
Abstract
Background: Follow-up after a positive colorectal cancer screening test is necessary for screening to be effective. We hypothesized that nurse navigation would increase the completion of colonoscopy after a positive screening test.
Methods: This study was conducted between 2008 and 2012 at 21 primary care medical centers in western Washington State. Participants in the Systems of Support to Increase Colorectal Cancer Screening study who had a positive fecal occult blood test (FOBT) or flexible sigmoidoscopy needing follow-up were randomized to usual care (UC) or a nurse navigator (navigation). UC included an electronic health record–based positive FOBT registry and physician reminder system. Navigation included UC plus care coordination and patient self-management support from a registered nurse who tracked and assisted patients until they completed or refused colonoscopy. The primary outcome was completion of colonoscopy within 6 months. After 6 months, both groups received navigation.
Results: We randomized 147 participants with a positive FOBT or sigmoidoscopy. Completion of colonoscopy was higher in the intervention group at 6 months, but differences were not statistically significant (91.0% in navigation group vs 80.8% in UC group; adjusted difference, 10.1%; P = .10). Reasons for no or late colonoscopies included refusal, failure to schedule or missed appointments, concerns about risks or costs, and competing health concerns.
Conclusions: Navigation did not lead to a statistically significant incremental benefit at 6 months.
Impact: Follow-up rates after a positive colorectal cancer (CRC) screening test are high in a health care system where UC included a registry and physician reminders. Because of high follow-up rates in a health care system where UC included a registry and physician reminders, and small sample size, we cannot rule out incremental benefits of nurse navigation.
There is strong evidence that colorectal cancer (CRC) screening decreases CRC incidence and mortality.1 Despite the efficacy of screening, almost 40% of eligible adults are not screened at recommended intervals,2 and many have never had any type of CRC screening. Screening failures occur not only from a lack of screening but also from breakdowns in follow-up on positive tests, which obviate the benefits of screening.
Complete diagnostic evaluation with optical colonoscopy is recommended after a positive fecal occult blood test (FOBT) or a positive flexible sigmoidoscopy, that is, when precancerous lesions are found or polyp resection is incomplete. In randomized controlled trials, rates of completed diagnostic evaluation have ranged between 83% and 90%.3⇓–5 However, in community-based studies, completion of recommended follow-up is much lower, with rates of 30% to 65% reported.6⇓⇓–9 Lack of diagnostic follow-up after a CRC screening test has been associated with increased risk of death due to CRC10,11 and is a potential medicolegal issue.12,13
To test a method of improving follow-up, patients who had a positive FOBT or sigmoidoscopy were randomized to receive either usual care (UC) (which included a positive FOBT registry and provider reminder system) or UC plus nurse navigation to support care coordination (colonoscopy scheduling) and patient self-care (preparing for and completing testing). We hypothesized that nurse navigation would lead to increased rates and more rapid completion of diagnostic testing after a positive screening test.
Methods
This study was a follow-up trial within the larger Systems of Support to Increase Colorectal Cancer Screening Study (SOS) conducted from August 2008 through June 2012. The methods and design14 and screening outcomes15 of the main study, which tested incremental levels of support to increase CRC screening rates, have been published. The study was conducted at 21 primary care clinics of the Group Health Cooperative, a large, nonprofit, integrated health care delivery system in Washington State.
Participants 50 to 74 years old were eligible for the follow-up trial if they had a positive FOBT (SENSA; Beckman Coulter, Brea, CA), with ≥1 of 3 cards guaiac-positive for blood, or a flexible sigmoidoscopy with an adenomatous lesion or incomplete polyp resection while they were participating in the main SOS trial. Patients were not eligible for the follow-up study if they had a diagnosis of CRC before the positive test; had a colonoscopy after enrollment in the parent study but before the positive FOBT or flexible sigmoidoscopy; died; or left the health plan before the positive screening test. The Group Health Institutional Review Board approved all study procedures. Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health (award no. R01CA121125; clinicaltrials.gov identifier NCT00697047).
Randomization
An electronic database captured positive screening tests and automatically randomized participants in equal proportions to UC or nurse navigation (navigation). Concealed random allocation sequences with a block size of 4, stratified by clinic and by whether the participant had a positive FOBT or a positive sigmoidoscopy, were generated by a computer program.
Blinding
Investigators were blinded to outcomes until all data were collected. Because of the nature of the intervention, the navigator and patient could not be blinded to interventions.
UC and Interventions
UC at Group Health included a positive FOBT registry.16 Primary care providers (mainly physicians) were sent electronic health record (EHR) reminders about their patients with a positive FOBT who had not completed a colonoscopy until either the patient completed testing or until the provider filled out an exception form stating why colonoscopy was not indicated (eg, patient refused, was too ill, or left the health plan and had been notified to follow up with their new provider). Medical center directors received lists of providers who had patients without diagnostic follow-up or exception forms. Follow-up after a positive sigmoidoscopy was the responsibility of the performing provider and/or the patient's physician and was not part of the FOBT registry.
Patients randomized to the intervention arm received UC plus navigation interventions that targeted the 6 domains of Wagner's chronic care model, including evidence-based decision and self-management support, clinical information systems, delivery system design, health care organization, and community resources.17 Some of these components were already part of UC at Group Health. In addition, the navigation intervention emphasized delivery system design (care coordination, linking patients to community resources) and self-management support (addressing patients' barriers).
Study nurse navigators were registered nurses already practicing within Group Health who had additional paid time to provide study interventions. They used the study database to identify new patients randomized to the navigation arm and track ongoing interventions (referral, scheduling appointments, precolonoscopy preparation needs) until the patient completed a diagnostic colonoscopy or the provider adequately documented in the EHR the reason that colonoscopy was not done. Upon receiving notification of a new participant, the nurse reviewed the patient's EHR to determine what follow-up already occurred. If processes of care were not underway or were incomplete, the nurse contacted the patient and their physician as appropriate. The nurse assisted the patient in completing colonoscopy, including resolving barriers such as understanding insurance coverage, making an appointment, planning for preparation and transportation, and addressing concerns or ambivalence about testing. The nurses used motivational interviewing techniques, and their phone conversations with participants were periodically monitored or directly observed by study personnel. After diagnostic testing was completed, the nurse also confirmed that documentation was complete, including ensuring that a copy of the colonoscopy procedure report and pathology (if a biopsy was performed) were entered into the EHR.
Measures
The primary outcome was completion of colonoscopy within 6 months (defined as 184 days) of the positive screening test. Colonoscopy is the preferred diagnostic test after a positive FOBT or sigmoidoscopy at Group Health. No study participants received alternative testing such as computerized colonography or sigmoidoscopy combined with barium enema. EHR procedure and claims data were used to determine whether a colonoscopy was completed and the date of the examination (nurse or patient self-report of colonoscopy were excluded because of the possibility of ascertainment bias). Secondary outcomes included time to completion and reasons for lack of or late colonoscopy. Late colonoscopy was defined as one occurring after 6 months. Chart audit and nurse navigator entries into the study database were used to assess reasons for noncompletion.
Analysis
Power estimates were based on the assumptions that 7000 patients would be randomized in the main SOS study, 45% would complete a FOBT with a 6% positive rate, and 8.5% would complete a flexible sigmoidoscopy with a 12% positive rate.14 These assumptions resulted in an estimated 260 participants who were eligible for the follow-up study, providing 80% power to detect a 15% difference between groups, assuming the colonoscopy completion rate within 6 months was 65% among the UC group. Analyses were completed using Stata statistical software, version 12.0 (StataCorp, College Station, TX).
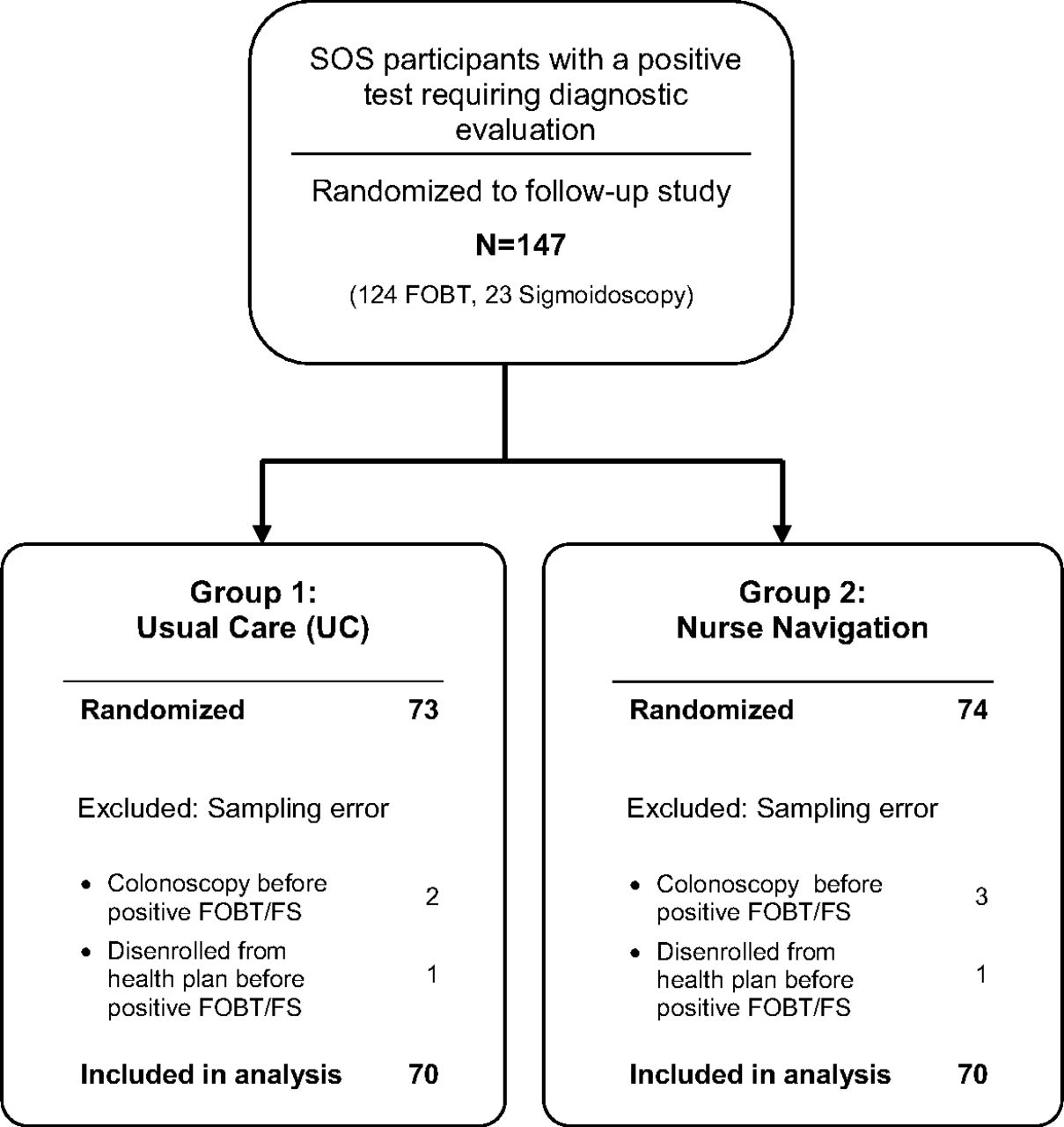
The analysis was based on intent-to-treat principles. Participants were included in the analysis according to the randomization group to which they were assigned regardless of intervention received. However, randomized participants were excluded from the analysis if they had been sampled in error, that is, they had received a colonoscopy or disenrolled from the health plan after randomization into the main SOS study but before the positive FOBT or positive sigmoidoscopy that flagged them for the follow-up study (Figure 1). Logistic regression models were used to estimate predictive margins for the binary primary outcome of completing colonoscopy within 6 months of the positive screening test. Predictive margins are estimated probabilities adjusted across the covariate distribution in the sample. Differences between groups are reported as relative risks and risk differences with 95% confidence intervals.

Consort diagram of the System of Support Trial study participants with a positive fecal occult blood test (FOBT) or flexible sigmoidoscopy (FS); SOS, Systems of Support to Increase Colorectal Cancer Screening Study.
Results
Of the 4664 participants in the main SOS trial, 124 participants had a positive FOBT and 23 had a sigmoidoscopy needing follow-up, totaling 147 randomized patients. Participants sampled in error were excluded from the analysis, including 5 participants who received a colonoscopy before the positive FOBT and 2 who left the health plan before completing the FOBT, leaving 140 participants who were analyzed (Figure 1). Table 1 shows baseline characteristics of the patients in the UC and navigation arms. The majority was <65 years old and white. Patients in the UC group were somewhat more likely to have less formal education and slightly more likely to be married.
Overall, 85.7% (120 of 140) had a colonoscopy within 6 months of the positive screening test. Rate of colonoscopy completion within 6 months was higher in the navigation arm than the UC group, but differences were not statistically significant (adjusted proportions: navigation, 91.0% vs UC, 80.8%; adjusted net difference, 10.1%; P = .10) (Table 2). Six-month colonoscopy completion rates were not influenced by the type of positive screening test (positive FOBT, 79.7% vs 90.0% and positive sigmoidoscopy, 81.8% vs 90.9% in the UC vs navigation arms, respectively). The time between positive screening test and colonoscopy among participants who completed colonoscopy was similar across intervention groups, with a mean of 53.6 days (standard deviation, 35.6 days) in the UC arm and 56.5 days (standard deviation, 38.0 days) in the navigation arm.
Of the 20 participants without colonoscopy at 6 months (14 in the UC and 6 in the navigation group), 9 had a colonoscopy within 12 months (5 in the UC and 4 in the navigation group). One additional participant receiving UC completed colonoscopy at 13 months, and 10 had no follow-up testing. The overall percentage completing colonoscopy within 13 months was 92.9% (130 of 140).
Charts were audited to assess reasons for lack of and late diagnostic follow-up (Table 3). As previously noted, both arms received navigation interventions if a colonoscopy was not completed by 6 months. All patients receiving UC and navigation received colonoscopy referrals from their primary care physicians. In 3 instances, UC patients with either a positive FOBT (n = 2) or sigmoidoscopy (n = 1) were referred but had not made an appointment until the nurse navigator assisted them with scheduling. Other reasons for late colonoscopy in both the UC and navigation groups included canceled and missed appointments, concerns about colonoscopy risk, being too busy, competing health issues, or losing or changing health insurance. Reasons for no colonoscopy in both groups included active refusal, passive refusal by missing appointments, losing health insurance, and serious health issues.
Discussion
Although navigation led to a 10% net increase in receipt of a colonoscopy within 6 months compared with UC, group differences were not statistically significant. A limitation of our study was that the power calculations were based on a planned sample size of 260, but only 147 participants were randomized. Budget cuts required decreasing the sample size of the main SOS trial from 7000 to 5000 participants, with the result of fewer participants being eligible for the follow-up study.14 In addition, the number of positive screening tests in the main trial was smaller than projected.
Another explanation for the lack of differences between the groups is a ceiling effect. Follow-up rates were high in the UC group, probably because of the registry, with physicians receiving ongoing reminders until either colonoscopy was completed or the reason for noncompletion was documented in the EHR. In 2008 Miglioretti et al16 reported that diagnostic evaluation follow-up rates within 1 year of a positive FOBT at Group Health were 60% between 1993 and 1996 but increased to 82% by 2006 (3 years after implementation of the positive FOBT registry). The SOS study was already underway when we received this information, and we chose to continue study interventions because of the possibility that we might still find significant differences between groups.
Other studies that included navigation interventions have had mixed results. Using a community health worker navigator program in a safety-net clinic health care system, Raich et al18 found improvements in rates of diagnostic resolution (79% vs 58%; P < .002) and time to resolution. In contrast, Wells et al19 failed to find significant differences in resolution rates after a positive FOBT using a community health worker navigation intervention tailored for minority groups. Paskett et al20 tested whether nurse navigation improved time to resolution after abnormal cervical, breast, or colorectal screening tests or symptoms. Navigation decreased time to diagnostic resolution compared with UC; greater differences between groups appeared over time, suggesting that prolonged interventions with persistent reminders might lead to eventual completion of colonoscopy. In our study, the UC group received navigation after 6 months, and the overall proportion with colonoscopy follow-up continued to increase for both groups, particularly for navigation (only 2 patients did not have colonoscopy), supporting the view that some patients may benefit from prolonged interventions. Follow-up interventions that included systems changes have been more consistently positive. In a cluster trial performed by Humphrey et al21 at Veteran's Administration clinics, positive fecal tests directly sent to the gastroenterology clinic and use of a standard workflow for creating patient appointments led to a 31% increase in diagnostic evaluation at 180 days. Follow-up rates were low, however: Only 50% of the intervention patients completed colonoscopy.
Notable in our study was that all patients received a gastroenterology referral. Instances of system breakdowns still occurred, however; patients did not receive calls or make an appointment until reminded by the nurse navigator. Myers et al22 showed that one-on-one physician training and audit and feedback (physicians receiving lists of their patients without complete diagnostic evaluations) resulted in improved completion of diagnostic testing (from a baseline rate of 50% to 63% compared with controls, who remained unchanged at 53%; P < .03). Singh et al23 assessed a clinic-based quality improvement activity that included provider education, a positive FOBT registry, and feedback resulted in a significant decrease in time to colonoscopy referral and completion. Colonoscopy completion increased from 64% to 76%. In our study the combination of a systems approach (the positive FOBT registry) and either initial or delayed navigation resulted in colonoscopy follow-up rates exceeding 92%. We know of no clinic-based interventions reporting completion rates this high.
Study limitations included the requirement of verbal consent to participate in the main study and the fact that volunteers might be more compliant with both screening and completing diagnostic evaluations and thus not be representative of Group Health patients or the general population. In addition, almost all participants had health insurance, and most policies covered diagnostic colonoscopy; thus these results may not generalize to patients without health insurance or with high-deductible plans. Our interventions may also be less generalizable to community primary care practices that do not directly capture colonoscopy data from external providers and hospitals. However, most primary care practices have EHRs and are increasingly using these or registries for quality improvement and reporting efforts. Navigators could be used to assist community practices in capturing colonoscopy data and outcomes and to update EHRs and registries for the purposes of tracking population-based CRC screening completion, follow-up testing, and ongoing surveillance.
Our study also had several notable strengths. The study reported extremely high positive FOBT or sigmoidoscopy follow-up rates—higher than those previously reported in clinic settings. UC alone, which included a registry and physician reminders, led to very high completion rates, and even though our findings were not significant, a 10% improvement could be important because 2% to 4% of patients with a positive FOBT will have CRC and up to one-third will have advanced adenomas at colonoscopy.24 Larger studies are needed to confirm the independent benefits of registries, potential incremental benefits of navigation, and whether navigation increases diagnostic evaluations beyond 6 months. In addition, navigation may have differential benefits in settings without robust systems for follow-up or for populations with health disparities. Future studies of different populations should investigate these potential differences.
Acknowledgments
The authors thank Systems of Support Trial study nurses, Sandy Randles and Diana Griffith.
Notes
This article was externally peer reviewed.
Funding: Work on this article was supported by the National Cancer Institute Award R01CA121125 (ClinicalTrials.gov: NCT00697047).
Conflict of interest: BBG is an editorial board member of the JABFM.
- Received for publication April 21, 2014.
- Revision received August 1, 2014.
- Accepted for publication August 5, 2014.




{kind=link}