
Abstract
Early disseminated Lyme disease can be difficult to diagnose because of atypical symptoms and physical findings. A clinical diagnosis must be made in the absence of confirmatory serologic testing to allow timely therapy. We report a case of a 69-year-old woman who presents with fever, Horner syndrome, and a 12-cm oval-shaped erythematous macular rash with multiple vesiculopustular eruptions. The patient recovered after appropriate intravenous antibiotics, but serologic testing only confirmed the diagnosis 4 weeks later. This case also describes an unusual complication involving the neurologic system. We illustrate the clinical presentation and review the medical literature. Lyme disease should always be considered in patients from endemic regions with viral-like symptoms or a new rash.
Case Report
A 69-year-old healthy jogger from Baltimore County, Maryland, presented with a 4-day history of right eye pain with progressive drooping of the right upper eyelid (Figure 1). She noted fever and fatigue during the 2 days before presentation although she denied headache, neck pain, diplopia, change in speech, facial palsy, extremity numbness, or weakness.

Ptosis, right eye.
During examination, her temperature was 102°F. The ophthalmologic examination in this patient was suggestive of Horner syndrome, with 3-mm ptosis on the right, a 2.5-mm right pupil, and a 4-mm left pupil. A positive cocaine test showed that the affected right pupil had no dilation to cocaine stimulation compared with normal dilation of the left pupil, confirming the diagnosis of Horner syndrome. Anhidrosis was not noted and the remainder of her neurologic examination was unremarkable.
An ophthalmology consult and magnetic resonance imaging scan were initially scheduled as outpatient studies, but near the end of the visit the patient mentioned a “sunburn” in her groin that she attributed to a recent trip to the beach. She had no recollection of recent tick exposure before the onset of symptoms. On examination, we discovered a 12-cm, well-circumscribed, oval-shaped area of redness with multiple vesiculopustular eruptions in its central region, consistent with an erythema migrans (EM) rash of Lyme disease (Figure 2).

An example of an atypical vesiculopustular variant of the erythema migrans lesion.
Because of the presence of an acute neurologic deficit and a suspicious rash in a previously healthy patient from an area endemic for Lyme disease, a lumbar puncture was also performed. Cerebrospinal fluid (CSF) analysis revealed 2 white blood cells (WBCs; 55% polys, 45% monos); 183 red cells; and a CSF protein level of 35. The peripheral WBC count was 4970 with a normal differential. The only abnormalities on a comprehensive metabolic panel were a mildly elevated aspartate aminotransferase of 78 U/L and an alanine aminotransferase of 69 U/L. Lyme serology was initially negative.
The patient had early Lyme disease based on this clinical presentation, despite the negative Lyme serology. The lack of thrombocytopenia, leukeopenia, anemia, or severe or prolonged fever led to a low clinical suspicion for anaplasmosis or babesiosis. Because coinfections were not indicated, treatment with a 4-week course of intravenous ceftriaxone, 2 grams per day, was initiated without the addition of doxycycline or antiprotozoal therapy. Several hours after the first dose, the patient developed a transient exacerbation of her fever, sweats, and rash. Fortunately, she made a consistent and dramatic improvement over the next several days (Figure 3).

Rash from Figure 2, 2 weeks after treatment.
After 3 weeks of incubation, CSF cultures conducted as part of a research protocol1 grew Borrelia burgdorferi, although blood cultures remained sterile. Her initially negative serum serology to Borrelia burgdorferi, converted to positive when repeated 4 weeks later. The Horner syndrome slowly and completely resolved over the subsequent 2 months.
Discussion
Early Lyme disease is a clinical diagnosis in endemic areas in patients presenting with the EM lesion, predominately during the months of May through August. In this scenario, serologic confirmation is unnecessary and can be misleading because the false-negative rate is as high as 60% in the first 2 to 4 weeks of infection.2 Despite negative Lyme serology, the EM rash in the setting of fever, fatigue, and neurologic symptoms suggested a diagnosis of acute Lyme disease.
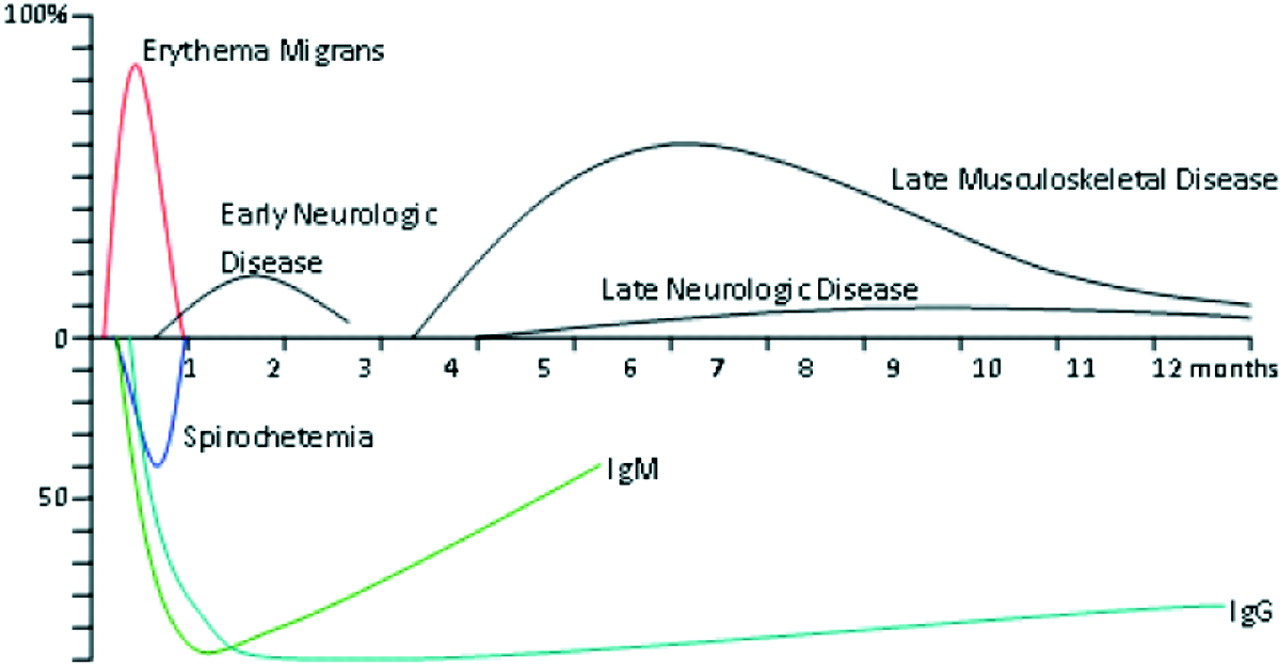
The spirochete B. burgdorferi is the causative agent of Lyme disease in North America, where it is a known cause of acute and delayed musculoskeletal and neurologic disease (Figure 4).3 Approximately 68% of patients with early Lyme disease present with systemic viral-like symptoms, most commonly fatigue, arthralgia, myalgia, headache, fever, and/or chills.4 In the eastern United States the infection is transmitted to humans through the bite of infected Ixodes scapularis ticks, with the majority of cases occurring in patients to whom the tick was attached for more than 36 hours. Early Lyme disease appears after a typical 1- to 2-week incubation period, with a range 3 to 30 days.5
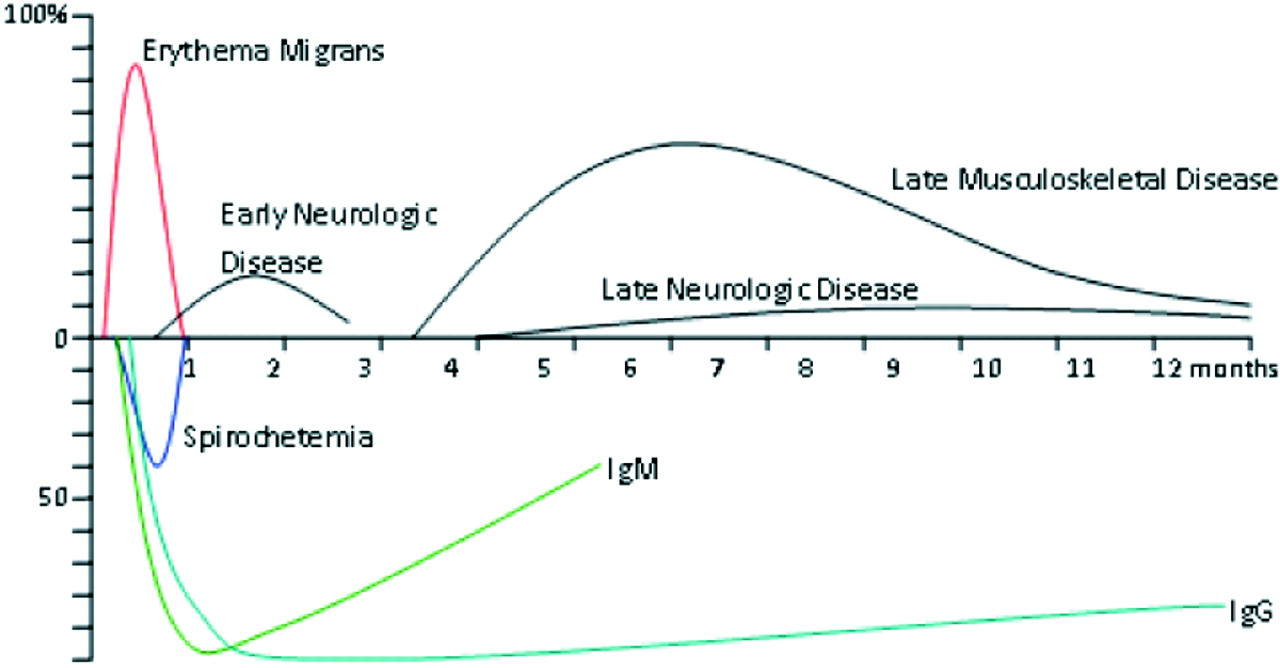
Natural history of untreated Lyme disease.
The patient's “sunburn” was in actuality an uncommon form of the EM lesion. The vesiculopustular component of the patient's rash is an uncommon although well-documented variant of the characteristic bulls-eye lesion found in early Lyme disease (Figure 2). The majority of rashes are uniform in color, with the famous “bulls eye” appearing in only 20% of patients in the United States and the vesiculopustular lesions in 1% to 2% of cases.6,7 EMs may be mistaken for a spider bite when there is a vesicular or necrotic center to the lesion.8 In North America, rashes diagnostically indistinguishable from EM may be caused by Lyme disease or a newly described infection of unknown cause called southern tick-associated rash illness. Therefore, the positive predictive value of EM for Lyme disease is expected to be highly dependent on the prevalence of Lyme disease in a particular geographic region.6 The negative predictive value of EM is poor because no rash is present in up to 10% of patients with early Lyme disease.9,10
The 3 most common early neurologic presentations of Lyme disease are cranial neuritis with 7th nerve palsy, painful radiculitis, and lymphocytic (aseptic) meningitis.11 Other cranial nerves may be involved, producing symptoms of neurosensory hearing loss, vertigo, trigeminal neuralgia, or diplopia. Radiculitis is often misdiagnosed and may mimic abdominal or chest pain syndromes or sciatica. Lyme meningitis may be indistinguishable from viral aseptic meningitis.
Horner syndrome is a rare manifestation of neurologic Lyme, with only 2 cases reported in the literature during the last 19 years.12,13 Other neuro-ophthalmologic or ophthalmologic manifestations of Lyme disease include conjunctivitis, optic neuritis, uveitis, and retinitis. Interstitial keratitis may occur as a later-stage complication.14,15 Lyme disease rarely presents with signs of encephalitis or cerebellar dysfunction, and white matter abnormalities are infrequently seen on magnetic resonance images during acute disease.11
CSF examination shows lymphocytic pleocytosis in cases of Lyme meningitis and in some patients with Lyme-associated early radiculopathies. The “gold standard” for documenting active central nervous system infection is the presence of intrathecal antibody production, manifested by a CSF-to-serum index of antiborellia antibody greater than 1.0.16
Most patients with Lyme disease exhibit a normal peripheral WBC count. The presence of leukopenia, thrombocytopenia, and/or fever greater than 103°F shifts the suspicion from Lyme disease toward anaplasmosis (formerly known as granulocytic Ehrlichiosis).17 The presence of severe anemia should prompt evaluation for babesiosis, an intracellular, malaria-like infection that may be especially severe in patients with a history of splenectomy. If indicated, examination of blood smears may be done for identification of intragranulocytic inclusions for anaplasma or intraerythrocytic protozoa of babesia, although organisms may be absent or few in number. Polymerase chain reaction testing for anaplasma and babesia are considered more sensitive than a visual examination of blood smear, with a 95% sensitivity and 100% specificity of polymerase chain reaction in acute babesia infection.18 Coinfection with any of these organisms, all of which are transmitted by the Ixodes tick, can complicate the clinical picture. Other laboratory abnormalities are uncommon in Lyme disease. Mild elevations of liver function studies occurred in up to 40% of patients in one review of 115 patients.19 These abnormalities are generally transient and should return to normal within a few weeks after treatment.
Doxycycline (100 mg twice daily for 10 to 21 days) is the first choice for therapy for non-neurologic Lyme disease (relatively contraindicated in children younger than 8 and pregnant women). Doxycycline also has the advantage of treating coexisting anaplasmosis.20 Neurologic disease is treated with intravenous ceftriaxone. Studies have demonstrated that a 2- to 4-week course of 2 grams daily is sufficient. In cases with isolated facial palsy without evidence of other neurologic features such as meningitis, recommendations for treatment with oral doxycycline have been made. However, some experts would suggest that lumbar puncture is necessary to rule out coexisting meningitis before initiation of oral therapy.21,16
This patient developed a Jarisch-Herxheimer-like reaction after the initiation of antibiotics. These reactions are characterized by transient exacerbation of symptoms and increased rash secondary to the release of cytokines related to spirochete destruction. This has been reported to occur in approximately 15% of Lyme disease patients and does so within 24 hours of treatment initiation.6
Although antibodies will be present long-term because of the patient's predilection for outdoor activities, this patient is at risk for reacquiring Lyme disease from a future tick bite. Prevention strategies, such as careful inspection of skin surfaces for ticks or rash, protective clothing, and use of repellants were stressed.3
Conclusion
A clinical diagnosis of Lyme disease should be made in the absence of confirmatory serologic testing in the first weeks of infection to allow timely therapy. Any patient from an endemic region who presents with a new rash or viral-like symptoms in the summer months should be considered for the diagnosis. A characteristic bulls-eye rash is actually uncommon and any new rash larger than 5 cm should arouse suspicion for Lyme disease. Intravenous ceftriaxone is preferred if the Lyme disease presents with neurologic symptoms other than isolated facial palsy.
Notes
This article was externally peer reviewed.
Funding: AS's time was supported by a summer internship sponsored by the Lyme Disease Research Foundation of Maryland.
Conflict of interest: none declared.
- Received for publication June 20, 2008.
- Revision received September 24, 2008.
- Accepted for publication September 24, 2008.




{kind=link}
{kind=link}
{kind=link}
{kind=link}