
Abstract
Background: Although the understanding of the health impact of hormone replacement therapy (HRT) is incomplete, even less is known about the attitudes, perceptions, and motivations of women faced with the decision to use HRT. The purpose of this study was to evaluate the relation between HRT use and women’s perceptions of the risk and benefits associated with HRT use.
Methods: A written questionnaire was administered to 387 women, aged 45 years and older, responding to a health plan invitation for free bone mineral density screening. Women were asked to estimate the lifetime probability of developing breast cancer, uterine cancer, osteoporosis, and myocardial infarction when taking HRT and when not taking HRT. Women rated their quality of life in their current state of health, with breast cancer, with uterine cancer, with osteoporosis, and after myocardial infarction.
Results: HRT users perceived a greater risk reduction using HRT compared with HRT nonusers for osteoporosis (−34.9% vs −17.8%, P < .001) and myocardial infarction (−20.7% vs −8.4%, P < .001). HRT nonusers perceived a greater risk increase using HRT compared with HRT nonusers for breast cancer (16.5% vs 3.3%, P < .001) and uterine cancer (9.2% vs 0.6%, P = .004). HRT users estimated a greater quality-of-life reduction compared with HRT nonusers for osteoporosis (−31.0 vs −24.5, P = .006).
Conclusions: Regardless of whether they used HRT, women in this study overestimated their risk for all four diseases. HRT users perceived greater benefit and less risk using HRT than nonusers. The results of our study show that continuing efforts are needed to help women understand the risks and benefits of HRT.
The American College of Obstetricians and Gynecologists,1 the American Academy of Family Physicians,2 the American College of Physicians,3 and the US Preventive Services Task Force4 have previously recommended that physicians counsel postmenopausal women about their individual risks and benefits of hormone replacement therapy (HRT). Despite the widespread promotion of the benefits of HRT for preserving bone density,4 most women did not accept HRT. A nationally representative survey of US women aged from 50 to 74 years old reported in 1999 that 59% of women without a uterus and 20% of women with a uterus used HRT.5
Although the understanding of the health impact of HRT use is still incomplete, there is even less knowledge about the attitudes, perceptions, and motivations of women faced with the decision to use HRT.6 Women generally have started HRT for relief of menopausal symptoms.7 Few nonusers of HRT have been aware of the increased risk of osteoporosis associated with lack of estrogen.8 Concerns about the risk of breast cancer, uterine and endometrial cancer, menstrual bleeding, and other side effects have affected women’s decisions to accept and continue HRT.9 The purpose of this study was to evaluate the relation between HRT use and perceived risks and benefits associated with HRT use.
Methods
A written questionnaire was distributed to women aged 45 years and older responding to a health plan invitation for free bone mineral density screening. Sixty-four urban, suburban, and small-city radiology centers providing dual-energy radiograph absorptiometry (DEXA) or computerized tomographic scan measurement of bone mineral density that were participating in the health plan-sponsored screening were enlisted to assist in distribution and collection of the questionnaire. Sixty-two of the participating centers were in Oklahoma. Women completed the questionnaire without the assistance of study or radiology center staff. Women were considered to be postmenopausal if they had undergone a hysterectomy with removal of both ovaries, menses had ceased for at least 12 months, a physician had told them that they were postmenopausal, or they were 57 years old or older (age at which menopause has occurred in 99% of women).10 Women with a history of breast cancer or uterine cancer were excluded from the analysis.
Data were collected about demographic and clinical characteristics, including age, race-ethnicity, education, smoking status, exercise, height, weight, fracture history, family history of fractures, and rheumatoid arthritis. Body orientation regarding health was assessed by responses to 3 statements using a 5-point scale (almost never = 1, sometimes = 3, and almost always = 5).11 For example, one item stated, “I work hard to keep my body healthy.” Health locus of control was measured by responses to three statements from a larger instrument12 using a 6-point scale (strongly disagree = 1, moderately disagree = 2, slightly disagree = 3, slightly agree = 4, moderately agree = 5, and strongly agree = 6). Perception of overall health was measured using five levels (poor, fair, average, good, excellent). Women were asked about any menopausal symptoms they experienced (hot flashes, trouble sleeping, vaginal dryness, fatigue, skin changes, headaches, depression, and open-ended other). Attitudes toward five menopausal symptoms (hot flashes, vaginal dryness, osteoporosis, skin aging, and depression) were rated using a 5-point Likert scale (not very important = 1, neutral = 3, very important = 5).
Data were collected about daily calcium supplementation and any prescribed or nonprescription treatment of osteoporosis or menopausal symptoms. Estrogen use was classified according to current, never, and previous use. Other prescribed treatments for osteoporosis included etridonate, calcitonin, alendronate, fluoride, tamoxifen, clonidine, α-methyldopa, and raloxifene. Nonprescription medicines included vitamin D, vitamin E, valerian, dong quai, progesterone cream or oil, zinc, DHEA (dehydroepiandrosterone), sage, anise, primrose oil, licorice root, Black Bear Claws, black cohosh, soy estrogens, flaxseed, chasteberry, and Mexican wild yam root. Other medications could be added by participants.
Women were asked to estimate the lifetime probability of developing breast cancer, uterine cancer, or osteoporosis, and of having a myocardial infarction when taking HRT and when not taking HRT. They marked their estimates on a nonlinear scale from 0 to 100 (Figure 1). A nonlinear scale was used because it allowed women to make sharper distinctions of their risk in the region of smaller risk. Women rated their quality of life in their current state of health, as well as their perceived quality of life if they were to have breast cancer, uterine cancer, osteoporosis, and a myocardial infarction. They marked their estimates on a linear scale from 0 to 100. This portion of the questionnaire was pilot tested with 10 women using a think-aloud process modeled after the procedures used by the cognitive survey laboratory of the National Center for Health Statistics.13

Example of risk and utility estimate scales.
For each participant, menopausal symptoms were summed to calculate a menopause symptom composite score. Likert scale responses regarding attitudes toward preventing menopausal symptoms were summed to create a composite score to measure global attitude toward menopause symptom prevention. Perceived risk difference for each condition was calculated by subtracting the perceived risk of the condition when taking HRT from the perceived risk when not taking HRT. Quality-of-life difference for each condition was calculated by subtracting the quality-of-life estimate in the current health state from the quality-of-life estimate with each of the four diseases.
Statistical analyses included descriptive analysis (t test for difference of means and chi-square for proportions), univariate relative odds, and multivariate logistic regression. Means of risks, quality-of-life estimates, risk differences, and quality-of-life differences were calculated, together with 95% confidence intervals, using normal approximation.14 Risk differences and quality-of-life differences were classified into high and low groups for univariate comparisons between users and nonusers of HRT, using the means as cutoffs. Because the distribution differed significantly from normal, the median was used as the cutoff for the risk difference of breast cancer. A multivariate logistic regression model was created to consider simultaneously the relation between HRT use and perceived risk differences, quality-of-life differences, age, race (white vs nonwhite), fracture history, symptoms of menopause, any other osteoporosis treatment, nonprescription drug use for menopausal symptoms, and cigarette use. A stepwise backward elimination technique (likelihood ratio test, P < .1) was used to determine the best model. Analysis of residuals did not suggest major analytic limitations that were due to violations of model assumptions. Data were analyzed using the personal computer version of Statistical Package for the Social Sciences (SPSS/PC+ version 7.5).
Results
Questionnaires were completed by 387 of 663 women (58.4%) who attended one of the participating bone mineral density screening sites. Of the women who completed a questionnaire, 330 were found to be postmenopausal and without a history of breast or uterine cancer. Of the postmenopausal women, 220 (66.7%) were current HRT users, 106 (32.1%) did not take HRT, and 4 had missing data.
The characteristics of participants according to HRT use are displayed in Table 1. Most respondents were highly educated, with 59% having a college education or higher. Most women (94.1%) were white. HRT users were younger (59.2 years vs 63.2 years, P < .001). A higher proportion of HRT users were ever-smokers (29.3% vs 17.9%, P = .028), although there was no significant difference in pack years between the smokers in the two groups. More HRT nonusers reported a history of fracture (13.5% vs 6.2%, P = .03). Most fractures in HRT nonusers were wrist fractures. More HRT users had ever had symptoms of menopause (82.9% vs 64.8%, P = .001). More HRT nonusers used another prescribed treatment for osteoporosis prevention (19.4% vs 10.8%, P = .08), but fewer HRT nonusers reported using at least one nonprescription medication (15.7% vs 23.0%, P = .18).
Characteristics of Postmenopausal Women Participating in Osteoporosis Screening, by Use of Hormone Replacement Therapy.
Attitudes about preventing menopausal symptoms, general health, body orientation, and locus of control appeared similar for HRT users and nonusers. Both groups of women took responsibility for their health, with 93% agreeing with the statement, “The main thing which most affects my health is what I myself do.” Only 18.3% agreed with the statement, “Luck plays a big part in determining whether I will get sick.”
Women’s perceptions of risk for developing breast cancer, uterine cancer, osteoporosis, or myocardial infarction with or without HRT are displayed in Figure 2. Both HRT users and HRT nonusers estimated lifetime probabilities that were inflated for all four diseases both on and off HRT. The perceptions of the risk of developing breast cancer, osteoporosis, and myocardial infarction when not taking HRT were similar in both groups. HRT nonusers estimated higher risks for all four diseases while using HRT. HRT users perceived a greater risk reduction using HRT for osteoporosis compared with HRT nonusers (−34.9% vs −17.8%, P < .001) and myocardial infarction (−20.7% vs −8.4%, P < .001). HRT nonusers perceived a greater risk increase using HRT compared with HRT users for breast cancer (16.5% vs 3.3%, P < .001) and uterine cancer (9.2% vs 0.6%, P = .004).

Risk perception and hormone replacement therapy (HRT).
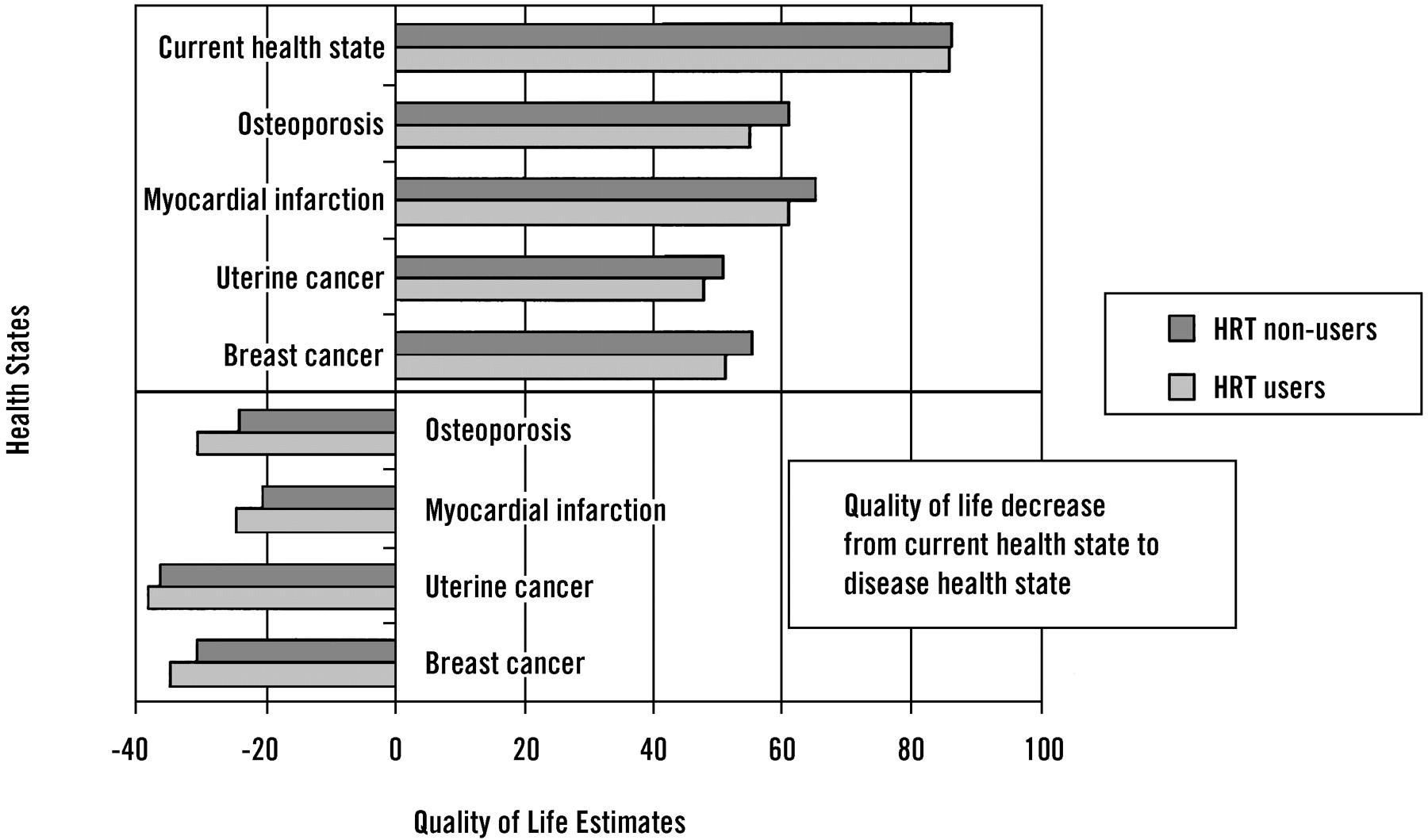
Perceived quality-of-life estimates in the current state of health and all four diseases were similar for HRT users and nonusers (Figure 3). HRT users estimated a greater quality-of-life reduction for osteoporosis compared with HRT nonusers (−31.0 vs −24.5, P = .006). The quality-of-life reductions for other diseases were not significantly different.
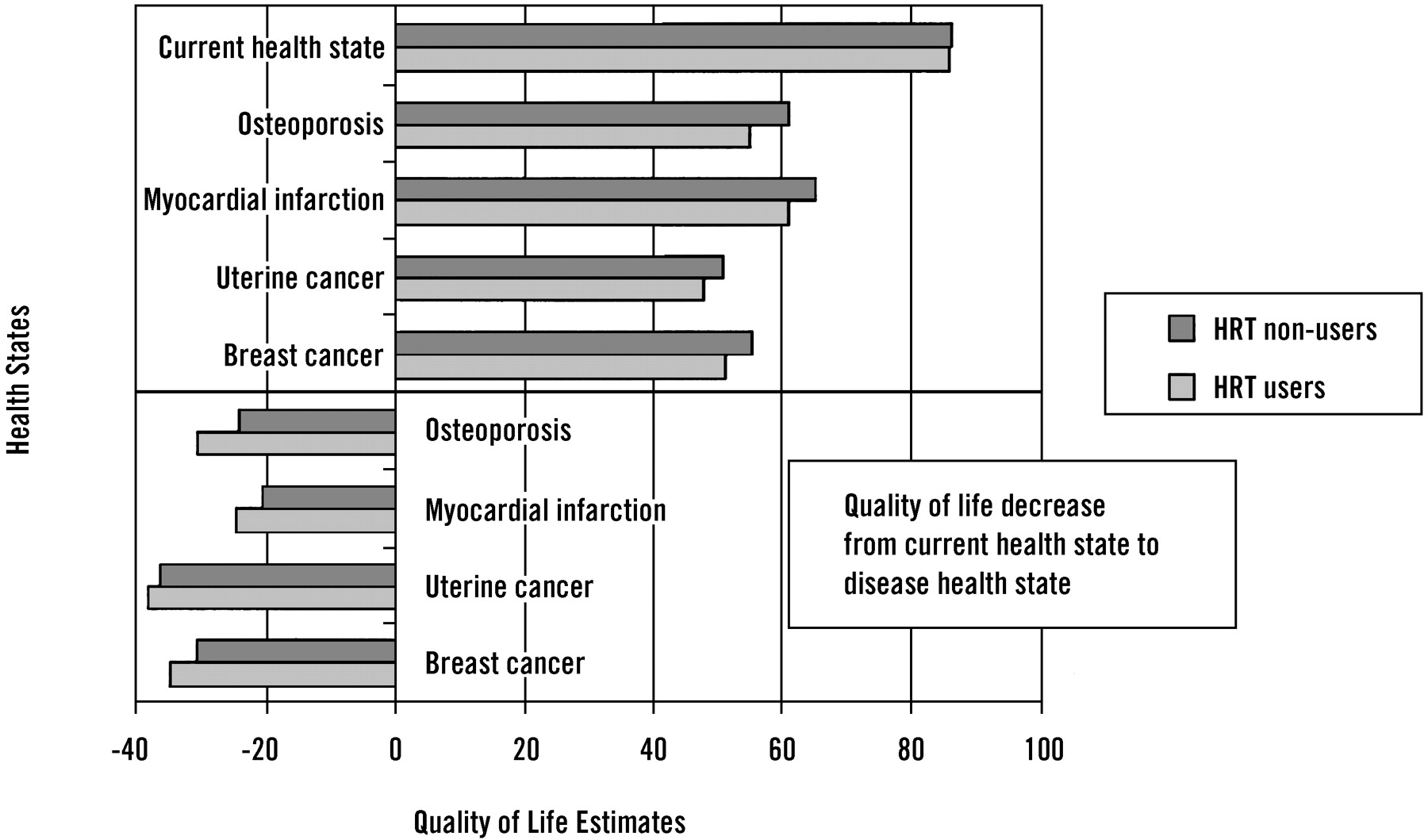
Quality of life of health states considered with hormone replacement therapy (HRT).
The univariate relative odds of HRT use and the relative odds of HRT use, adjusted by logistic regression (ROadj) according to perceived risk differences, estimated quality-of-life differences, and other selected characteristics, are displayed in Table 2. The most parsimonious descriptive model included only menopausal symptoms, breast cancer risk difference, myocardial infarction risk difference, osteoporosis risk difference, and the quality-of-life difference with breast cancer. Instead, we present a model that includes other variables that are well known to be associated with osteoporosis and HRT use, because small numbers might have affected the significance of their relationship. Inclusion of these variables did not greatly affect the relative odds estimates for the other variables. Overall, HRT users perceived less risk associated with HRT use. As expected, a greater estimate of the reduction in quality of life with osteoporosis increased the likelihood of HRT use (ROadj 2.39, 95% confidence interval [CI] 0.96, 5.96). Women using HRT, however, also had a greater estimate of the reduction in quality of life with breast cancer (ROadj 3.63, 95% CI 1.23, 10.74). There were no significant interactions found between risk perceptions and quality-of-life estimates for the same disease.
Relation Between Hormone Replacement Therapy Use and Perceived Risk, Quality of Life, and Selected Clinical Characteristics.
Discussion
Regardless of whether they used HRT, women in this study overestimated the risk for all four of the diseases, particularly uterine and breast cancer. Compared with nonusers, however, HRT users believed that HRT would produce a greater reduction in the risks of osteoporosis and myocardial infarction and a smaller increase in the risks of breast and uterine cancer. In addition, the decrease in perceived quality of life with osteoporosis was slightly greater for HRT users.
These findings expand the less quantitative results of previous studies. In a similar group of highly educated women with a median age of 50 years, 52% of women perceived their risk of developing breast cancer by age 70 years to be ≥10%.15 In contrast, 73% of the women estimated their risk of heart disease by age 70 to be ≤1%. In a National Council on Aging survey of women between 45 and 64 years old, 61% were most afraid of cancer (particularly breast cancer), and only 9% were most afraid of heart disease.16 Women in England have similar health concerns. Cancer was the highest health priority of 40.7% of women, and heart disease was the highest priority for only 6.6%.17 The magnitude of misperception of personal risk, as shown by our study, suggests that it might be useful to include realistic disease-specific population risks as anchors to facilitate risk communication.
The results of this study are consistent with expectations based on the Health Belief Model, which explains behavior to prevent a health condition according to perceived susceptibility, seriousness, benefits, and barriers.18 Bandura19 added the concept of self-efficacy, defined as the conviction that one is capable of behaviors required to produce the desired outcome. In our study of mostly self-efficacious women, as measured by responses to questions regarding internal health locus of control, HRT users considered themselves more susceptible to conditions that were perceived to reduce their quality of life markedly. HRT users perceived greater benefits and lesser risk using HRT.
Because of the design of the study, however, it is impossible to determine whether these perceptions preceded the choice to use HRT. Women might have first chosen HRT and subsequently developed risk perceptions that supported this decision. This type of cognitive restructuring by persons making decisions under value conflicts has been previously described by Svenson et al.20 The optimistic estimates of HRT users and the pessimistic estimates of HRT nonusers regarding the impact of HRT are consistent with this interpretation as well. For instance, HRT users might have increased their perception of risk of osteoporosis after their decision to use HRT and might have reduced or failed to increase their estimate of the risk of breast cancer. Only a prospective study design could elucidate these decision-making processes.
Menopausal symptoms were also associated with HRT use, consistent with findings of other studies.21–23 Oddens and Boulet21 reported high rates of menopausal symptom experience among women taking HRT. Larcos22 and Rozenberg et al23 found that physicians are more likely to prescribe HRT when patients complain of menopausal symptoms.
The greater proportion of ever-smokers in the group taking HRT suggests that these women could be taking HRT to compensate for a perceived increased risk of osteoporosis or heart attack caused by smoking. In a similar manner, higher rates of exercise among women not taking HRT could explain why these women perceived a reduced risk of osteoporosis and myocardial infarction in the absence of HRT use. Both observations are consistent with risk homeostasis theory.24
Our study might be limited by a lack of generalizability to all postmenopausal women. All the women in this study had already responded to an invitation for bone mineral density screening. Many were college educated, and most were already HRT users. Consequently, their perceptions of risk and quality of life might not reflect the perceptions of all postmenopausal women. The instrument used to elicit perceived risk and utility with only written instructions could have increased the error of measurement. The use of a nonlinear scale from 0 to 100 to estimate perceived risk of diseases while using a linear scale from 0 to 100 to estimate quality of life might have been confusing to some women and could have led to biased estimates of perceived risk and quality of life. A few women did estimate a better quality of life with one of the four diseases compared with their current state of health; however, this response seldom occurred. Although our sample size was comparable to other studies with similar goals, a larger sample would have allowed greater precision in our estimates of association. We did not ask about other conditions that possibly could affect the decision to use HRT, such as thromboembolism, dementia, and depression.
This study, among others, shows that postmenopausal women often have an inflated perceived risk of developing adverse outcomes while taking HRT.25,26 Women who choose not to take HRT perceive even higher risks associated with HRT use. Because the women in this study were highly educated and highly motivated to improve their health, we suggest that women in the general population might have perceptions of risk that are even more unrealistic. Our study suggests that perception of risk of diseases and quality of life does play an important role in decision making for postmenopausal women choosing whether to use HRT. If women are to make decisions based on risk and quality of life, they must be given accurate information by clinicians. Direct observation of physician-patient communication has previously shown that discussions of risks and benefits are infrequent.27 The results of our study show that continuing efforts are needed to help women understand the risks and benefits of HRT.
The recent highly publicized studies that failed to show HRT (estrogen-progestin) efficacy for both primary and secondary prevention of ischemic heart disease28–30 and studies that suggest an increased risk for breast cancer associated with HRT use30–32 might further influence the perceptions of postmenopausal women. In particular, the early termination and publication of the main results of the estrogen plus progestin arm of the Women’s Health Initiative (WHI) showed that the disease prevention benefits of combination HRT were outweighed by the harms.30 Already on the heels of this revelation are indications that the constantly evolving decision of whether to use HRT has not become moot. The observational component of the WHI has reported results suggesting that only HRT users with elevated C-reactive proteins might be at increased risk for cardiovascular events.33 Seeking a better understanding of how to communicate benefits and harms is an important step toward helping women deal with this paragon of increasingly complex health care decisions.
Acknowledgments
We are indebted to the Wellness Division of the State and Education Employees Group Insurance Board for their assistance in conducting the survey.
Notes
Presented in part at the Society for Medical Decision Making, Cincinnati, Ohio, September 26, 2000.
- Received for publication October 11, 2002.
- Revision received October 11, 2002.
References




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.