
Abstract
Background: The prevalence and nature of sleep disorders in primary care has not been widely studied. As part of a survey conducted in 5 family practice offices in North Carolina, we screened adult patients for sleep syndromes and sought to ascertain which demographic status and health status were associated with these disorders.
Methods: We approached 2963 consecutive adults who presented for office visits to the 5 study practices. The 4-page study questionnaire, which was available in English and Spanish, included items on insomnia, excessive daytime sleepiness, obstructive sleep apnea syndrome, and restless legs syndrome. Analyses evaluated the relationship between sleep syndromes and demographic factors, health status, and disability.
Results: We enrolled 1935 patients (65.3% response rate). More than half reported excessive daytime sleepiness, one third had insomnia, more than 25% had symptoms of restless legs syndrome, and 13% to 33% reported obstructive sleep apnea syndrome symptoms. Participants who rated their health as poor reported significantly higher rates of all sleep disturbance items. Patients with hypertension, pain syndromes, and depression had a significantly increased risk for all sleep complaints. Patients who reported limited activity had a significant risk of restless legs syndrome.
Conclusion: Sleep complaints are highly prevalent in primary care populations. Patients with the highest risk for sleep disturbance are those with pain, mental illness, limited activity, and overall “poor physical and mental health.” Because sleep disorders are associated with a significant health impact, positive responses to questions regarding sleep symptoms should prompt further diagnostic inquiry.
Sleep is an essential restorative physiologic phenomenon, and impaired sleep can have significant negative impact on health. Sleep disorders have been linked to impaired cognition, poor job performance, motor vehicle accidents, and increased health care use.1,2 Sleep disorders are common in adults, especially in the elderly3–5; they include insomnia, excessive daytime sleepiness (EDS), obstructive sleep apnea syndrome (OSAS), and restless legs syndrome (RLS). Because of their impact on quality of life, primary care physicians should be aware of these common sleep disorders.
A considerable proportion of adults (43%) report EDS that interferes with daily activities.6 EDS is generally caused by a sleep disorder or inadequate sleep; in clinical settings, it typically presents as decreased stamina or daytime grogginess.7 EDS carries a risk of increased work-related or motor vehicle accidents. Comorbid conditions, including medical (eg, heart disease and arthritis); psychiatric (eg, depression); and other sleep disorders (eg, OSAS) are important risk factors for EDS. Substance abuse and sedating medications are contributing factors.
Insomnia is characterized by difficulty initiating or maintaining sleep, often leading to EDS. Sleep initiation insomnia is associated with depression or anxiety, stress (“burnout”), or a primary sleep disorder such as RLS. Frequent nighttime awakenings reflect disruption in normal sleep mechanisms and are often caused by medical disorders such as arthritis or primary sleep disorders such as OSAS. Drug or alcohol abuse, caffeine, or shift work can contribute to insomnia.
OSAS is common in the general population. Snoring, gasping for air, or difficulty breathing at night, coupled with EDS and frequent awakenings, are cardinal signs of OSAS. Risk factors include obesity, crowded oropharyngeal airway, older age, male sex, hypertension, and cardiovascular disease.8–10 Because many of these risk factors are more common among primary care patients than in the general population, it is likely that people with OSAS present frequently in primary care settings.11 OSAS leads to an increased risk of vascular disease, such as hypertension. Therefore, recognition and treatment of OSAS is clinically important.
The reported prevalence of RLS in the general population ranges from 2.5% to 15%, with increased prevalence among the elderly. RLS is unpleasant and typically occurs during rest (in the evening or bedtime), with relief provided by rubbing the legs or walking. Patients with RLS have difficulty falling asleep and frequently experience EDS. RLS is also associated with poor general health, depression, end-stage renal disease, pregnancy, iron deficiency, peripheral neuropathies, medications (eg, tricyclic antidepressants or selective serotonin reuptake inhibitors), caffeine, and alcohol.5,12,13
The prevalence and nature of sleep disorders in the primary care population has not been widely studied. Therefore, as part of a survey conducted in 5 family practice offices, we screened adult patients for sleep syndromes and sought to ascertain which demographic and health status factors were associated with the presence of these disorders.
Methods
Data Collection Sites and Study Subjects
This research study was conducted in a practice-based research network consisting of a representative sample of family practices in North Carolina, the North Carolina Family Practice Research Network (NC-FP-RN). Subjects were recruited from 5 primary care sites in North Carolina. Two were rural community health centers, 2 were suburban private practices, and 1 was a university-affiliated practice located in a small town. In each study practice, patient enrollment and data collection were conducted for 1 month. This length of time was chosen to maximize the number of subjects enrolled yet minimizing the number of repeat patients.
During data collection, all patients 18 years of age and older who had an appointment with a physician, physician assistant, or nurse practitioner were eligible to enroll. Eligible subjects were approached before their appointment, and informed consent was solicited using procedures approved by the Committee for the Protection of the Rights of Human Subjects of the University of North Carolina School of Medicine. Consenting subjects could either complete the questionnaire on their own or, if desired, be interviewed by a data collector. Family members who accompanied subjects were permitted to provide assistance. Patients who were acutely ill or did not feel like completing the survey in the waiting room but still wanted to participate were given the survey and a return address envelope.
Measures and Data Collection
The data collection instrument was a 4-page self-report health questionnaire, which was available in both English and Spanish and required 10 to 15 minutes to complete. It included (1) the following demographic and health status items: birth date, height and weight (from which body mass index was calculated), sex, race/ethnicity, smoking status, self-reported health, years of education, and marital status14,15; (2) questions about the presence or absence of heart disease, high blood pressure, lung disease, stroke (or “mini-stroke”), depression, back pain, joint pain, arthritis (including gout, lupus, and fibromyalgia), cancer, and diabetes; (3) self-report items on days of disability because of physical or mental health problems16; and (4) a series of items on sleep-related symptoms, which were modified from existing instruments.17,18
The study's data collection questions about sleep disorders are included as Appendix A. Respondents were screened for EDS with 2 questions: one regarding subjective sleepiness and one regarding dozing off during daytime activities. A question about tingling, creeping, or restless feelings in the legs while trying to sleep was used to screen for RLS. The questionnaire screened for sleep-related breathing disorders and, in particular, OSAS with 2 questions addressing snoring and gasping or apnea during sleep. Sleep maintenance insomnia was assessed with a question regarding the number of nocturnal awakenings. For the questions about EDS, RLS, and snoring, a positive screen was recorded if the symptom was reported at least once a week; for gasping/apnea, a positive screen was recorded if the symptom had been reported 1 or more times in the past month; for sleep maintenance insomnia a response of 3 or more awakenings per night was considered a positive response.
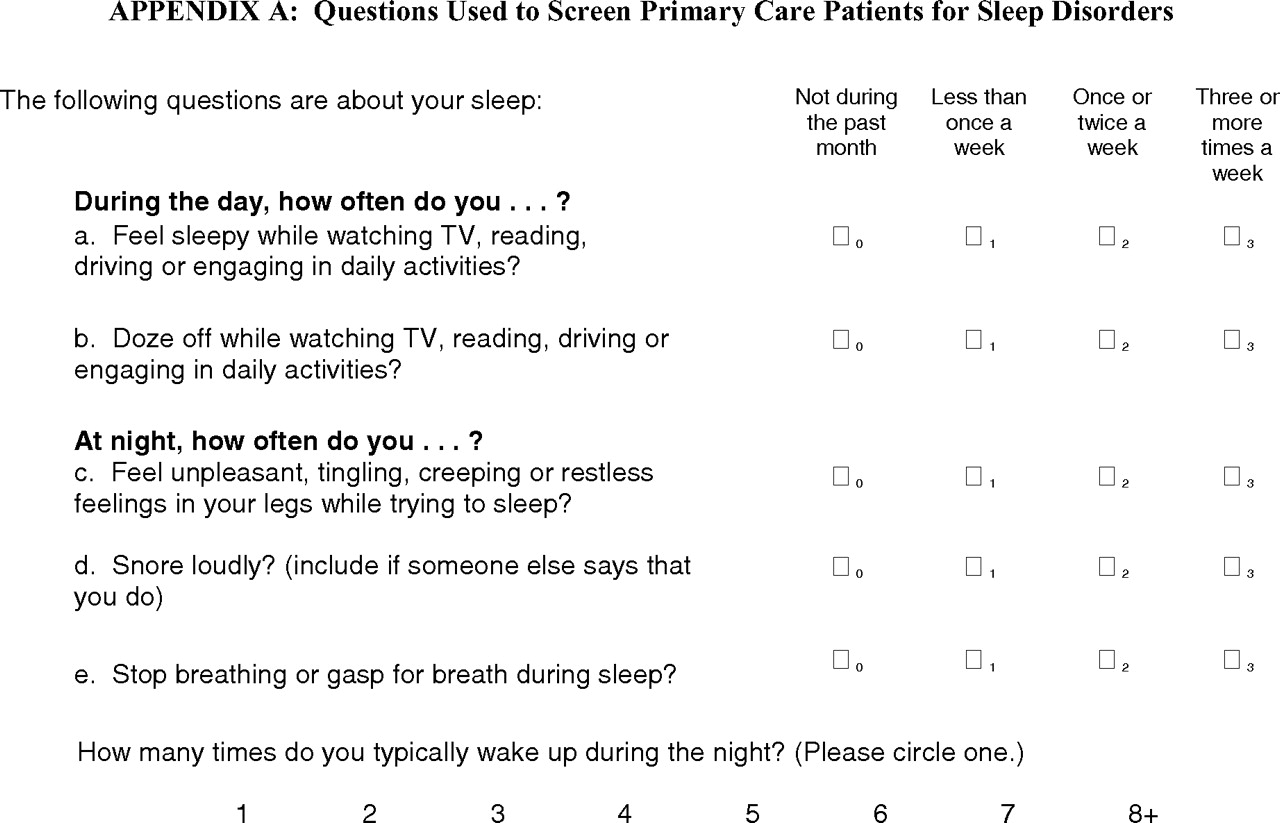
Questions used to Screen Primary Care Patients for Sleep Disorders
Data Preparation and Analysis
Analytic data files were created using SAS software, and all analyses were conducted using SAS/STAT software.19 Descriptive statistics (frequencies and percentages for categorical variables and means ± SDs for continuous variables) were computed for each sleep symptom and for demographic and health characteristics. χ2 statistics and attendant P values were computed for the bivariate comparisons of the demographic and health characteristics and sleep symptoms of older (≥65 years of age) versus younger (<65 years of age) patients. Associations among sleep symptoms were examined using Spearman's correlation coefficient. Odds ratios (ORs) between selected dichotomized demographic and health characteristics and sleep symptoms were computed, with analyses adjusting for age, race (African-American vs other), and sex.
Results
During data collection, 2963 eligible patients presented to the study practices. Of these, 1935 (65.3%) completed all or a portion of the survey and were enrolled. Of the 1935 respondents, 1934 (99.9%) completed the sleep items. This article examines data from these 1934 respondents.
Demographics and Health Characteristics (Table 1)
Demographic and Health Characteristics of Primary Care Patients Studied (N = 1934)
Study participants were 68% female, 58% white, 30% African-American, and 9% Latino. Mean age was 50 years. Approximately 60% were married or living with a partner. The majority had attended some college. More than 30% noted fair/poor health status; hypertension, joint or back pain, depression, diabetes, and heart disease were the most common chronic conditions. Approximately 20% smoked cigarettes. Older participants were more likely to report fair or poor health status, hypertension, lung disease, stroke, cancer, diabetes, arthritis, depression, and bad days because of mental health.
Prevalence of Sleep Symptoms (Table 2)
Prevalence of Sleep Symptoms among Primary Care Patients Studied (N = 1934)
Sleep syndromes were common among study participants. More than half reported experiencing EDS at least once a week, and 37% dozed off during daily activities. More than 25% reported experiencing RLS at least once a week, 33% reported snoring, and 13% reported symptoms of witnessed apnea. More than one third reported insomnia.
The frequency of sleep symptoms varied significantly by age. Older patients reported higher frequencies of daytime dozing. In contrast, insomnia, snoring, and witnessed apnea were significantly more prevalent in younger participants. There was no significant difference in RLS prevalence between older and younger adults.
Correlations between Sleep Disorder Symptoms (Table 3)
Spearman Correlation Coefficients (and P values) between the Sleep Screening Items
Each of the 6 sleep disorder symptoms (sleepy during daily activities, dozing during daily activities, RLS symptoms, snoring, sleep apnea, and sleep maintenance insomnia) were significantly and positively associated with reported overall sleep quality (r ≥ .156 for all symptom pairs). In addition, each sleep disorder symptom was significantly positively correlated with other symptoms of sleep disorders. Correlations between items were modest, however, with the largest correlation (r = .051) being between the number of awakenings and overall sleep quality.
Relationship between Demographic and Health Status Variable and Sleep Disorder Symptoms (Table 4)
Risk Odds Ratio Between Demographic and Health Status Variables and Sleep Disorder Symptoms among Primary Care Patients (n = 1934)
A variety of demographic and health status variables were associated with various sleep symptoms. Older participants were significantly more likely to doze off during daily activities (OR, 1.44) but less likely to report snoring (OR, 0.74); sleep apnea (OR, 0.58); or insomnia (OR, 0.79). Women were less likely to report snoring (OR, 0.54) or sleep apnea (OR, 0.69) but were more likely to experience insomnia (OR, 1.28). Racial differences were also seen. Latinos were less likely than whites to report sleepiness or dozing during daily activities (OR, 0.53 and 0.49, respectively); RLS (OR, 0.46); or snoring (OR, 0.53). After adjusting for age, race, and sex, married participants were more likely to report snoring (OR, 1.52), but less likely to report insomnia (OR, 0.79). Participants with higher education were less likely to report sleepiness or dozing during daily activities (OR, 0.98 and 0.80, respectively); RLS (OR, 0.63); or insomnia (OR, 0.55).
A number of health variables were strongly associated with sleep problems, even after adjusting for age, race, and sex. Participants who rated their health as fair or poor and those with a history of pain syndromes reported significantly higher rates of all 6 sleep disturbance items. Participants with elevated body mass index were more than twice as likely to report snoring (OR, 2.18) and sleep apnea (OR, 2.20) and were significantly more likely to report RLS (OR, 1.23) and insomnia (OR, 1.32). Patients with heart disease did not have a greater risk of snoring or sleep apnea, but were more likely to report sleepiness or dozing during daily activities (OR, 1.45 and 1.81, respectively); RLS (OR, 2.06); and insomnia (OR, 1.57). Hypertensive patients had a significantly increased risk for all sleep complaints. Patients who reported limited activity had a significant risk of RLS (OR, 3.88). Patients with lung disease had a significant risk of sleep apnea (OR, 2.94); insomnia (OR, 2.34); daytime sleepiness (OR, 1.79); and RLS (OR, 2.24). Patients with cancer reported an increased risk of insomnia (OR, 1.48). Smokers were at risk for RLS (OR, 1.87); insomnia (OR, 1.48); sleep apnea (OR, 1.78); and sleepiness during daily activities (OR, 1.31).
Discussion
The results of this survey confirm that sleep complaints are highly prevalent in primary care patients. Depending on the syndrome, the reported prevalence across 5 primary care practices was between 13% and 55%. In contrast, approximately a quarter of randomly sampled adults report dissatisfaction with their sleep.20 Our study provides additional details about the range of sleep complaints, their associated risk factors, and the extent to which they are interrelated than details that have been previously reported. As is demonstrated in Table 4, the likelihood of specific sleep symptoms varies according to sex, ethnicity, age, education, health habits, and comorbid conditions. Patients with the highest risk for sleep disturbance are those with pain, mental illness, limited activity, and overall “poor physical and mental health.” Vascular disease, diabetes, respiratory illness, and smoking confer a smaller but still significant risk. Thus, primary care patients are a select population at high risk for having 1 or more sleep disturbance.11
Chronic back pain, arthritis, and joint pain and stiffness were associated with all of the sleep complaints studied. This finding is consistent with clinical research indicating the connection between pain and sleep disturbance21; however, in these analyses, it is impossible to determine which preceded or caused the other.22 Our analyses also identified increased risk of OSAS in patients with musculoskeletal pain. The cause of this relationship is unclear, but it can be postulated that disability and medications (especially opioids) may contribute to sleep apnea. RLS symptoms were also significant in patients with pain, a finding that mirrors others in the literature.23 Thus, a plan that addresses the sleep complaints as well as the pain can optimize the treatment of pain and improve quality of life.
Mental disorders were significantly associated with sleep complaints, a finding that is consistent with previous reports.24,25 The relationship between depression and sleep disturbance is so strong that it is one of the diagnostic criteria of major depression26; people who are not depressed but who have persistent insomnia are at increased risk of developing depression a year later.24 Our survey also supports previous reports that people with sleep apnea may present to their primary care physicians with depression and that treatment of sleep apnea may ameliorate depression.27 Therefore, patients reporting sleep disturbance need to be thoroughly evaluated for mood disorders.
Vascular disease and respiratory illness both contribute risk to and can be exacerbated by sleep complaints. OSAS is an established independent risk factor for systemic hypertension9,28; it is not surprising that we found associations between hypertension and snoring, sleep apnea, EDS, and frequent awakenings. Similarly, we found heart disease to be associated with symptoms of RLS and EDS; however, we did not observe the previously identified association between heart disease and OSAS symptoms.9 Patients with lung disease showed the most significant risk for symptoms of OSAS, especially for gasping during sleep and EDS. Stroke and diabetic patients also showed significant sleep problems, most notably EDS, frequent awakenings, and symptoms of RLS.
The nonspecific symptoms of EDS and insomnia affected 55% and 34% of respondents, respectively. The prevalence of insomnia reported by other studies has ranged from 19% (for chronic insomnia) to 50% (for occasional insomnia),29 with higher rates being reported among women and people who are unemployed, living alone, and residing in large cities.30 In our study, older age was not associated with insomnia but was linked to EDS, both of which are consistent with a previous report.31
According to Young et al,32 the strongest predictors of OSAS in community-dwelling adults are habitual snoring, loud snoring, and frequent breathing pauses. Snoring and witnessed apnea were frequent among our survey respondents (37% and 13%, respectively), although not more frequently than in a general population survey.33 Previous research indicates that people reporting snoring or witnessed apnea are at 3 to 4 times the risk of having clinically significant sleep apnea.33 However, it is important to note that OSAS would be missed if screening is based solely on these questionnaires because OSAS is a complex disease with a varied constellation of symptoms. Therefore, traditional risk factors might differ in certain populations.34 For example, witnessed apneas and obesity might be particularly insensitive in the elderly.32 The decision by the clinician to proceed with extensive and costly evaluation and treatment for patients who are suspects for OSAS depends on a number of factors that should include the severity of symptoms; associated comorbid conditions (eg, hypertension); and functional impairment. Polysomnography is required for definite diagnosis of OSAS; evaluation by a sleep specialist may help assure diagnostic accuracy and increased compliance with therapy. Treatment includes weight control, CPAP therapy, and, in certain populations, a dental device or surgical intervention.
A third of our subjects reported RLS symptoms. This proportion is slightly higher than the 25% percent prevalence reported by Nichols et al,35 and is considerably higher than the rates of 7.2% and 9% reported in 2 general population surveys.36,37 This discrepancy may reflect that, although relatively common, RLS is often not diagnosed by physicians. In one study from 6 countries, 81% of the 416 respondents with RLS symptoms reported discussing their symptoms with a primary care physician, but only 21 (6.2%) were given a diagnosis of RLS.36 As our study demonstrates, patients with depression, pain syndromes, and vascular disease are at increased risk for RLS and should be questioned for its symptoms. Another under-recognized risk factor for RLS is the use of antidepressant medication,38,39 and ruling out adverse effects of drugs, caffeine, or iron deficiency is part of treating RLS. Pharmacological intervention with dopamine agonists may be required. Given the documented high prevalence of undiagnosed RLS and its responsiveness to treatment, primary care physicians should become more aware of the condition and consider active screening.39
That responses to all sleep disorder screening questions were correlated (Table 3) confirms the finding from previous studies that multiple sleep complaints often coexist in the same patients. However, the modest size of the correlations suggests that the various sleep syndromes tend to be distinct. Thus, when evaluating a patient with a sleep complaint, health professionals should both seek to make a specific diagnosis, evaluate for risk factors, and also screen for related sleep disorders.
As with any screening instrument, the questionnaire used here was designed to identify the prevalence of sleep complaints suggestive of specific diagnoses, such as OSAS or insomnia. Although the questions were modified versions of well-accepted measures, they were not diagnostic, and their sensitivity, specificity, and predictive value in the primary care setting have not been determined against standards, such as polysomnography. As with any effective screening tool, it is likely that not all patients with the symptoms identified would meet diagnostic criteria for specific syndromes, such as sleep apnea or insomnia. Thus, positive responses to such items should be the beginning of diagnostic inquiries. Subsequent activities should depend on the history of symptoms and their effect on everyday function. Evaluation should seek to identify modifiable health and mental health issues and other factors such as medications. Thus, effective management of sleep complaints involves screening, diagnosis, the search for and treatment of risk factors, and the identification and treatment of specific syndromes, such as RLS or OSAS.
Acknowledgments
The NC-FP-RN Study is jointly sponsored by the Department of Family Medicine, the Thurston Arthritis Research Center, and the Cecil G. Sheps Center for Health Services Research at the University of North Carolina at Chapel Hill, in collaboration with the North Carolina Academy of Family Physicians. The project co-directors are Leigh Callahan, PhD, and Philip Sloane, MD, MPH. Participating family practices have included: Biddle Point Health Center, Charlotte; Bladen Medical Associates, Elizabethtown; Black River Health Services, Atkinson and Burgaw; Blair Family Medicine, Wallace; Chatham Primary Care, Siler City; Community Family Practice, Asheville; Cornerstone Medical Center, Burlington; Dayspring Family Medicine, Eden; Goldsboro Family Physicians, Goldsboro; Henderson Family Health Center, Hendersonville; North Park Medical Center, Charlotte; Orange Family Medical Center, Hillsborough (pilot site); Person Family Medical Center, Roxboro; Pittsboro Family Medicine, Pittsboro; Prospect Hill Community Health Center, Prospect Hill; Robbins Family Practice, Robbins; South Cabarrus Family Physicians, Harrisburg, Concord, Mt. Pleasant, and Kannapolis; Summerfield Family Practice, Summerfield; and Village Family Medicine, Chapel Hill. Activities of the NC-FP-RN Study and North Carolina Health Project (NCHP) have been supported by the Centers for Disease Control and Prevention, the Agency for Health Care Research and Quality, the National Institutes of Health, and the Department of Family Medicine and the Program on Health Outcomes at University of North Carolina at Chapel Hill. Special thanks is also extended to Lauren Cohen, MA, for her expert assistance in manuscript editing.
Notes
This article was externally peer reviewed.
Funding: This research study was conducted in a practice-based research network consisting of a representative sample of family practices in North Carolina, from which a cohort of patients has been enrolled and is maintained longitudinally. The network is called the North Carolina Family Practice Research Network (NC-FP-RN), and the cohort is called the North Carolina Health Project (NCHP) cohort. The NC-FP-RN and the NCHP are jointly sponsored by the Department of Family Medicine, the Thurston Arthritis Research Center, and the Cecil G. Sheps Center for Health Services Research at the University of North Carolina at Chapel Hill (UNC-CH), in collaboration with the North Carolina Academy of Family Physicians. Activities of the NC-FP-RN and NCHP have been supported by the Centers for Disease Control and Prevention, the Agency for HealthCare Research and Quality, the National Institutes of Health, the Department of Family Medicine at UNC-CH, and the Program on Health Outcomes at UNC-CH.
Conflict of interest: none declared.
- Received for publication September 1, 2006.
- Revision received January 8, 2007.
- Accepted for publication January 16, 2007.
References




{kind=link}
Jump to section
Related Articles
Cited By...
- Prospective Study of Restless Legs Syndrome and Coronary Heart Disease Among Women
- Identification by Primary Care Clinicians of Patients with Obstructive Sleep Apnea: A practice-based research network (PBRN) study
- Identifying Patients at Risk for Obstructive Sleep Apnea in a Primary Care Practice
- Alcohol and Sleep Problems in Primary Care Patients: A Report from the AAFP National Research Network
- Psychosocial Correlates of Insomnia Severity in Primary Care
- Associations Between Subjective Night Sweats and Sleep Study Findings