
Abstract
Type 2 diabetes is a serious, costly, and increasingly common disease. Several conditions commonly seen in family medicine settings confer increased risk of developing diabetes. Among these conditions are impaired glucose tolerance, impaired fasting glucose, obesity, gestational diabetes, hypertension, hyperlipidemia, and menopause. We here present the results of a systematic review of the literature examining the evidence for different strategies aimed at preventing type 2 diabetes in patients with these conditions. The strongest evidence supports an intensive lifestyle intervention designed to induce modest weight loss. The greatest degree of prevention, based on lesser quality evidence, may be imparted by bariatric surgery. Metformin and troglitazone have appreciable evidence in specific populations, and orlistat and acarbose have slightly less evidence among obese patients, for preventing diabetes. Ramipril, captopril, losartan, pravastatin, and estrogens show some very preliminary promise for preventing diabetes in patients treated for hypertension, hyperlipidemia, and menopause, but each needs a more rigorous evaluation. Although more questions remain to be answered, family physicians now have tools available to help our patients lead lives free of diabetes.
Diabetes mellitus is a serious, costly, and increasingly common disease.1,2 From the year 2000 to 2050, the number of persons with diagnosed diabetes is projected to increase by 165%.3 The lifetime risk for developing diabetes is estimated to be 32.8% for a man and 38.5% for a woman born in the Unites States in the year 2000.2 The vast majority of these cases will be of type 2 diabetes, a syndrome that is the result of both insulin resistance and insufficient insulin production.4 In light of the dramatic epidemic of type 2 diabetes, there is great interest in identifying and implementing interventions to prevent or delay its onset.
Impaired glucose tolerance (IGT) is a condition intermediate between normal glucose homeostasis and type 2 diabetes.5 People with IGT are identified by the results of an oral glucose tolerance test with a 2-hour plasma glucose value between 140 and 199 mg/dL. IGT places people at an increased risk of developing type 2 diabetes.6 Although not often recognized, as many as 17% of overweight Americans may have the condition.7
Like IGT, impaired fasting glucose (IFG) is a condition that falls between normal glucose tolerance and diabetes. The diagnostic criterion for IFG is a fasting glucose between 100 and 125 mg/dL.8 Both IGT and IFG are associated with an approximately equal risk of diabetes. Those with both IFG and IGT have an even higher risk.9 Although it may be tempting to consider IFG as equivalent to IGT, there is very limited information addressing diabetes prevention in patients with IFG only.10
Other factors that have been shown to increase risk of type 2 diabetes to varying degrees include obesity,11,12 a history of gestational diabetes,13,14 hypertension,15,16 and hyperlipidemia.15,16 The risk of diabetes also increases with menopause,17–19 and estrogen has known effects on glucose tolerance.20
Using the above risk factors, all of which are conditions commonly confronted in family medicine settings, as potential situations in which prevention may be applied, we present the results of research interventions designed to prevent type 2 diabetes. Although all these interventions are currently available in some form, the United States Food and Drug Administration has not yet approved the medications included in this review for the specific purpose of preventing diabetes.
Methods
Data Sources
We conducted a systematic review of the literature to identify research that addresses the prevention of type 2 diabetes. We searched MEDLINE, via PubMed, for reports in English of randomized, controlled trials in humans between January 1, 1965, and January 30, 2004, using the search terms “type 2 diabetes AND prevention,” “NIDDM AND prevention,” and “adult onset diabetes AND prevention.” This search produced a total of 282 articles. We reviewed the titles and abstracts of each study. We also added 5 studies that did not appear in the search but were suggested by subject matter experts or identified during review of the articles. From the combination of these data sources, we identified 18 articles in which preventing type 2 diabetes was the objective. These articles were reviewed in full for confirmation of the primary research outcome, description of the target population and intervention, and identification of the relative and absolute risk reduction of the intervention (Figure 1).
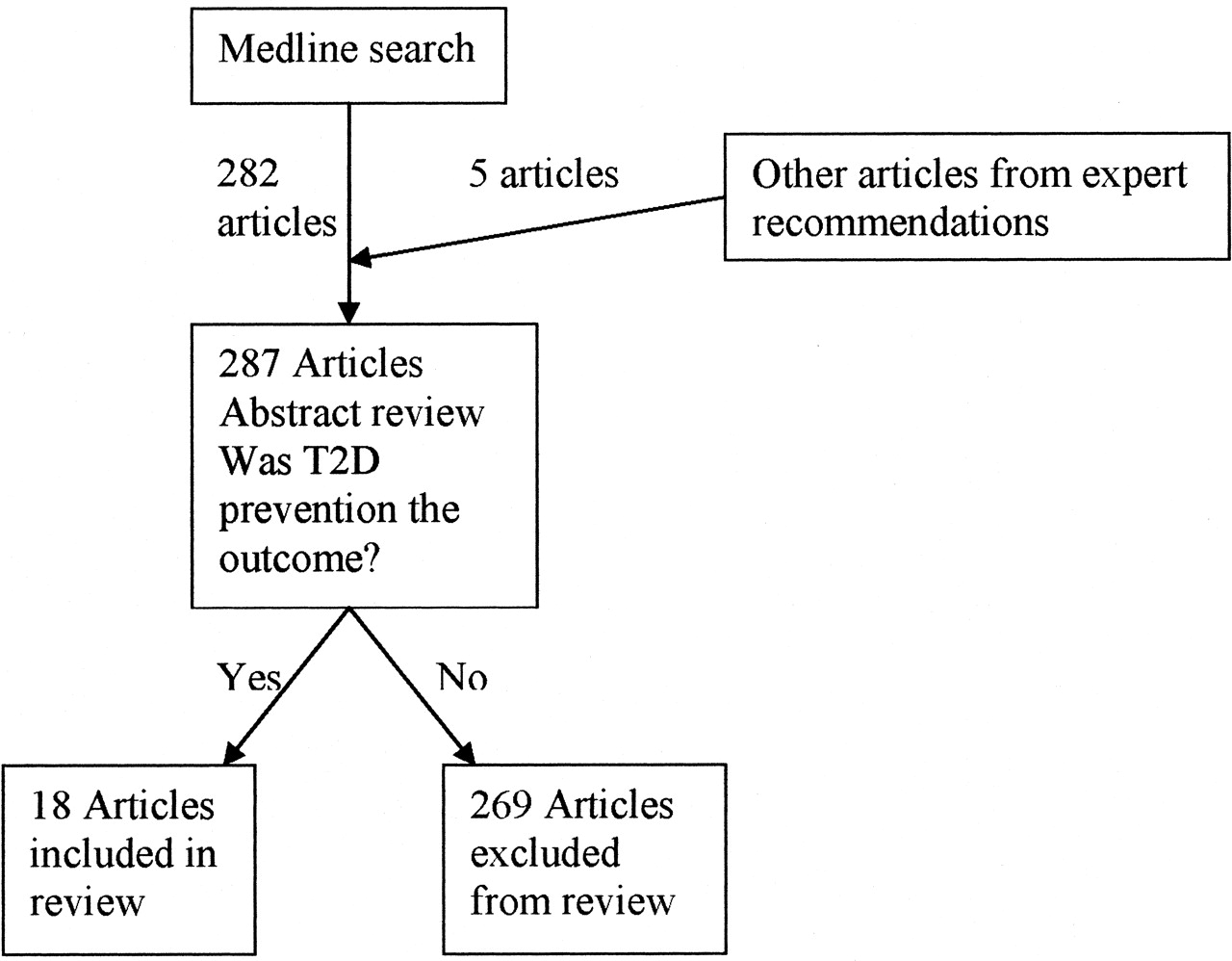
Article selection flow diagram.
Results
People with Impaired Glucose Tolerance
The Diabetes Prevention Program (DPP) studied people with IGT.21 This study’s intervention included structured education, individualized medical nutrition therapy, and intensive lifestyle modification and support designed to result in 150 minutes of physical activity per week and a 7% weight loss. Participants in the control group were given information on healthy eating patterns and exercise, but they did not receive intensive lifestyle support. The absolute risk of developing diabetes in the intervention group was 4.8% per year, compared with 11.0% per year in the control group. Using the DPP intervention, 7 people with IGT would need to be treated for 1 year to prevent 1 new case of diabetes [the number needed to treat (NNT) per year is 7]. Similar results were seen in the Finnish Diabetes Prevention Study (DPS).22 In the DPS, a comparable lifestyle adaptation intervention also resulted in 3.2% of patients in the intervention group developing diabetes, compared with 7.8% in the control group, for an NNT of 5 people with IGT over 5 years. Several other smaller studies have confirmed that similar lifestyle interventions can reduce the risk of type 2 diabetes.23–26
In another arm of the DPP, metformin (Glucophage) at a dose of 850 mg twice daily was compared with a placebo. The incidence of diabetes in the treated patients was 7.8%, compared with 11.0% in the placebo group. Twenty patients with IGT needed to be treated with metformin for 3 years to prevent 1 new case of diabetes. It is noteworthy that metformin was not more effective than placebo among those patients with a body mass index (BMI: weight in kilograms divided by square of height in meters) less than 30 kg/m2, among those over 60 years old, or in those whose fasting plasma glucose was less than 110 mg/dL. The combination of metformin and lifestyle intervention was not studied.
The Study to Prevent Non–Insulin-Dependent Diabetes Mellitus (STOP-NIDDM) examined the ability of the α-glucosidase inhibitor acarbose (Precose) to prevent type 2 diabetes in overweight and obese patients with IGT.27 In this study, patients treated with acarbose, at a dose up to 100 mg 3 times daily, experienced a diabetes incidence of 17% over 3.3 years, whereas the placebo group’s diabetes incidence was 26%. The NNT in this study was 11.5 patients treated for 3.3 years. The benefit of acarbose was seen across the range of age and obesity included in the study.
The weight loss medication orlistat (Xenical), a gastrointestinal lipase inhibitor, may also be effective in people with IGT. In a recent study of 3305 obese (BMI ≥30 kg/m2) patients with IGT, those treated with orlistat 120 mg 3 times daily experienced a 6.2% incidence of diabetes over 4 years, whereas those treated with placebo had a 9.0% incidence.28 Ten patients would need to be treated with orlistat for 4 years to prevent 1 new case of diabetes. In a meta-analysis from 3 weight loss studies that used orlistat in the same dose as above, obese (BMI ≥30 kg/m2) patients with IGT who were treated with orlistat experienced a 3.0% incidence of diabetes, compared with a 7.6% incidence in those treated with placebo.29 According to this meta-analysis, 45 obese patients with IGT would need to be treated for 2 years to prevent 1 new case of diabetes.
Other medications have been evaluated in small studies or will be evaluated soon to determine their ability to prevent diabetes in patients with IGT or similar risk.30,31
Obese People with Normal Glucose Tolerance
In the same meta-analysis cited above, among 522 obese people (BMI 30–43 kg/m2) with normal glucose tolerance, 120 mg of orlistat 3 times daily resulted in a decreased incidence of diabetes.29 Those randomized to placebo experienced a 10.8% incidence of IGT and a 1.2% incidence of diabetes over a 2-year period, whereas those who received orlistat had a 6.6% incidence of IGT and none developed diabetes. The apparent relative risk reduction for diabetes incidence over the course of this short study was 100%, but interpretation is complicated by the low incidence of diabetes in the placebo group.
In the Swedish Obese Subjects (SOS) Study, obese (BMI ≥34 kg/m2 for men or ≥38 kg/m2 for women) patients treated with gastrointestinal surgery to promote weight loss are compared with matched (but not randomized) nonsurgically treated control patients.32,33 Surgically treated patients have shown reductions of up to 97% in diabetes incidence at 2 and 5 years after surgery. The risk reduction has been greatest among those whose weight loss has been greatest. The observational nature of the study limits the ability to generalize the findings. Liposuction does not seem to affect glucose metabolism.34
Women with Previous Gestational Diabetes
The Troglitazone in Prevention of Diabetes (TRIPOD) trial studied Hispanic women with a history of gestational diabetes.35 Women with 2-hour oral glucose tolerance test values in the high end of the normal range were randomized to receive the thiazolidinedione troglitazone (Rezulin) in a dose of 400 mg daily or placebo. The treated group experienced an annual diabetes incidence of 5.4% compared with 12.1% in the placebo group. The NNT was 15 patients for 1 year. Troglitazone has since been removed from the market because of an increased risk of hepatotoxicity. Currently available thiazolidenediones do not seem to share as high a risk of hepatotoxicity but have not been studied for the purpose of preventing diabetes.36
People with Hyperlipidemia or Hypertension
Several large cardiovascular disease prevention studies have recently published post hoc analyses of the incidence of diabetes among subgroups of participants. Among people with a history of coronary artery disease, the angiotensin-converting enzyme inhibitor ramipril (Altace), up to 10 mg daily, was associated with a decrease in incidence of diabetes from 5.4% over 4.5 years in the placebo group to 3.6% in the treated group (NNT = 56 for 4.5 years).37 Use of another angiotensin-converting enzyme inhibitor, captopril (Capoten), titrated to keep supine diastolic blood pressure below 90 mm Hg, was associated with diabetes incidence of 13.3%, compared with 15.2% over 5 years in those treated with diuretics and β-adrenergic receptor blockers for hypertension (NNT = 53 over 5 years).38 Likewise, the angiotensin receptor blocker losartan (Cozaar), titrated to keep blood pressure below 140/90 mm Hg, was associated with a 1.30% incidence of diabetes per year, compared with 1.75% per year in patients treated with the β-adrenergic receptor blocker atenolol (Tenormin) for hypertension and left ventricular hypertrophy (NNT = 222 per year).39 In men with hyperlipidemia, use of pravastatin (Pravachol), at a dose of 40 mg daily, was associated with a 1.9% incidence of diabetes over 5.5 years compared with 2.8% in those patients treated with placebo (NNT = 111 for 5.5 years).40 It is not known whether other medications in these classes will have similar effects or whether these findings will withstand the scrutiny of a randomized clinical trial.
Women after Menopause
In postmenopausal women, hormone replacement therapy, using 0.625 mg of conjugated estrogens plus 2.5 mg of medroxyprogesterone acetate (Prempro) daily, was associated with a 6% incidence of diabetes over 4.1 years, versus 10% in patients treated with placebo.41 In this study, 30 postmenopausal women needed to be treated for 4.1 years to prevent 1 new case of diabetes. Any potential diabetes prevention benefits of hormone replacement therapy will need to be balanced against the other complicated risks of the therapy.
These studies are summarized in Table 1, and strength of recommendation data are provided in Table 2.
Recent Major Diabetes Prevention Studies
Evidence
Discussion
Amid all the attention given to the increasing incidence of type 2 diabetes, there is also ever-mounting evidence that the disease is preventable, even among those at highest risk. The preventive strategy with the best supporting evidence is an intensive lifestyle intervention, designed to produce modest weight loss. Although on face value the success of the DPP and the DPS may tempt physicians to recommend healthy eating and regular exercise, using the specific intervention strategies as the basis for a discussion with patients, and to believe therefore that they have provided an evidence-based preventive intervention, it is important to realize that even the control groups in these studies received more intervention than routine physician recommendations. The interventions were intensive, interdisciplinary, individualized programs aimed at inducing weight loss. Truly implementing a version of these interventions will require developing treatment teams with the ability to motivate patients to make changes in lifestyle patterns that have probably been present for decades.
The intervention that seems (based on lesser quality evidence) to have the greatest potential for preventing diabetes is bariatric surgery. However, this treatment is far more invasive than the lifestyle interventions, and the surgery requires lifestyle modifications that are probably more intensive. Because of its cost and invasiveness, bariatric surgery will probably never be the diabetes prevention strategy of choice for the majority of the at-risk population.
The medications with the strongest evidence supporting their ability to prevent diabetes are metformin and troglitazone. Of course, troglitazone is no longer available, and whether other thiazolidinediones will have similar benefits is yet to be seen. Orlistat and acarbose also show considerable promise. The other medications included in this review (ramipril, captopril, losartan, pravastatin, and estrogens) have been evaluated only in post hoc subgroup analyses. Therefore, they do not carry nearly the weight of evidence for preventing diabetes that metformin, orlistat, and acarbose do.
It is clear that there is much yet to learn about preventing type 2 diabetes. For example, does the combination of lifestyle intervention and medication have a greater effect than either alone? Does preventing diabetes by these strategies also prevent the micro- and macrovascular complications of diabetes, or does it merely prevent glucose elevation above diagnostic values? And can earlier intervention among patients with familial risk but no aberration in glucose homeostasis prevent diabetes more effectively than intervention after other risk factors have become apparent? However, there is sufficient evidence that diabetes can be prevented using techniques and agents that are currently available. The onus is now on us as physicians to implement this evidence to help our patients improve their chances of leading lives free of this disease.
- Received for publication September 6, 2004.
- Revision received September 6, 2004.
References




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.