
Article Figures & Data
Figures
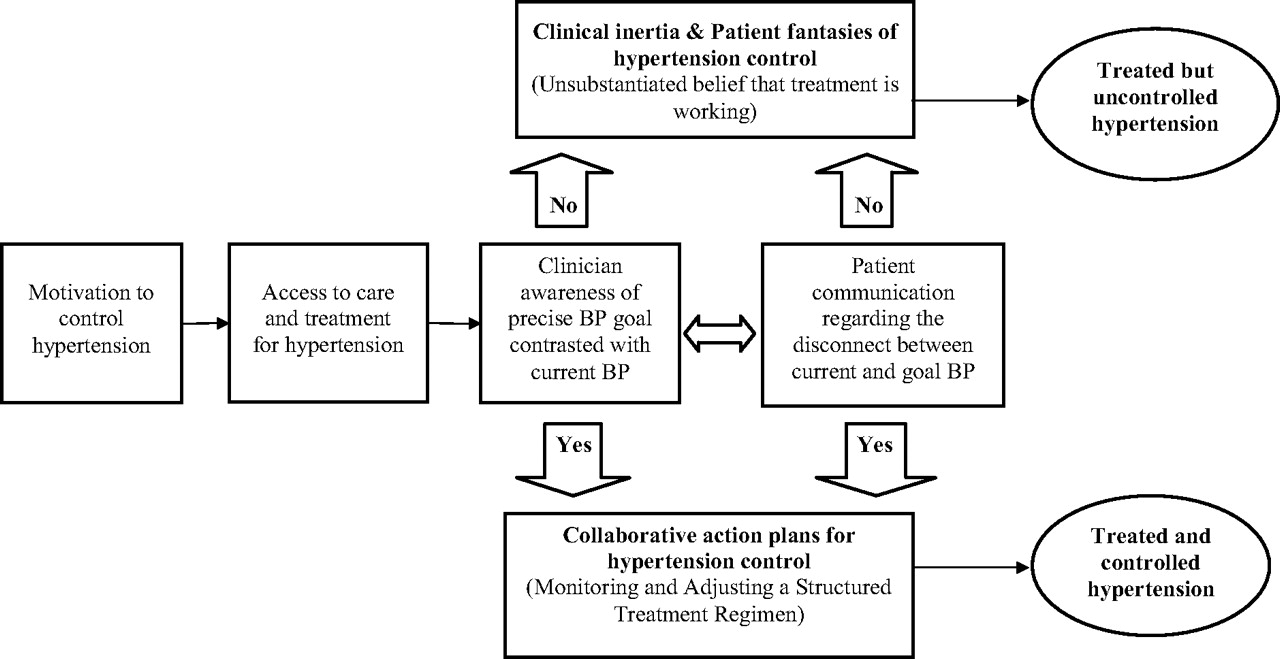
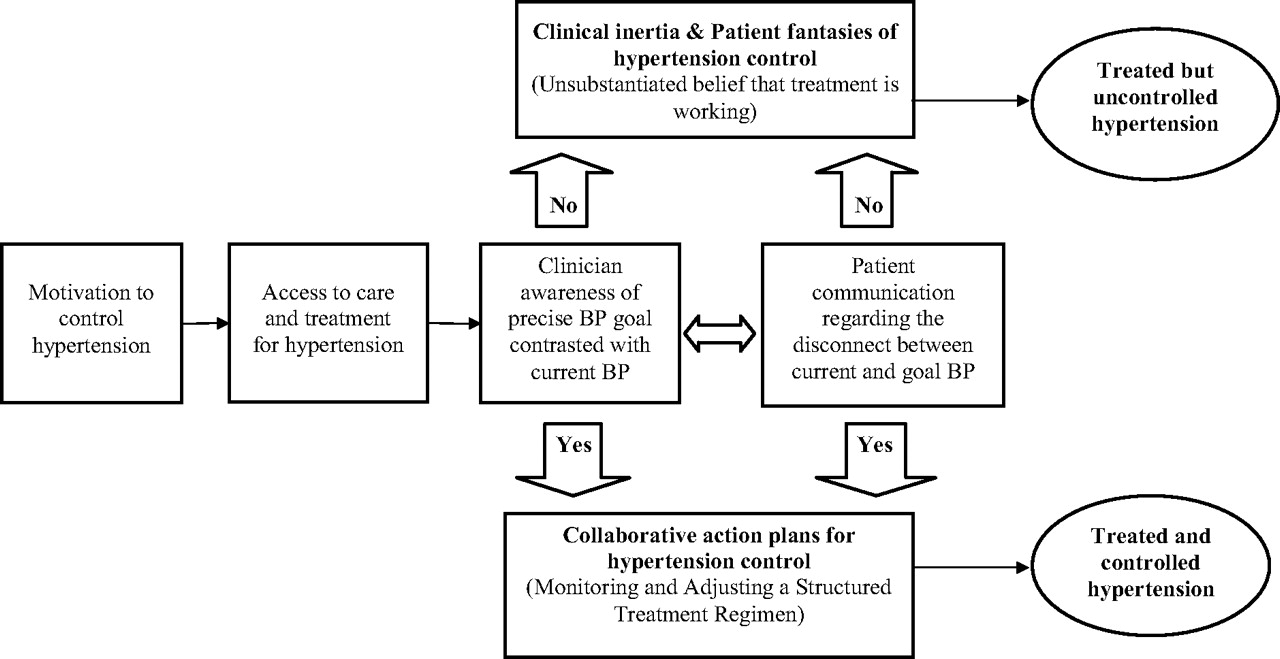
- Figure 1.
The role of collaborative goal setting and action planning to improve the effectiveness of treatment for hypertension control.
Tables
Clinical Trial Principal Maneuver Comparison Maneuver Study Design Eligibility Criteria Enrollment Procedures Primary Outcome 1. SHEP (Systolic Hypertension in Elderly) subgroup18 Chlorthalidone Placebo + Usual Care DB Age ≥60 years, NIDDM, BP ≥ 160/90 IC, RC Stroke 2. SYST-EUR (Systolic Hypertension in Europe Trial) subgroup19 Nitrendipine Placebo + Usual Care DB Age ≥60 years, SBP ≥ 160, controlled DM IC, RC Stroke 3. ALLHAT (Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attacks Trial) subgroup20,21 Chlorthalidone Lisinopril, Amlodipine DB Age ≥55 years, DM, HTN + CV RFs IC, RC Composite CV endpoints 4. CAPPP (Captopril Prevention Project) subgroup22 Captopril Usual Care O-BE Age 25 to 65 years, DM + DBP >100 IC, RC Composite CV endpoints 5. LIFE (Losartan Intervention for Endpoint Reduction in Hypertension Study) subgroup23 Losartan Atenolol DB Age 55 to 80 years, DM, HTN + LVH IC, RC Composite CV endpoints 6. STOP-2 (Swedish Trial in Old Patients with Hypertension) subgroup24 Calcium antagonists, ACE inhibitors Usual Care O-BE Age 70 to 84 years, DM + HTN IC, RC Composite CV endpoints 7. INSIGHT (International Nifedipine GITS Study) subgroup25 Nifedipine GITS Diuretics DB Age 55 to 80 years, DM, HTN + CV RFs IC, RC Composite CV endpoints 8. JMIC-B (Japan Multicenter Investigation for Cardiovascular Diseases) subgroup26 Nifedipine ACE inhibitor O-BE Age 55 to 75 years, DM, HTN + CAD IC, RC Composite CV endpoints 9. IDNT (Irbesartan Diabetic Nephropathy Trial)27 Irbesartan Amlodipine + usual care DB Age 30 to 70 years, DM, HTN + albuminuria IC, RC Composite CV endpoints 10. CONVINCE (Controlled Onset Verapamil Investigation of Cardiovascular Endpoints) subgroup28 Verapamil Usual care DB Age ≥55 years, DM + HTN IC, RC Composite CV endpoints 11. BENEDICT (Bergamo Nephrologic Diabetes Complications Trial)29 Trandolapril Verapamil + placebo DB Age >40 years, DM, HTN + no micoalbuminuria IC, RC,TPP Microalbuminuria 12. INVEST (International Verapamil SR-trandolapril Study) subgroup30 Verapamil Atenolol O-BE Age >70 years, DM, HTN + CAD IC, RC,TPP Composite CV endpoints 13. FACET (Fosinopril versus Ampldipine Cardiovascular Events Randomized Trial) subgroup31 Fosinopril Amlodipine + usual care O-BE Age >60 years, DM + BP≥140/90 IC, RC,TPP Composite CV endpoints 14. NORDIL (Nordic Diltiazam Study) subgroup32 Diltiazam Usual care O-BE Age 50 to 80 years, DM + DBP >100 IC, RC Composite CV endpoints 15. Hypertension in Diabetes Study IV33 Tight BP control Less tight BP control OP Age 25 to 65 years, DM, BP ≥ 150/85 IC, RC Macro/Micro Vascular Complications 16. UKPDS (United Kingdom Prospective Diabetes Study) subgroup34 Tight BP control Less tight BP control OP Age 25 to 65 years, DM + HTN IC, RC Death 17. HOT (Hypertension Optimal Treatment Study) subgroup35 Tight BP control Less tight BP control O-BE Age 50 to 80 years, DM + DBP > 100 IC, RC Composite CV endpoints 18. ABCD (Appropriate Blood Pressure Control in Diabetes Trial)36 Tight BP control Less tight BP control OP Age 40 to 75 years, DM + untreated DBP > 80 IC, RC Diabetic nephropathy 19. Steno-2 Study37 Intensive multi-risk factor control Conventional strategies OP DM + microalbuminuria IC, RC,TPP Macro- or microvascular complications 20. High Risk Patients with Diabetes: A Motivation and Teaching Intervention38 Personalized BP goals Usual care OP Age 45 to 70 years, DM + BP > 140/90 IC, RC,TPP Microvascular complications ACE, angiotensin-converting enzyme; BP, blood pressure; DB, double blinded; O-BE, open, blinded to endpoints; OP, open pragmatic; DM, diabetes mellitus; HTN, hypertension; SBP, systolic blood pressure; DBP, diastolic blood pressure; CV, cardiovascular; RF, risk factors; IC, informed consent; RC, reviewed medical charts; TPP, targeted physician practices.
Co-maneuver Types Co-maneuver Characteristics by Study (Indicated by Reference Number) Frequency of clinic visits Frequent baseline visits:18, 22–31, 35, 36, 38 Every 3 to 4 months: 18–20, 25, 27, 29, 33, 34, 37 Every 6 months: 22–24, 26, 28, 30–32, 35, 36 Annual follow-up only: 38 Activities occurring at each visit Treatment titrated unless BP at target: 18–37 BP measured and compared to target: 18–38 Assessment of study endpoints: 18–38 Feedback given to study clinicians Detailed feedback and decision support: 38 Structured reminders of participants’ status: 20, 30, 33, 34 No additional structured decision support: 18, 19, 22–28, 32, 35–37 Education offered to study participants Counseling, support, and behavior modification education: 37, 38 Structured education at follow-up visits: 18, 21 No structured education: 19, 22–36 Specificity of blood pressure target(s) A specific systolic and/or diastolic BP target: 18, 20–38 Targeted BP change from baseline: 19, 25, 27, 31 Action plan for modification of treatments Action plan explicitly defined: 18–37 Specific medications or medication classes: 18–38 Communication of adverse events from principal maneuver Adverse events discussed at each follow-up: 18–37 Specific adverse events queried: 19, 20–27, 29, 30, 32–37 No published documentation of adverse events: 38 BP, blood pressure.




{kind=link}