
Abstract
Background: Health literacy has been defined as the ability to obtain, process, and understand the basic information needed to make appropriate health decisions. Half of adults lack the health literacy skills needed for our complex health care environment. In 2005, Weiss et al introduced the Newest Vital Sign (NVS), an instrument that can be used to quickly assess health literacy. The purpose of this study was to determine the acceptability and timeliness of using the NVS to measure the level of health literacy in various suburban, urban, and rural primary care settings. A secondary purpose was to determine the influence of taking a health class on one's level of health literacy.
Methods: In this cross-sectional design, adults were recruited from 4 primary care settings and student athletes were recruited during preparticipation sports physicals. The NVS was administered and health literacy rates were compared with known trends. A subset of 50 patients was timed during test administration, and refusals were logged throughout. The adults and the athletes were analyzed separately.
Results: One thousand fourteen patients (including athletes) agreed to participate (response rate, 97.5%). Average time needed to complete the NVS was 2.63 minutes. Of the adults tested, 48.1% demonstrated adequate health literacy. In logistic regression analysis, younger age, more formal education, health class participation, and body mass index were positive predictors of adequate health literacy among adults. An interaction term was used for gender/race, with white women used as the comparator. The gender/race odds ratio negatively affected literacy, with white men at 0.497 (95% CI, 0.328–0.753), non-white women at 0.177 (95% CI, 0.111–0.282), and non-white men at 0.210 (95% CI, 0.110–0.398). Among the participating middle- and high-school athletes, 59.7% had adequate health literacy. In logistic regression of this population, body mass index was a positive predictor whereas gender/race was a negative predictor.
Conclusion: The NVS revealed health literacy status in less than 3 minutes, was widely accepted, and provided results comparable to more extensive literacy tests. Particularly, taking a health education class was associated with higher levels of health literacy among adults.
Health literacy has been defined as the ability to obtain, process, and understand basic information and services needed to make appropriate health decisions.1 A patient must be able to understand and use information in a meaningful way to be able to improve health and nutrition. Furthermore, education level, reading level, and other demographics alone do not accurately predict a patient's health literacy. The average, English-speaking US adult reads at an 8th- to 9th-grade level whereas most health care materials are written at 10th-grade level or higher.2–4
Everyday in a physician's office, patients are asked to sign forms consenting to treatment, stating specifics regarding a procedure, or detailing privacy of medical records and transference of medical records. They are also given written and verbal information about their medical condition(s) and/or prevention of disease. To have appropriate educational materials and standardized forms available that foster a fully informed decision regarding a patient's health care needs and rights, a physician must know the average health literacy level of his or her patient population. Physicians often have difficulty recognizing individuals with poor literacy skills5,6 and overestimate patients’ levels of health literacy, especially among minorities.7
The Joint Commission on Accreditation of Health Care Organizations established health literacy benchmarks for hospitals to achieve by 2010.2 In 2004, the Institutes of Medicine, the Agency for Healthcare Research and Quality, and the American Medical Association all issued reports about health literacy,1 noting that up to 50% of adults lack the literacy skills needed to function adequately in a health care environment. Inadequate health literacy has been associated with increased incidence of smoking, advanced age, increased risk of hospitalizations, increased likelihood of carrying a weapon, higher glycated hemoglobin levels, and a decreased incidence of breastfeeding.4,8–12 However, other investigators found mixed results when they examined the association between the level of health literacy and health outcomes.13,14
Efforts have been made to improve the level of health literacy among health care recipients as well as among the general public. Health care providers have modified educational materials or have used visual or multimodal teaching techniques. Mandatory health education classes have become more prevalent in middle and high schools, although their impact on improving health literacy is unclear.15
The Test of Functional Health Literacy in Adults (TOFHLA) has been widely used for assessing health literacy, but takes 18 to 22 minutes to administer. The short form (S-TOFHLA) can take 7 to 10 minutes to administer. In 2005, Weiss et al16 developed a new screening instrument, the Newest Vital Sign (NVS), to assess level of health literacy. Taking just 3 minutes to administer, the NVS assesses math, reading, and comprehension skills as well as abstract reasoning. Most importantly, its sensitivity was as great as the TOFHLA's for identifying those with inadequate health literacy.16 Initial testing was conducted on a small sample from university-affiliated primary care practices with few male patients (8%). These populations may not represent most primary care offices.17
The purpose of this study was to determine the acceptability and timeliness of using the NVS to measure health literacy in various suburban, urban, and rural primary care settings. A secondary purpose was to determine the influence of taking a health class on one's level of health literacy.
Methods
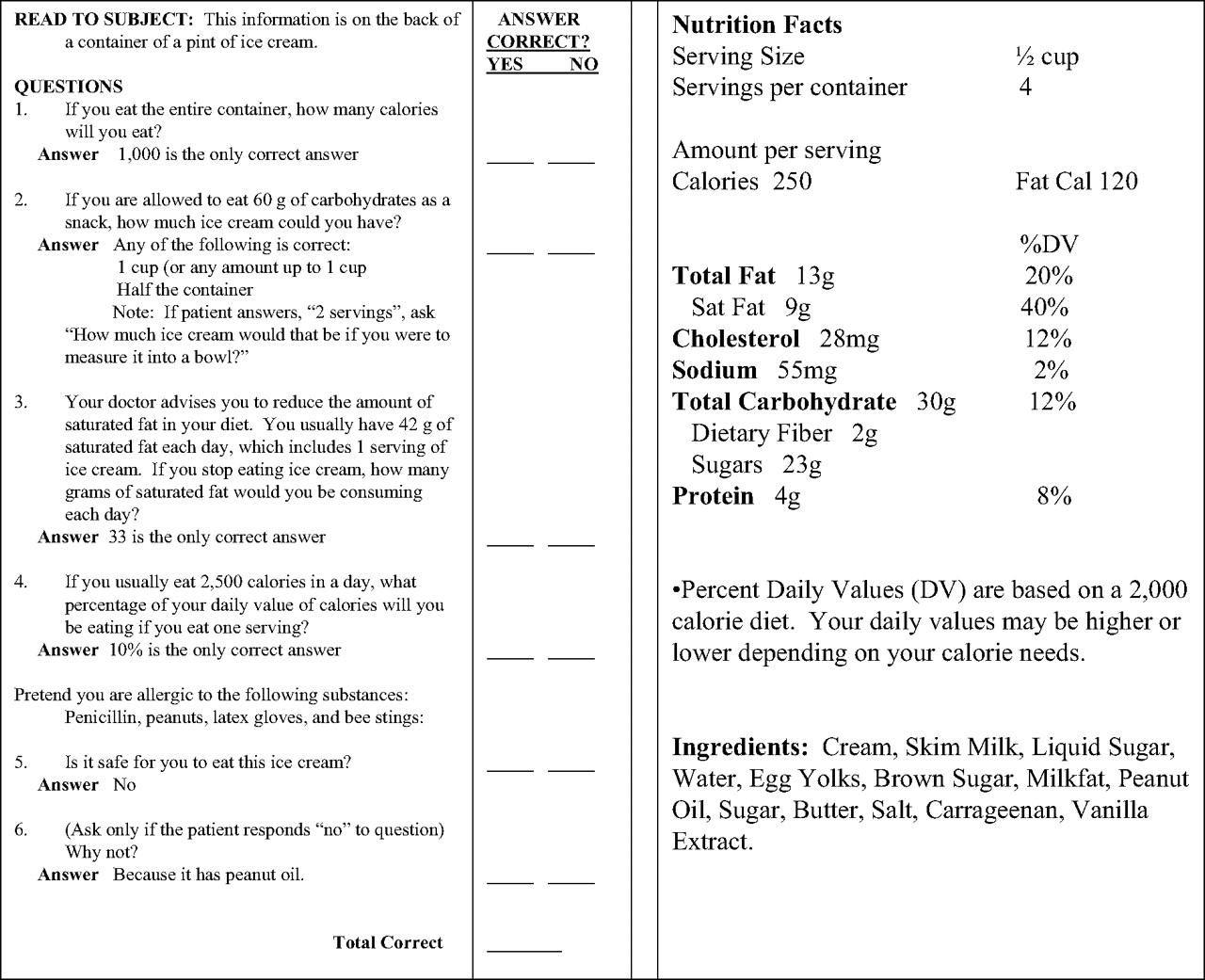
St. John Hospital Institutional Review Board approved this cross-sectional study. The principal investigator (LCS) or a trained research assistant recruited participants. Demographic information—including the patient's stated age, gender, height, weight, smoking status, highest level of education, perceived health status, and whether the patient had ever taken a health class—was collected first. The NVS was then administered (see Figure 1). The NVS uses an ice cream nutrition label that the patient holds and reviews; then, 6 questions based on that nutrition label are given orally. Four or more correct answers indicate adequate literacy; 2 to 3 correct answers indicate limited literacy is possible, and 0 to 1 correct answers indicate limited health literacy is likely.
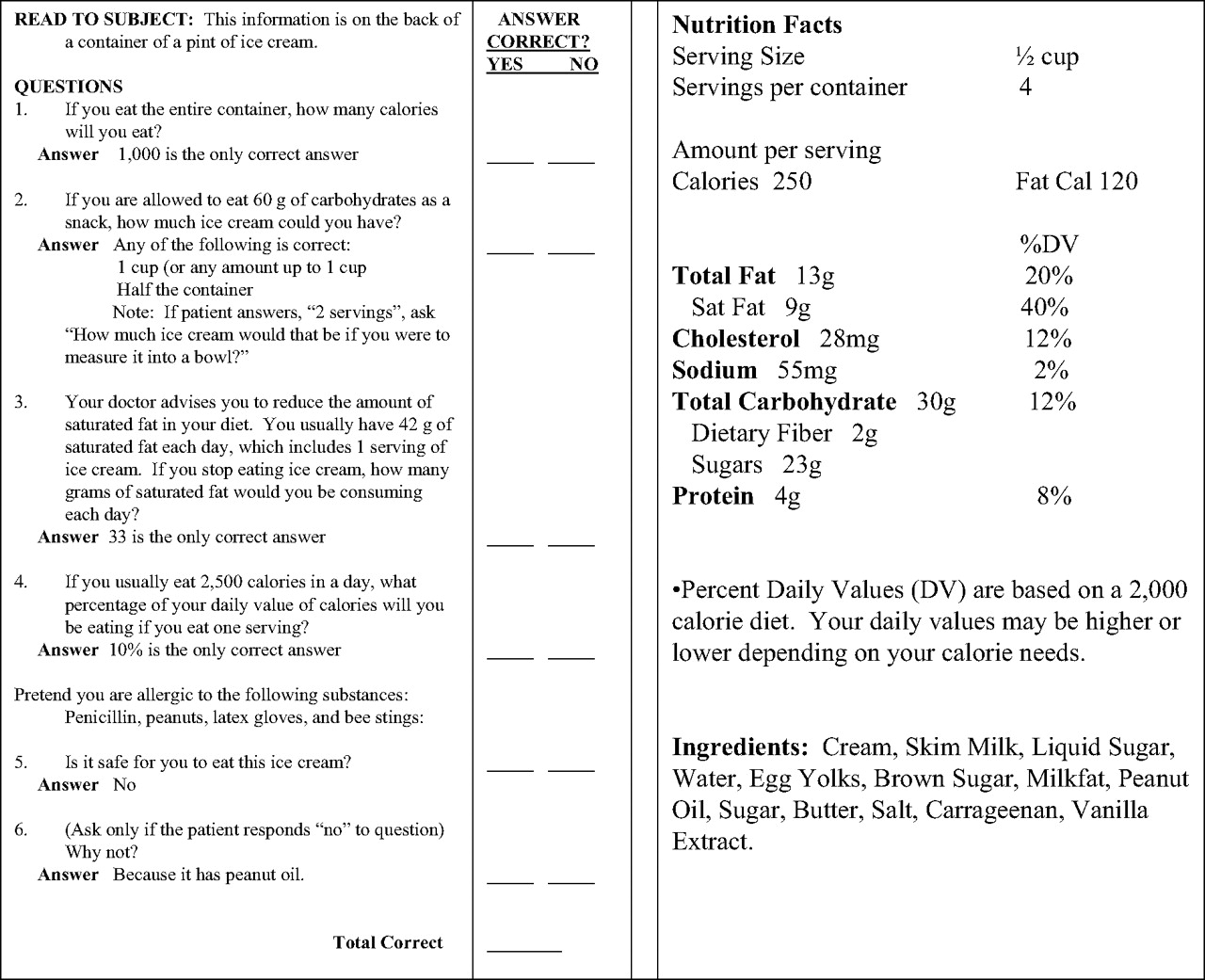
Tester verbally administers the questions on the left. The patient holds and uses the ice cream nutrition label on right to answer 6 questions. (NVS screening tool originally printed by Weiss, et al16 in 2005.) Reprinted with permission from “Quick Assessment of Literacy in Primary Care: The Newest Vital Sign, ” November/December 2005, Annals of Family Medicine. Copyright © 2005 American Academy of Family Physicians. All Rights Reserved.
The NVS was administered to approximately 200 patients at each of 5 primary care sites: 2 suburban family medicine clinics, a rural family medicine clinic, an urban community health clinic, and during preparticipation sports physicals among middle- and high-school athletes in suburban areas. Fifty participants were timed as they were given the test, and all refusals were logged throughout the study at all sites. Any patient ≥13 years of age was eligible for inclusion. Exclusion criteria included any individuals with organic brain disease or mental handicap, patients younger than 13 years, those unable to read English, and patients unable to see the nutrition label. At the 4 clinical sites, qualified, agreeing participants were tested one-on-one in a private setting before being seen by the physician.
Statistical Analysis
The χ2 test was used to compare rates of adequate health literacy for gender, educational level, smoking status, body mass index (BMI) classification, ethnicity, age (by decade), perceived health status, and whether individuals had taken a health class. Analysis of variance (ANOVA) compared age and BMI by literacy level. Logistic regression was also used to find predictors of health literacy (adequate or not adequate). P < .05 was considered significant.
Results
A total of 1014 participants were equally distributed between the 5 sites. Only 29 individuals declined (response rate, 97.5%). The average time to administer the test was just 2.6 minutes.
We detected differences between the middle- and high-school athletes and the adults evaluated at clinics and found an interaction between race and gender; therefore, results are presented for each group. The mean age (± SD) of adult participants (n = 808) was 44.9 ± 15.0 years (range, 18 to 91); men comprised 34.2% of the group (n = 274). Educational distribution revealed that most adults were high school graduates or had at least some college (88.8%). Whites were the most represented race (68.8%), followed by African Americans (28.5%), Hispanics (1.5%), and other (1.2%). The mean BMI (± SD) was 29.7 ± 7.3 (range, 12.9 to 62.8). Overall, inadequate health literacy was detected in 51.9% of adults.
The mean age (± SD) of middle- and high-school athletes (n = 206) at preparticipation health physicals was 15.0 ± 1.3 years (range, 13 to 20); boys comprised 53.4% of the group. Whites were the most represented race (90.8%). The mean BMI was 22.3 ± 3.8 (range, 15.6 to 37.4). Overall, inadequate health literacy was detected in just 40.3% of these athletes.
As shown in Table 1, more women than men had adequate literacy, regardless of race, with white women the most likely to have adequate literacy and non-white men the least likely to have adequate health literacy. For the rest of the variables in Table 1, only adults showed differences. More adults who never smoked or quit >5 years ago had adequate literacy than those who did not, and health literacy increased with education. Self-reported health status was rated as excellent or very good by 39.9% of those with adequate literacy whereas only 27.8% of adults with less-than-adequate literacy rated their health this highly. A fair or poor self-rating was given by just 15.9% of those with adequate literacy, but 31.1% of those with less-than-adequate literacy chose this category.
Proportion of Patients with Adequate Health Literacy*
As shown in Figure 2, health literacy decreased with advancing decades (P < .0005). The mean age (± SD) of adults likely to have low health literacy was 53.3 ± 15.2 years; of those with possible low health literacy, 45.9 ± 15.4 years; and of those with adequate health literacy, 40.0 ± 12.5 years (ANOVA; P < .0005).

Health literacy decreases with age. Age by decades is plotted against adequate health literacy. The youngest participant was 13; the oldest was 91. There was a significant effect of age category on health literacy (χ2 P < .0005). Total number of patients in each age bracket is shown within each bar.
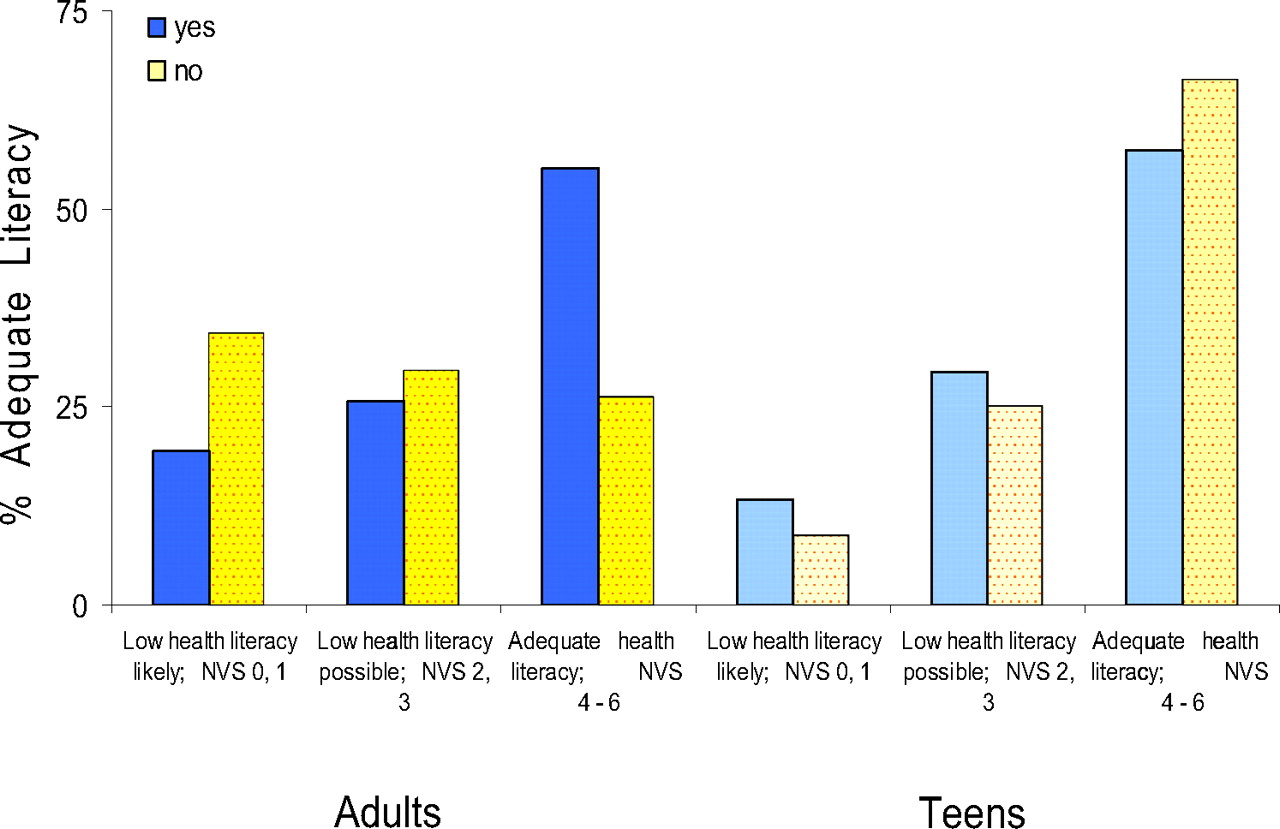
Just more than half of adults (55.1%) and middle- and high-school students (57.3%) had taken a health class. A higher percentage of adequate health literacy (55.1%) was observed for the adults who had taken a health class in school than for those who had not (36.3%) (χ2; P < .0005; see Figure 3). BMI for adults likely to have low health literacy was 29.9 ± 7.8 kg/m2; BMI for those adults with possible low health literacy was 29.7 ± 7.2 kg/m2 and 29.5 ± 7.3 kg/m2 for those with adequate health literacy (ANOVA; P = .871). The proportion of adults demonstrating adequate health literacy in each of the 6 World Health Organization BMI categories did not differ (χ2; P = .509); this is plotted for adults and high-school athletes in Figure 4.

A higher percentage (55%) of adults having adequate health literacy had taken a health class in school (left; n = 800; χ2 P < .0005), but this relationship was not true for teens still in school (right; n = 206; P = .485). Having taken a health class in school was a predictor in the logistic regression analysis for adults but not for teens. NVS, Newest Vital Sign.
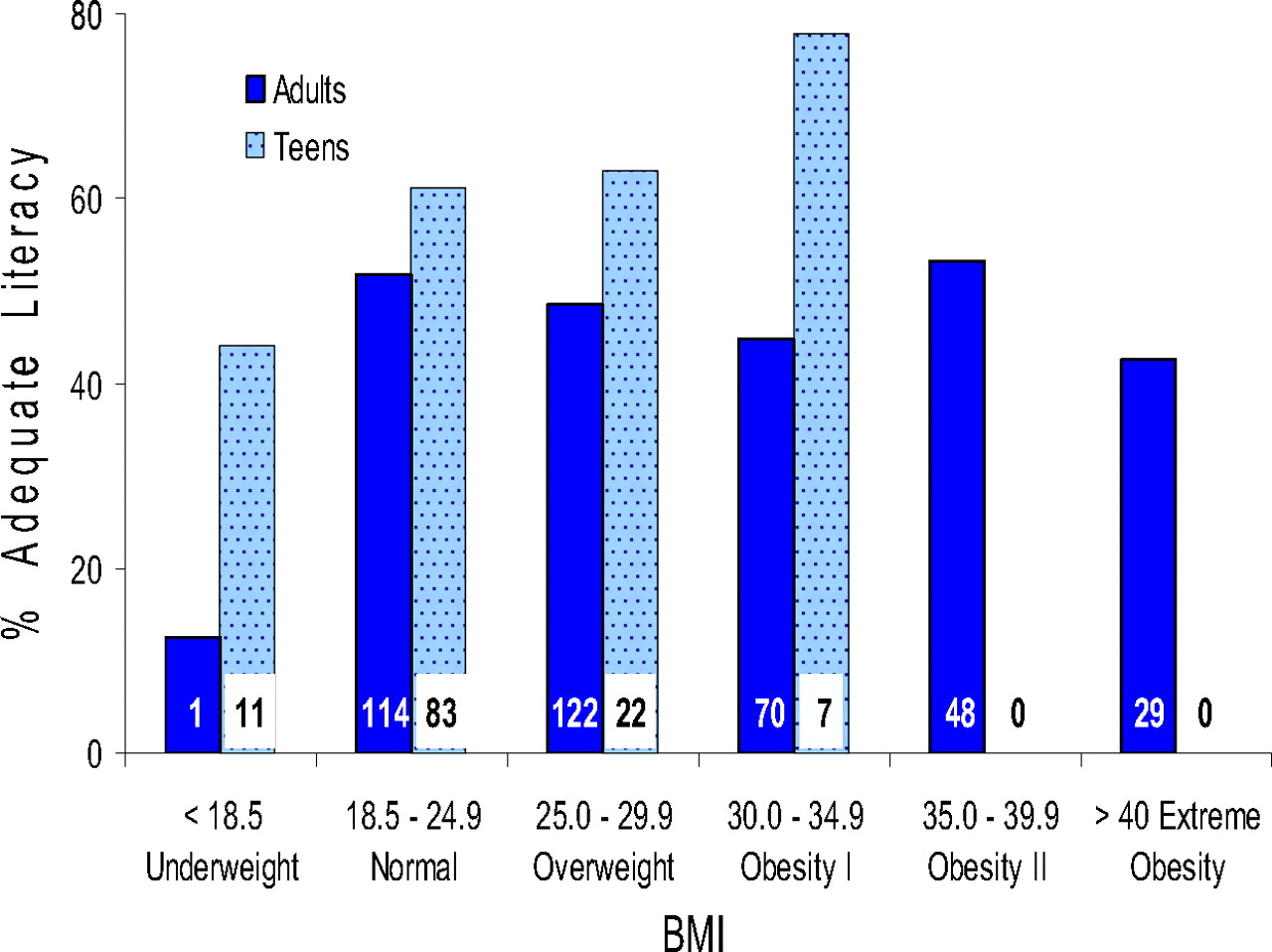
Body mass index, categorized using World Health Organization criteria, is depicted against adequate health literacy for adults (solid bars) and teens (dotted bars). There was no association of BMI with health literacy level among either group when evaluated by analysis of variance (P > .05) or BMI category (χ2 P > .05). However, BMI category was the fourth of 5 predictors in the logistic regression analysis for adult participants (odds ratio, 1.040; 95% CI, 1.016–1.065) and second of 2 predictors among teen athletes (odds ratio, 1.087; 95% CI, 0.999–1.182). The number within each bar represents the number of patients with adequate literacy per group. No teen athlete fell in the Obesity II or Extreme Obesity BMI categories.
From the logistic regression, significant predictors of adequate health literacy are shown in Table 2, with odds ratio and 95% CI values reported for adults and middle- and high-school athletes. For both age groups, the significant negative predictor of health literacy was gender × race and the positive predictor was BMI. For adults, positive predictors additionally included more advanced education, younger age, and participation in a health class. We also examined which items of the NVS were most often answered correctly. Table 3 shows the percentage correct for each of the 6 NVS questions. The proportion of adults and teens correctly answering the question about calories in the entire ice cream carton (question 1) was not different; however, for every other question, young athletes scored better than adults. Interestingly, the most often missed items among adults and youth involved more complex mathematics (questions 3 and 4, respectively).
Variables Predicting Adequate Health Literacy in Logistic Regression Analysis
Correct Response Percentage for Adults and Young Athletes
Discussion
Our 51.9% adult inadequate health literacy rate is consistent with the 1993 and 2003 US Department of Education Adult Literacy Studies,18,19 which reported 34% to 51% of American adults had low levels of health literacy. The findings from our sample, the participants whom were evaluated with the NVS, also agreed with those first described by the NVS creators16 and with results using the TOFHLA.9 That health literacy decreases with advancing age (Figure 2; χ2; P < .0005; advancing age was the second strongest variable entered in the logistic regression) has been reported in several studies.9,11,20–24 Among the elderly, deficits in health literacy could occur as a result of declining cognitive function, increased time since formal education, and decreased sensory abilities.3,25,26 Clearly, health care providers need to make an extra effort with elderly patients to insure they understand the health information being conveyed.
Fewer years of formal education also was associated with less than adequate adult health literacy (Figure 3 and Table 2), a finding that is consistent across differing assessments.14,20–23,26–29 Although the association is strong, education should not be assumed to act as a surrogate for health literacy; in our study 37.6% of adults with at least some college education had limited literacy. In particular, a higher percentage of adequate health literacy was observed among the adults who had taken a health class, although this association was not seen among teens. Adults seemed to derive continuing benefit from their health class experience. Because teens are exercising their cognitive abilities daily and the NVS requires math skills for success, the benefit of a health class may have been obscured.
Gender/race was clearly associated with health literacy in our sample. More than 60% of white women had adequate health literacy whereas <25% of non-white men were in that category (Table 1). Although a gender effect has been detected less often,23,25,28,30 race has been consistently reported to affect health literacy.20–22,24,28,29 It is possible that the effect of race is so strong in some studies that it swamped any effect of gender. It has been proposed that the lower health literacy rate among non-whites may be related to the underserved status of minority participants.31
Although BMI was not associated with health literacy in univariate analysis, BMI was the fourth of 5 variables entered into the logistic regression equation for adults and the second of 2 variables entered for middle- and high-school athletes (Figure 4). In the majority of previous studies, no association was reported between BMI and health literacy. Having taken a health class was the last predictor variable for adults. The recognition of need for a functionally health literate population prompted the initiation of required health classes in school,32 and among our participants, this seemed to have a positive long-term effect (Figure 3). The decline in health literacy with age and time elapsed since formal education suggests that practitioners need to check for understanding more frequently as their patient population ages.
Self-reported health status has been shown to correlate with patient morbidity, and other researchers have described an association between health status and health literacy.20,28 Our patients’ self-reported health status was significant in univariate but not multivariate analysis. It is probable that any influence of reported health status was absorbed by the age variable because health status declined with age (excellent or very good, age 31.8 ± 18.0 years; good, 42.8 ± 16.6 years, fair or poor, 46.8 ± 14.6 years; P < .0005).
Few participants refused to take the NVS (2.5%), which indicates that this tool is acceptable to patients. Previous studies found similar acceptability.33,34 The NVS was administered, on average, in less than 3 minutes, which demonstrates the utility of the NVS in primary care and which is consistent with prior findings.35 The NVS would not be administered during every patient visit, but our data suggest that periodic reassessment should prove helpful to target patient-provider communication appropriately.
Limitations
There were several limitations to this investigation. The entire sample was recruited from sites in southeastern Michigan, which may have limited the generalizability of our findings. It does, however, add to similar investigations that tested the NVS in other areas of the country. Secondly, the sample was recruited in health-related settings, so participants may be more familiar with health-related materials (including nutrition labels) than is the general public. Effort was made to recruit consecutive patients based on the availability of a research assistant. A small percentage of patients may have been missed, which leaves the possibility of selection bias. Lastly, a “gold standard” was not used to compare the NVS with a more tested instrument, but the original developers of the NVS have demonstrated good reliability with the S-TOFLHA.15
Conclusion
Our results underline that health literacy is affected by many factors including age, education, race, gender, and, among adults, taking a health education class.1 The NVS is an accurate, objective, easy-to-administer, and well-accepted measure that estimates health literacy in approximately 3 minutes. Time required to administer the NVS could be offset by the time saved on call-backs from patients and pharmacists because of poor understanding of diagnosis or medications. The NVS may also be particularly helpful for new patients with chronic medical conditions. Information obtained can help determine the appropriateness of patient education handouts and possibly the need for intensive patient education by ancillary staff. Future research about the effectiveness of intervention when inadequate health literacy is identified is the next logical step.
Notes
This article was externally peer reviewed.
Funding: Funding was provided by the St. John Hospital Departments of Graduate Medical Education and Biomedical Investigation, Detroit, MI.
Prior presentation: Poster presentation during the American Academy of Family Physicians Scientific Assembly, Chicago, Illinois (October 2007); oral presentation during the 30th Annual Michigan Family Medicine Research Day Conference, Brighton, Michigan (May 2007); and poster presentation during the Society of Teachers of Family Medicine Annual Spring Conference, Chicago, Illinois (May 2007).
Conflict of interest: none declared.
- Received for publication December 17, 2007.
- Revision received August 15, 2009.
- Accepted for publication August 21, 2009.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Functional health literacy in a population-based sample in Florence: a cross-sectional study using the Newest Vital Sign
- Heart Failure and Low Health Literacy: Mitigating This Lethal Combination
- Do Subjective Measures Improve the Ability to Identify Limited Health Literacy in a Clinical Setting?
- Peanut Butter and Patient Education
- Brief Health Literacy Screening Items Predict Newest Vital Sign Scores
- Health literacy: A primer for pharmacists
- Time, Costs, and Clinical Utilization of Screening for Health Literacy: A Case Study Using the Newest Vital Sign (NVS) Instrument
- Key Questions and Technology in Clinical Practice