
Article Figures & Data
Figures
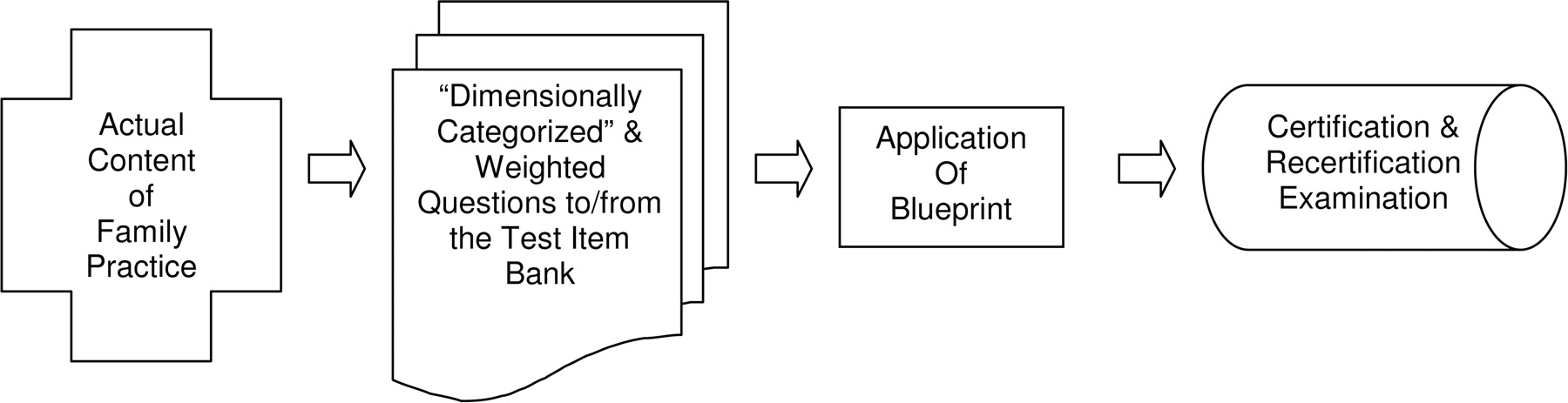
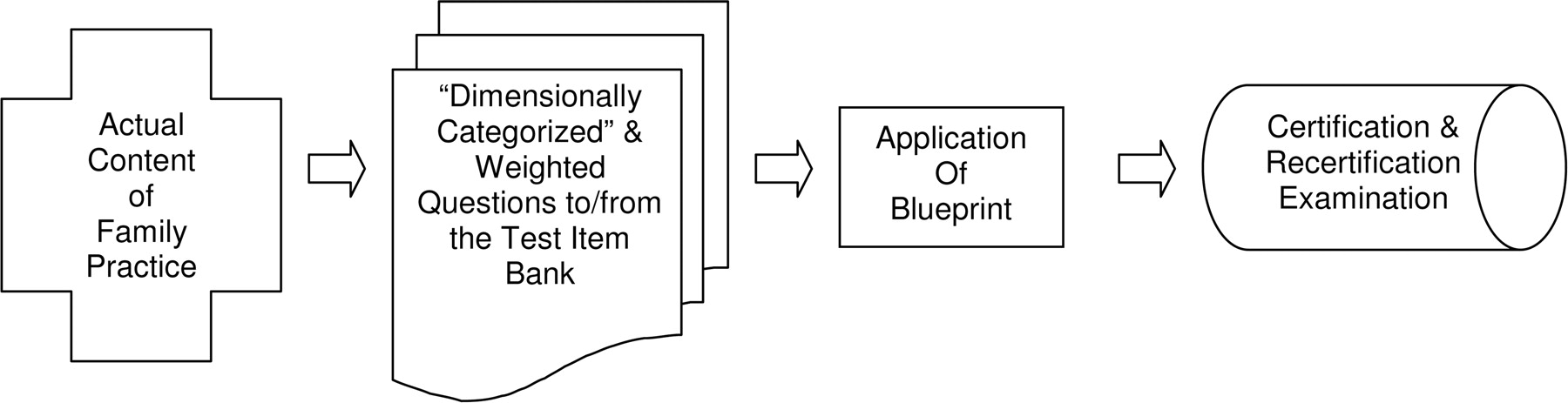
- Figure 1.
Conceptual diagram of the application of a content-based blueprint.
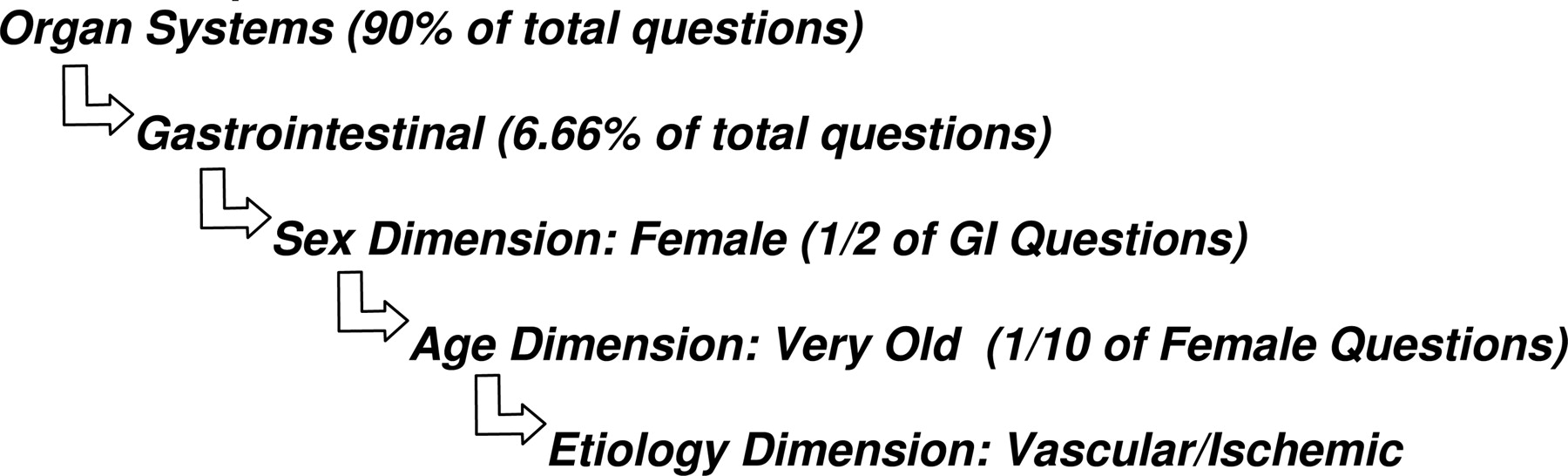
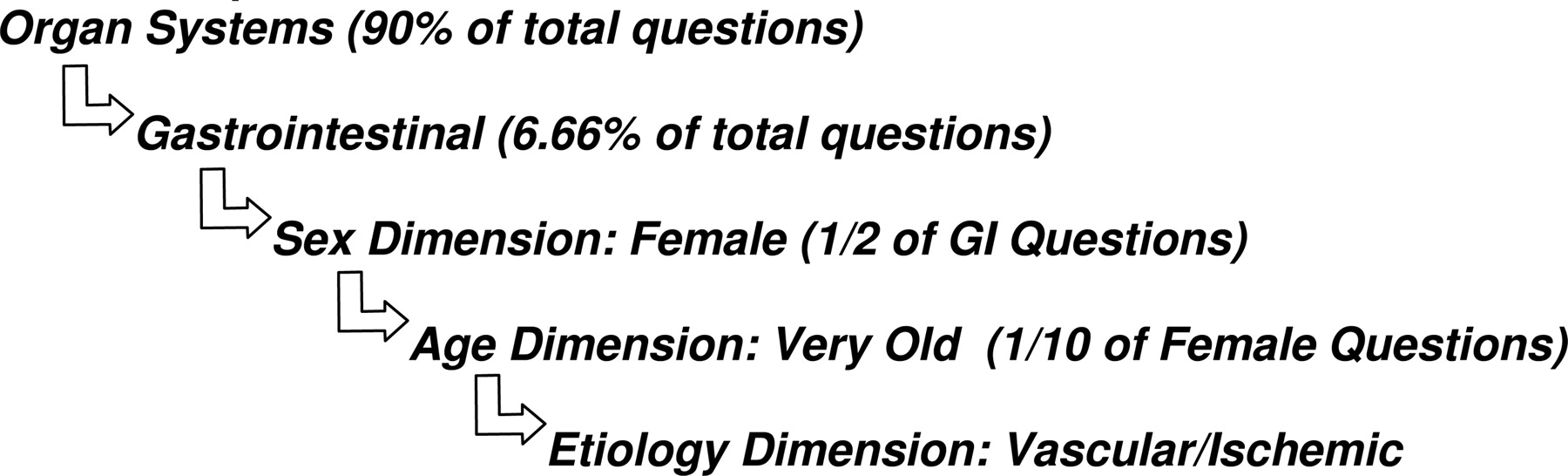
- Figure 2.
Example of use of the blueprint to select a question based on content of practice data.
Tables
General Medical Discipline Percentage of Representation Internal medicine 36 Surgery 6 Obstetrics 7 Community medicine 9 Pediatrics 13 Psychiatry 7 Geriatrics 12 Gynecology 10 Term Definition Classical test theory A theory about test scores, which postulates that a person’s test score can be modeled as the sum of two unobservable variables, a true score and an error score where with certain assumptions a true score can be shown to be the expected score across parallel test forms. A limitation of the classical test theory model is that both person scores and item statistics are dependent on the test and the sample of examinees, respectively. Item response theory A modern statistical theory for test development and scoring that improves the understanding of both individual and item performance. It is based on the concept that both test items and individuals can be simultaneously described in terms of their standing on, or relationship to, one or more ability/knowledge level scales. An individual is characterized by his or her position on the scale, and an item can be characterized by the point on the scale indicating the trait or ability level at which a person would have a 50% chance of responding correctly to the item. Examination blueprint A table of specifications based on the knowledge domain of family medicine, which is weighted by a judged frequency of use and clinical importance. It is used to determine the scope and depth of material covered in the examination process. Equating A statistical process by which the score scale on one test is converted to the score scale of another test so that the scores are equivalent or parallel. Certifiably competent A description of a candidate who has scored at or above the cut score level on a certification examination. Cut score A specified point on a score scale at or above which a candidate passes and below which a candidate fails. Dimensions/orders A categorization of the domain of knowledge in family medicine, which serves as an organizing agent for the content blueprint. Adaptive testing A sequential form of testing in which the order of items presented is determined by the examinee’s response to previous items. Age dimension Etiology/origin dimension Fetus Autoimmune/allergic Newborn Behavioral/lifestyle/cognitive Infant Degenerative Child Environmental Adolescent Genetic Adult Iatrogenic Young Idiopathic Middle aged Infectious Senior Neoplastic Old Nutritional Very old Pregnancy Sex/gender dimension Toxicologic Male Traumatic Female Undifferentiated Populations dimension Vascular/ischemic Immigrant/refugee Anatomic/obstructive/surgical Ethnicity/race Normal Disabilities Anatomy Gay/lesbian/bisexual/transgender Physiology Socioeconomic Growth and development General Diagnosis and management dimension Continuum of care dimension Diagnosis Prevention History Primary Physical Secondary Laboratory Emergent Imaging Acute Diagnostic procedure Chronic Other Early Management Advanced Pharmaceutical Procedural/surgical Behavioral/psychotherapy Complimentary and alternative medicine Other N Mean SD Relative Percentage of Practice 2004 2003 Cardiovascular system 807 4.28 0.943 16.7 17.0 Musculoskeletal system 807 3.66 0.895 12.2 13.0 Respiratory system 807 3.59 0.815 11.7 10.8 Psychogenic (mental health/behavior) 807 3.46 0.953 10.7 11.3 Endocrine system 807 3.34 1.034 9.8 8.0 Gastrointestinal system 807 3.29 0.720 9.5 10.4 Reproductive, female 807 2.75 1.048 6.1 5.3 Integumentary system 807 2.58 0.724 5.3 5.5 Nephrological/urological 807 2.39 0.607 4.4 4.7 Neurological system 807 2.35 0.615 4.2 4.0 Nonspecific 807 2.20 0.935 3.4 3.5 Hematological/immunological 807 2.14 0.521 3.1 2.4 Sensory system 807 2.09 0.548 2.9 2.4 Reproductive, male 807 2.04 0.523 2.6 1.7 Total 807 100.0 100.0 * Higher scores indicate higher frequency of exposure to issue.
N Mean SD Evidence-based practice 807 2.07 1.049 Quality improvement 807 2.59 0.884 Geographic (urban/rural) 807 2.82 1.065 Informatics 807 3.04 1.075 Health policy 807 3.09 0.941 Legal 807 3.13 0.893 Epidemiology 807 3.27 0.852 Biostatistics 807 3.52 0.801 Bioterrorism 807 3.88 0.414 * Lower scores indicate higher frequency of exposure to issue (1 = daily, 2 = weekly, 3 = monthly, 4 = almost never)
- Table 6.
Patient-Based Care and Systems Issues: Highest to Lowest Strength of Endorsement*
N Mean SD Clinical decision-making 807 1.09 0.428 Communication 807 1.17 0.533 Doctor-patient interactions 807 1.21 0.599 Family issues 807 1.56 0.730 Evidence-based practice 807 1.80 0.962 Cultural issues 807 2.00 0.991 Ethics 807 2.39 1.013 End-of-life care 807 2.62 0.868 Palliative care 807 2.71 0.895 * Lower scores indicate higher frequency of exposure to issue (1 = daily, 2 = weekly, 3 = monthly, 4 = almost never).
Organ System Category NAMCS Annual National Frequency NAMCS 2002 1st Diagnosis Percentage ABFM 2003 and 2004 Survey of Practice Percentage Cardiovascular 20,749,525 10.4 16.7 Endocrine 17,363,399 8.2 9.8 Gastrointestinal 12,387,729 5.1 9.5 Hematologic/immune 4,625,960 2.8 3.1 Integumentary 15,068,757 7.0 5.3 Musculoskeletal 31,860,955 13.9 12.2 Nephrologic/urologic 4,680,860 2.1 4.4 Neurologic 3,341,277 2.0 4.2 Psychogenic/behavioral 8,140,406 4.4 10.7 Reproductive, female 6,291,831 3.4 6.1 Reproductive, male 1,537,156 0.6 2.6 Respiratory 36,844,808 16.9 11.7 Special sensory 8,221,433 1.1 2.9 Nonspecific 35,958,364 16.9* 3.4* Not applicable to ABFM’s content blueprint 1,348,820 0.8 Total 208,421,280 100.0 Correspondence between NAMCS and ABFM survey of practice r = 0.78* * The nonspecific category was not included in the correlation between NAMCS and ABFM percentages.
- Table 8.
Percentage of Examination Items per Organ System, Based on 90% of the Examination Being Composed of Organ System Categories
Domain NAMCS ABFM Survey Averages NAMCS/ABFM Averages 90% of Average Cardiovascular 10.4 16.7 13.55 12.36 Endocrine 8.2 9.8 9.00 8.21 Gastrointestinal 5.1 9.5 7.30 6.66 Hematologic/immune 2.8 3.1 2.95 2.69 Integumentary 7 5.3 6.15 5.61 Musculoskeletal 13.9 12.2 13.05 11.90 Nephrologic/urologic 2.1 4.4 3.25 2.96 Neurologic 2 4.2 3.10 2.83 Nonspecific 16.9 3.4 10.15 9.26 Psychogenic/behavioral 4.4 10.7 7.55 6.88 Reproductive, female 3.4 6.1 4.75 4.33 Reproductive, male 0.6 2.6 1.60 1.46 Respiratory 16.9 11.7 14.30 13.04 Special sensory 1.1 2.9 2.00 1.82 98.70 90.00




{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Background
- The Development Process
- The New Examination Content Blueprint
- The Dimensions/Orders System
- A. Organ Systems (90% of examination questions)
- B. Population-Based Care and Health Systems (5% of examination questions)
- C. Patient-Based Care and Systems (5% of examination questions)
- Weighting
- Complexity or Depth of Knowledge
- Implementation
- Future Directions
- Conclusion
- Notes
- References
- Figures & Data
- References
- Info & Metrics
Related Articles
Cited By...
- Examining the Construct Stability of the Family Medicine Certification Scale Between One-Day Exam and Longitudinal Assessment
- The American Board of Family Medicine's 8 Years of Experience with Differential Item Functioning
- Using the Family Medicine Certification Longitudinal Assessment to Make Summative Decisions
- Validating the Test Plan Specifications for the American Board of Family Medicine's Certification Examination
- CREATING A NEW BLUEPRINT FOR ABFM EXAMINATIONS
- Frequency and Criticality of Diagnoses in Family Medicine Practices: From the National Ambulatory Medical Care Survey (NAMCS)
- Impact of One Versus Two Content-Specific Modules on American Board of Family Medicine Certification Examination Scores
- Family Physicians' Scope of Practice and American Board of Family Medicine Recertification Examination Performance
- Pass Rates on the American Board of Family Medicine Certification Exam by Residency Location and Size
- Performance on the American Board of Family Medicine Certification Examination by Country of Medical Training
- Response: Re: American Board of Family Medicine (ABFM) Launches New Exam Prep iPhone Application
- Performance on the American Board of Family Medicine (ABFM) Certification Examination: Are Superior Test-Taking Skills Alone Sufficient to Pass?