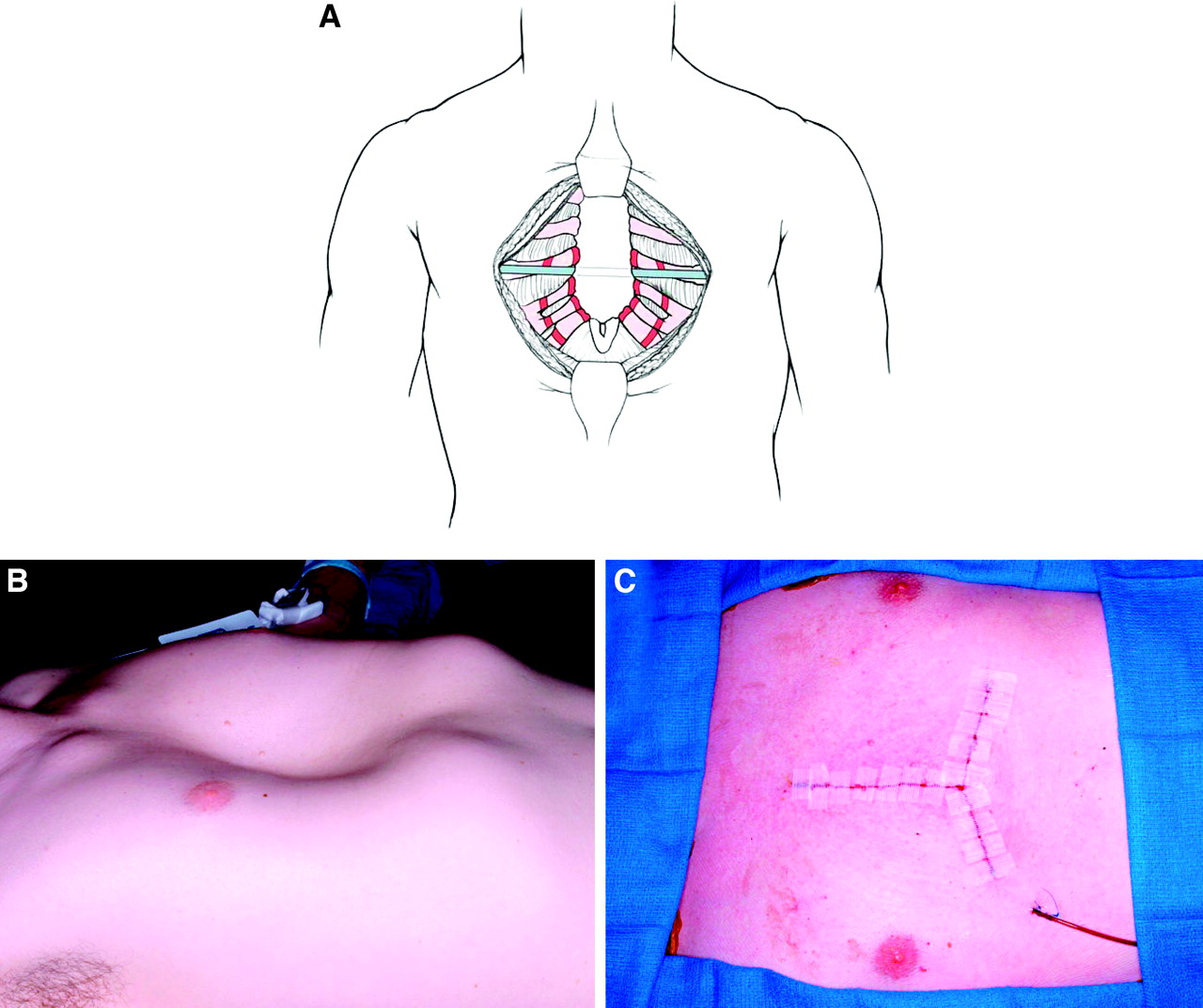
Modifications of the open repair as described by Ravitch have been used for decades and are still used routinely.5,14,15,19,28,46,51,52 The technique resects minimal cartilage and yields excellent results with low morbidity (Figure 6).14,15,46,51 There have been a variety of modifications reported, including the use of mesh, but the majority of procedures include placement of a metal strut to support the sternum, which may be left in place for 6 months to a year. Proponents of the modified Ravitch claim lower cost, shorter hospitalization, and less postoperative pain.38,46,53,54 It is ideal for patients who have a combination of PE and carinatum, significant asymmetry, or extensive defects involving the upper ribs and cartilage.
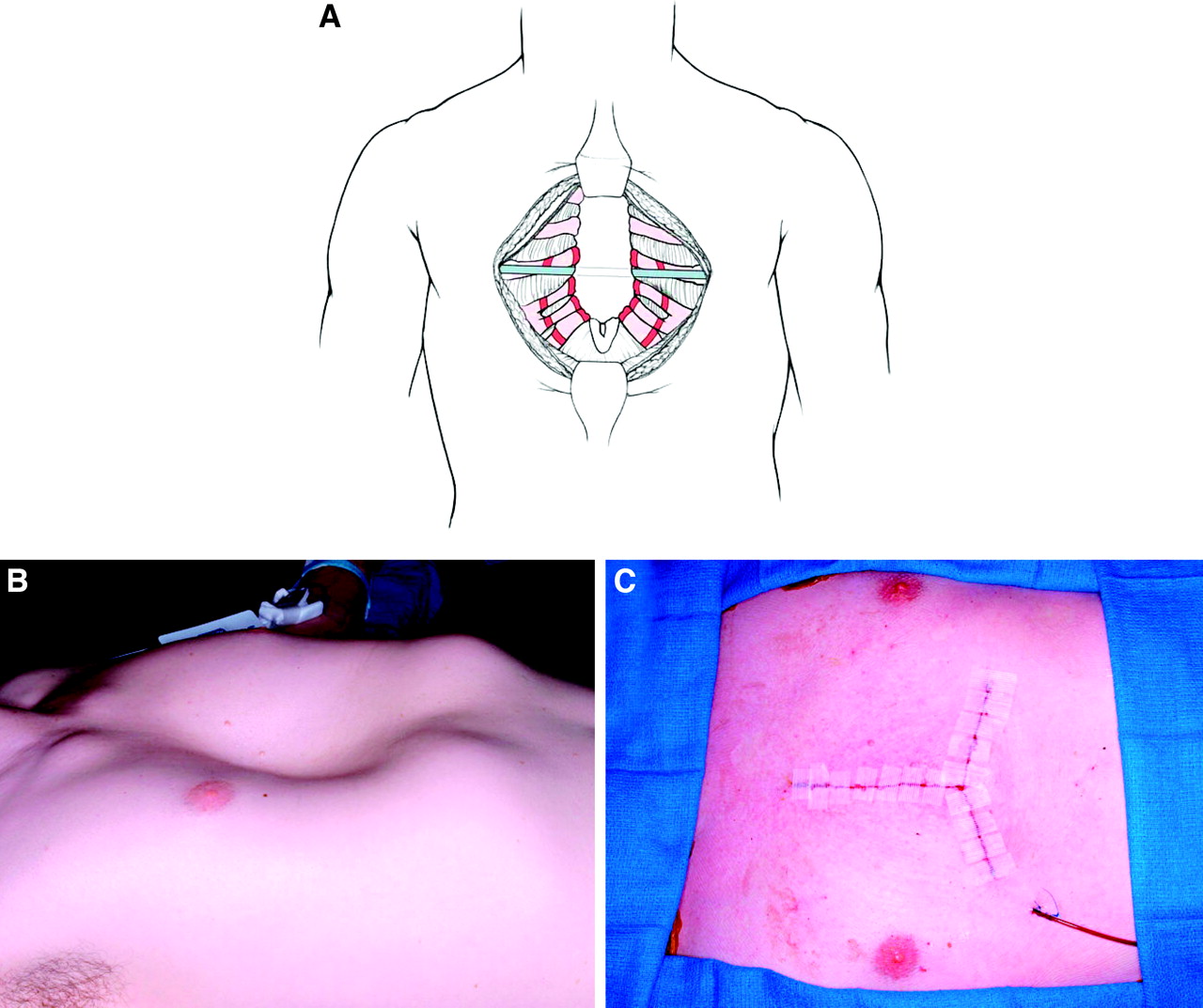
Schematic diagrams (A) and operative photographs (B and C) depicting the modified Ravitch procedure.
A minimally invasive technique for repair was described by Nuss et al42 in 1998. This method of repair involves the placement of a substernal concave bar, which is passed behind the sternum through the chest and “flipped” into a convex position to elevate the sternum outward (Figure 7). The bar is left in place for 2 to 3 years while the anterior chest wall remodels. Cosmetic results are reported as good to excellent in >85% of patients, and the operation has rapidly gained popularity because of the small skin incisions and shorter operative time.20,25,26,47,50 In recent years the operation has been successfully used to repair PE in adults, although higher rates of complications and postoperative pain have been reported.26,29,32,53 The advantages of the Nuss approach include avoiding an anterior chest wall incision, resection of rib cartilages, and no sternal osteotomy. Incorporation of thoracoscopic techniques has made the operation safer, allowing for visualization of the heart when the bar is passed retrosternal.29,47 An incidence of bar displacement rarely needing reoperation was reported at 5% to 7%.38,42
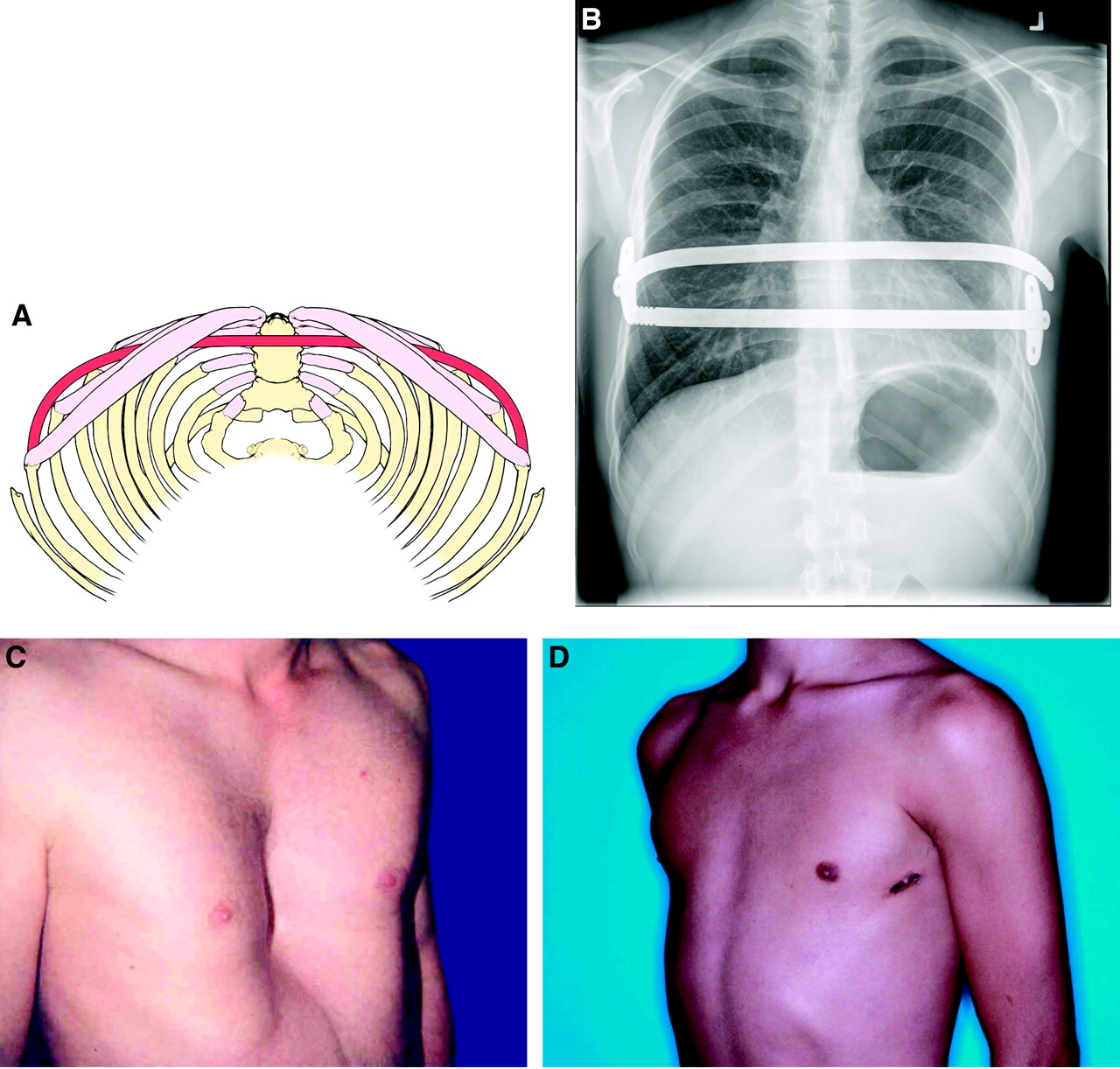
A: Schematic drawing showing position of support bar with the Nuss procedure. B: Chest roentograph showing 2 sternal support bars after repair with the Nuss procedure. Photographs before (C) and after (D) the operation of a patient with pectus excavatum undergoing minimally invasive Nuss repair. Lateral incisions are used to place the support bar.
Several studies have compared the 2 methods.25,29,38,53,54 In general, the minimally invasive Nuss procedure took less time to perform but required a longer hospital stay—The open technique usually ranged from 1 to 3 days in the hospital and the minimally invasive approach ranged from 3 to 6 days—and required more postoperative analgesics than the modified Ravitch procedure. Overall, there seems to be no significant advantage for either approach. Multicenter studies about PE have demonstrated that repair by either the Nuss procedure or an open operation could be accomplished successfully with minimal complications and good pain control.25,42,43,46,53,54
Other Repair Options
Innovative, nonsurgical approaches are also under development and evaluation, including vacuum treatment and the use of magnetic forces.55,56 The Brazilian orthopedic surgeon, Haje,11,57 has used bracing as a nonoperative approach with success. Custom-made silicone implants have also been used with a good esthetic outcome, but the deformity and physiologic consequences of the chest wall depression are not addressed.58
Conclusion
The philosophy of PE deformity has evolved as more data and treatment experience has accrued. PE is no longer felt to be just a cosmetic deformity but physicians may continue to base their recommendations for surgery on limited and preconceived knowledge from the past. As a consequence, many well-intentioned physicians advise patients that their deformity produces few symptoms and is primarily a cosmetic problem. The idea is conveyed that it will improve with age and surgical repair is complicated and unnecessary. The primary care physician has played and continues to play a critical role in the diagnosis and referral of these patients. The cardiopulmonary effects of severe deformities can be significant and may worsen as the patient ages. Surgery can be performed safely with few complications and short hospitalization. That surgical treatment is performed at a high-volume center with a surgeon dedicated to pectus repair is critical to success.
Notes
This article was externally peer reviewed.
Funding: none.
Conflict of interest: none declared.
- Received for publication June 9, 2008.
- Revision received October 5, 2009.
- Accepted for publication October 14, 2009.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Earlier preoperative percutaneous intercostal cryoanalgesia improves recovery after pectus excavatum surgery
- Tricuspid Valve Annulus Size by Echocardiography: Predictor of Cardiac Limitation in Pediatric Pectus Excavatum
- Quality of life of children and young people with anterior chest wall deformity: a systematic review of the literature
- Quality of life of children and young people with anterior chest wall deformity: a systematic review of the literature
- Can categorised values of maximal oxygen uptake discriminate patterns of exercise dysfunction in pectus excavatum: a prospective cohort study?
- Research progress in the effects of pectus excavatum on cardiac functions
- Proper compression landmark and depth for cardiopulmonary resuscitation in patients with pectus excavatum: a study using CT
- Key Questions and Technology in Clinical Practice