Abstract
Almost all working adults, more than half in any given year, experience low back pain. Although the differential diagnosis is extensive, most symptoms have biomechanical causes and resolve promptly with little intervention, although recurrence is common. History and physical examination are important in distinguishing potential causes and identifying “red flags” for more serious conditions. Diagnostic imaging should be ordered only when necessary because of the high incidence of radiologic abnormalities in asymptomatic persons. Once serious illness is ruled unlikely, first-line drug therapy with acetaminophen, a cyclo-oxygenase-2 inhibitor or a nonsteroidal anti-inflammatory drug is recommended. Short-term use of muscle relaxants may be considered, but they can be sedating. Patients should stay as active as possible. Comorbid conditions such as sleep disorders, anxiety, or depression should be treated, and psychosocial issues should be addressed. Opioids should be prescribed if other treatments have been insufficiently effective and if there is evidence of improved function with opioid treatment that outweighs adverse effects. Adjuvant antidepressants and anticonvulsants should be considered, especially in chronic or neuropathic pain. If a structural defect is identified and a diagnostic or therapeutic procedure is available, consider referral. If symptoms have not improved within 4 to 6 weeks, re-evaluation and additional diagnostic workup should be considered.
Low back pain is nearly ubiquitous in American society. It is frequently treated by family physicians and is the fifth most common reason for all physician visits.1 It is also a leading cause of lost work time and disability, responsible for direct health care expenditures of more than $20 billion annually.2
Many published guidelines for the diagnosis and management of low back pain are available. Most are straightforward, but few emphasize what family physicians actually do in practice, and they lack the richness that comes from also addressing the psychosocial issues,3 such as economic factors, averse incentives, cultural expectations, and personal reactions, that usually surround this problem.
Definitions
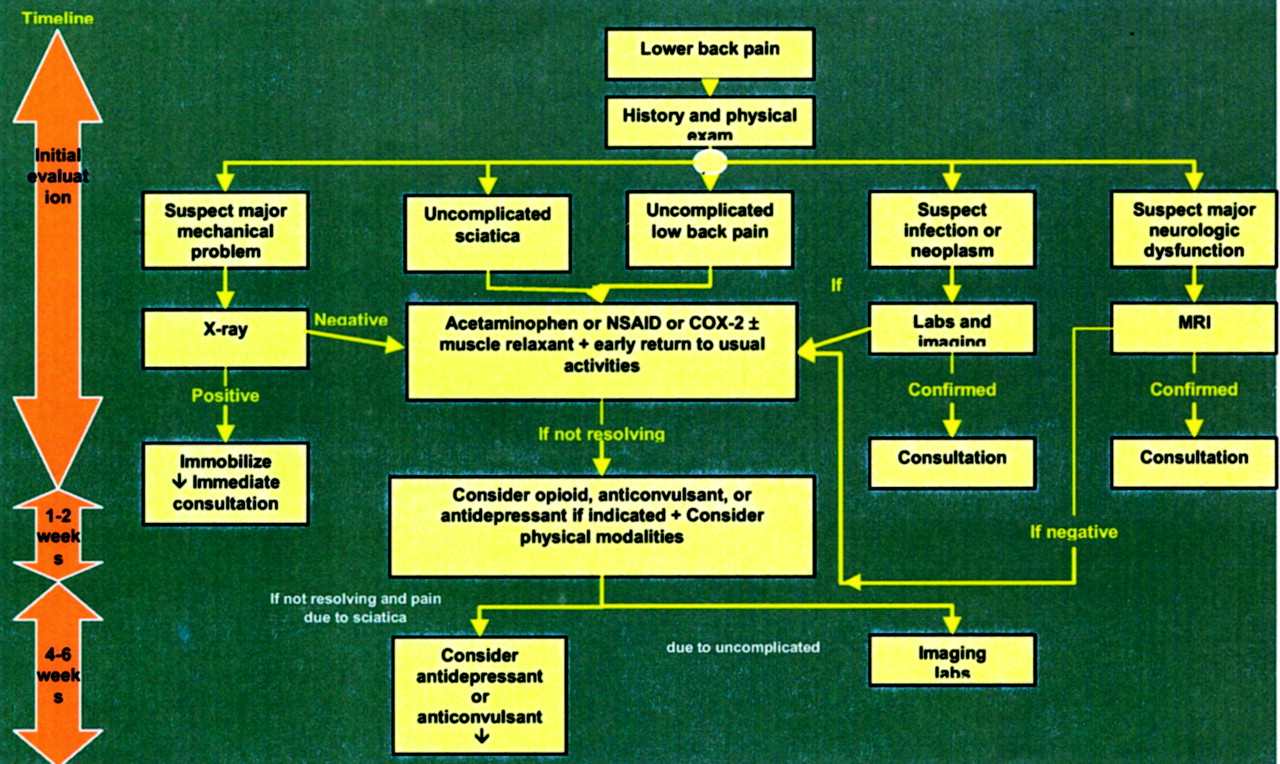
Low back pain can be broadly categorized into 5 clusters, including: (1) uncomplicated low back pain (nonradiating with no structural damage or defect), (2) uncomplicated sciatica (radiating back pain that does not extend below the knee), (3) major neurologic dysfunction (loss of motor function or continence), (4) major mechanical problem (spinal fracture or instability), and (5) infection or neoplasm. These categories drive the initial portions of the management algorithm (Figure 1). Many authors also divide low back pain into acute and chronic.4

Algorithm for evaluation and management of low back pain.
Although not always immediately apparent or easily determined, it is believed that most patients with low back pain have an underlying anatomic pain generator driving the symptoms.5 Potential pain generators include myofascial tissues, facet (zygapophysial) joints, discs, nerves, ligaments, and bony structures.
Prevalence and Natural History
Back pain is the most frequent cause of activity limitation in people aged younger than 45 years. Approximately 90% of all people experience low back pain at some time,6 and up to 50% of working adults have back pain each year.7
Most patients who miss work because of back pain return within 3 months. On average, 60% to 70% recover by 6 weeks and 80% to 90% by 12 weeks. After 12 weeks, further recovery is slow. Lifetime recurrence rates of as high as 85% have been documented.8 Reported rates of low back pain are generally higher for white persons than for other racial groups.8 Biopsychosocial factors such as presence of depression symptoms, previous history of back trouble,9 reimbursement issues, and ongoing litigation affect recovery and prognosis. When a public insurance system eliminated compensation for pain and suffering, the incidence of claims decreased by 31%. Improvements in pain and physical functioning and the absence of depressive symptoms correlated with faster claim closure. High pain intensity, female gender, full-time employment, concentration problems, and lawyer involvement early in the claim process delayed claim closure.10
Each year, about 2% of the American workforce have back injuries covered by workman’s compensation. The total annual direct cost of treating this subgroup was estimated to be $11.4 billion in 1994.6,11 Low back pain accounted for 23% ($8.8 billion) of total workers’ compensation payments in 1995.12
Differential Diagnosis
Low back pain has many causes. An exact diagnosis and anatomic pain generator may not always be evident, especially at the first visit. It is important to consider all possible causes (Table 1). It has been postulated that a pain-spasm cycle may exist in low back pain.13 Whether this is a protective muscle spasm indicating pathology in a neighboring joint has yet to be elucidated.14 Myofascial trigger points commonly occur, and bony and ischemic pain may contribute to symptoms. Bulging intervertebral discs and osteophytes may impinge on a nerve root, causing pain and dysesthesia. Pain can also be referred from more distant sources, including visceral organs, including abdominal aortic aneurysm or renal stones.
Differential Diagnosis of Low Back Pain
Nonorganic low back pain also occurs and can be divided into several categories, including (1) psychosomatic spinal pain (tension syndrome- fibrositis, or muscle tension generated physiologically by anxiety), (2) psychogenic spinal pain (somatization of anxiety into neck or back pain with no physiologic changes, as in a conversion reaction), (3) psychogenic modification of organic spinal pain (an emotional reaction that modifies the appreciation of an organic pain), and (4) situational spinal pain (litigation reaction, conscious overconcern or exaggeration).15
A number of metabolic disorders can contribute to neuropathy, fracture, muscle tension, or associated depression/anxiety. These include electrolyte disorders, diabetes, thyroid, renal, and liver disease.
Current Standards of Care
A number of guidelines exist for the evaluation of patients with low back pain. The most prominent include those from the Institute for Clinical Systems Improvement,16 the Royal College of General Practitioners,17 and the US Veterans Administration.18
Evaluation of the Patient with a Diagnosis of Low Back Pain
The goal of diagnosis is to define the anatomic pain generator(s) as specifically as possible, recognizing that this is not always possible. Physicians should be aware that some patient presentations can be “diagnostic traps,” leading down an unhelpful treatment path.15 For example, pain from a facet joint can radiate down the leg and be incorrectly diagnosed as disk herniation. Other pathological conditions may become evident with time, such as the classic osteoporotic vertebral collapse that later is discovered to be caused by a metastatic lesion. Frequent and careful reevaluation is therefore vital, and failure to improve should prompt reassessment. On the other hand, if pain does not fit any known syndrome’s diagnostic profile, there may be other factors involved that interfere with diagnosis and/or recovery and need to be addressed.19
History
History taking must be approached in a careful, consistent manner. Key historical areas to be covered are summarized in Table 2. Physicians should specifically ask about prior treatments for low back pain and their effectiveness. Accurately assessing patients’ problems and expectations is a key to successful therapy.
Important Historical Factors in Evaluation of Patients with Low Back Pain
Physicians should constantly be alert for “red flags” and “yellow flags.” Red flags denote symptoms or physical findings suggestive of a potentially serious cause for pain that requires immediate evaluation.20 Examples include a history of progressive physical deficit, fever, pain at rest or at morning awakening without relief, distal numbness or weakness, or loss of bowel or bladder control with saddle anesthesia. High impact trauma is a risk factor for serious fractures and misalignments. Weight loss, fatigue, insomnia, and night pain can indicate malignancy with metastases to bone or chronic infection such as osteomyelitis. Spinal osteomyelitis can present with back pain, fever,21 and night sweats.22 In young patients with back pain, ankylosing spondylitis, spondylosis, and spondylolisthesis should be considered. A personal history of cancer, immune system deficiency, or the use of immunosuppressive medications such as corticosteroids increases the likelihood of a serious cause for the back pain.
Yellow flags denote adverse prognostic indicators.23 Examples include depressive symptoms, work-related injuries still in litigation, signs and symptoms not consistent with pain severity, and behaviors incongruent with underlying anatomic and physiologic principles. Yellow flags signal the potential need for more intensive and complex treatment and/or earlier specialist referral. Emotional stress has long been recognized as a contributor to pain and/or its perception.24–26 When yellow flags are present, clinicians need to be vigilant for deviations from the normal course of illness.
Physicians should be alert for signs of drug addiction or diversion in patients seeking pain medications. Worrisome behaviors include a history of known substance abuse, visits to multiple physicians, requests for specific medication(s), lost prescriptions, and multiple failed therapies. Inconsistent responses to dosage changes or patient resistance to switching to an approximately equipotent opioid are of concern.
Physical Examination
The physical examination should dovetail with the history to generate a working differential diagnosis. Key portions of the examination are summarized in Table 3. Examination should seek identifiable patterns of findings suggestive of a diagnosis as well as potential sources of referred pain. Skin examination may reveal an infection such as zoster or cancer. Palpation may reveal crepitus suggestive of fracture (often with severe point tenderness over bone), instability, myositis, myofascial trigger points, or visceral organ tenderness. Range of motion assessment may reveal functional deficits. Pain on upper body flexion and rotation can indicate facet arthropathy or other structural problems. Rectal examination can reveal prostatitis, sacral pathology, or colon cancer.
Important Components of the Physical Examination in the Evaluation of Low Back Pain
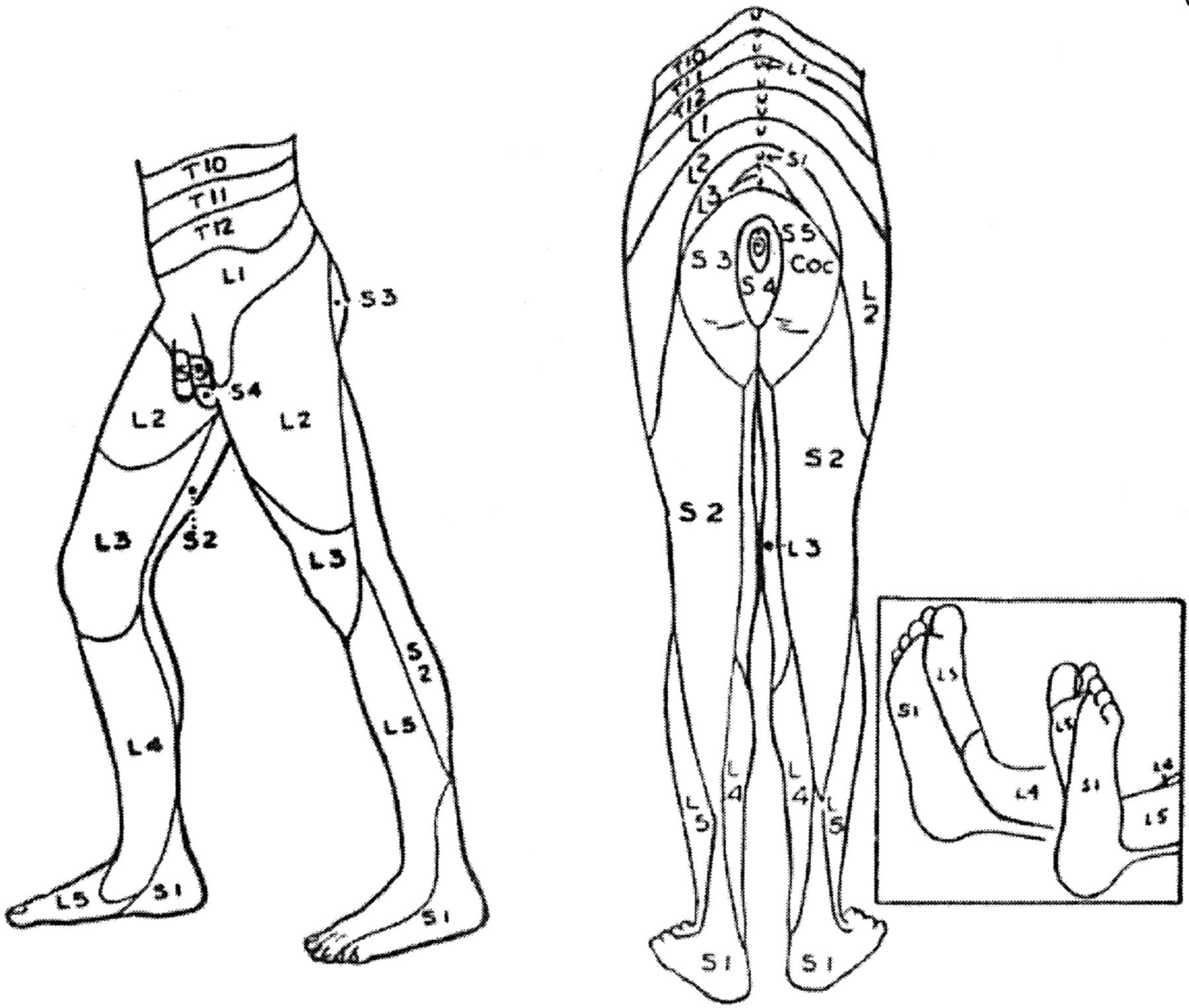
During neurologic examination (Table 4), vibratory deficit may indicate a neuropathic process. Dermatomal distribution (Figure 2) of pain suggests nerve impingement. Muscle weakness may also show a pattern indicating nerve impingement or, if diffuse, metabolic or central nervous system disease. Cerebellar signs and gait disturbances are important to any disability determination. Straight leg raise can reveal radiculopathy. Crossed nerve stretch can indicate peripheral nerve impingement.27

{kind=link}
{kind=link}
Sensory dermatomes of the lower extremities.
Important Components of the Neurologic Examination in the Evaluation of Low Back Pain
Waddell signs for nonorganic pain28 have been proposed to indicate a nonorganic pathogenesis of back pain. Signs include superficial nonanatomic tenderness, pain from simulation maneuvers that should not elicit pain, distraction maneuvers that should elicit pain but do not, regional disturbances not consistent with known patterns of pain, and over-reaction during examination. It is theorized that a greater number of signs present indicate a higher likelihood that a nonorganic cause of back pain is present. However, Waddell signs do not definitively rule out the possibility of organic disease. In a study of acute back pain in an occupational setting, patients with Waddell signs took a significantly longer time to return to unrestricted, regular work and used physical therapy and lumbar computerized tomographic imaging more frequently.29
Diagnostic Imaging and Testing
One goal of evaluation is to minimize unnecessary imaging studies that may generate potentially misleading information. Diagnosis can be confused by the high incidence of radiographic abnormalities in asymptomatic persons. On X-rays, 79% of patients between 50 and 65 years of age have narrowing, sclerosis, or osteophytes, and on magnetic resonance imaging (MRI), 14% of patients aged younger than 40 years and 28% of patients aged older than 40 years have major abnormalities.30 The majority of asymptomatic abnormalities on MRI are bulges and protrusions but not extrusions.31 Imaging studies should be ordered in patients with progressive neurologic deficits, failure to improve, history of trauma, and those at elevated risk for malignancy or infection.32
Several diagnostic tests can help diagnose malignancy or infection in patients with back pain.33 Serum or urine protein electrophoresis is the best initial diagnostic test for multiple myeloma given that many patients will have a normal bone scan.34 A history suspicious for vertebral cancer combined with an elevated erythrocyte sedimentation rate (ESR) has a positive correlation for vertebral cancer.35 However, the overall prevalence of malignancy in a study of hospitalized patients with an elevated ESR was only slightly higher (25%) than the prevalence in patients with a normal ESR (15%).36 Fever, elevated sedimentation rate, leukocytosis, and elevations in C-reactive protein level can all be indicative of infection. Blood cultures demonstrate bacteremia in up to 72% of cases of acute osteomyelitis.37,38 MRI is the most sensitive and specific test in identifying spinal infection.39
Management of the Patient with Low Back Pain
Once patients have been classified into a general category of back pain, management should follow the outline in Figure 1. “Red flag” conditions should be managed expeditiously and may require prompt specialist referral.
Drug Therapy
Most patients will have tried over-the-counter back pain remedies before seeking physician consultation. Initial therapy with acetaminophen, an nonsteroidal anti-inflammatory drug, or a cyclo- oxygenase-2–specific inhibitor is recommended (strength of recommendation A).40 Muscle relaxants can be effective when there is significant muscle spasm present, but benefits must be balanced with their sedative properties (strength of recommendation B).41,42 Tramadol can be an effective analgesic and has mild selective serotonin reuptake inhibitor properties, but side effects are common.43–46 An extensive body of evidence supports the effectiveness of short-acting opioids for moderate to severe pain (strength of recommendation A).47 Long-acting opioids are appropriate when other treatment modalities have been inadequate and the demonstrated improvement in functionality with the opioid therapy outweighs side effects.48 If pain is not responsive to opioid therapy or functionality does not improve, then the opioid should be discontinued. Adjuvant tricyclic antidepressants and anticonvulsants are effective in patients with underlying depression or a neuropathic component to their pain (strength of recommendation B).48 Amitriptyline has been most extensively studied in neuropathic pain, but its risks of sedation, anticholinergic side effects, and falls in elderly patients is higher than other agents within the class.49 Epidural corticosteroid injections are indicated only for radiculopathy (strength of recommendation B).50,51
Physical Modalities
After making an initial determination that a patient’s back pain is uncomplicated, physical modalities should be emphasized. Stretching, ice, and heat are all effective (strength of recommendation B).52–54 Although there is no definitive evidence supporting the effectiveness of massage, many patients find it helpful. There is limited evidence of the short-term effectiveness of manipulation (strength of recommendation B). After 6 weeks, all approaches seem to have about the same rates of success.55
Bed rest should be avoided, except possibly for the first 24 hours (strength of recommendation A).56,57 Patients should be encouraged to return to work and their usual activities as soon as possible (strength of recommendation A).58 Patients should be educated in proper posture, sitting position, and lifting techniques.
Beyond the acute phase, the choice of physical modalities is usually patient-specific, given the dearth of high-quality evidence supporting most interventions.58 Potentially beneficial therapies include exercise rehabilitation programs,59 electrical muscle stimulation,60 work hardening programs, and acupuncture.61 Transcutaneous electrical nerve stimulation (TENS) has not been shown to be effective for low back pain.62
Other Therapies
In appropriate clinical settings and selected patients, support groups, counseling, addiction therapy, or relaxation therapy can all improve outcomes.63 Treatment of coincident depression and anxiety can improve pain control.64 Some alternative treatments may potentially be of benefit, although firm evidence of efficacy is not currently available.65
Interventional Pain Management
Interventional pain specialists offer a variety of diagnostic and therapeutic options that may be helpful in the care of some patients. These include diagnostic facet and nerve blocks, therapeutic rhizotomies and nerve ablations, selective joint injections, epidural injections, intradiscal distraction therapy, and spinal endoscopy. Epidural steroids have been shown to be effective for pain with a significant inflammatory component, including nerve irritation or impingement.63 (strength of recommendation B) Referral to an interventionist is appropriate if a structural defect is likely and a procedure may help. Good communication between the family physician and interventionist is critical for the success of these procedures.
Confounding Factors in the Evaluation and Management of Low Back Pain
There are many potentially confounding variables (“yellow flags”) in the diagnosis and treatment of low back pain. It is common for patients to have a hidden agenda or set of beliefs that is not obvious to the physician. These may have an adverse effect on the outcome of treatment.
Certain beliefs and behavioral or cultural factors may consistently predict poor outcomes. These include:17
A belief that back pain is harmful or potentially severely disabling
fear-avoidance behavior and reduced activity levels
a tendency to depressed mood and withdrawal from social interaction
an expectation of passive treatment(s), rather than a belief that active participation will help
other factors that may interfere with recovery (anxiety, depression, unresolved occupational issues, prior disability claims).
Affective disorders are very common confounding factors in patients with chronic pain. Their concomitant treatment may improve outcomes.64
Opioid or benzodiazepine addiction and prescription drug diversion among patients with back pain can be very challenging. “Pseudoaddiction” is a patient behavior pattern often caused by undertreatment of pain. The patient initially seems to be drug seeking, but normal behavior returns with appropriate pain management.
Fibromyalgia and other complex pain syndromes often have low back pain as one of their symptoms. Their management is complex and beyond the scope of this article.
Conscious or unconscious secondary gain in a patient’s illness portends a poor outcome. Work-related back injuries and cases in which litigation is pending carry particular risk. Patient orientation toward treatment and improvement may determine the extent to which back pain responds to any therapy. The family physician has unique expertise in caring for undifferentiated problems, often in patients from different cultural backgrounds and value systems. Good communication and empathic understanding can enable the patient and encourage them to participate in their care.66 Familiarity with the patient and family can generate trust, encourage compliance, and uncover hidden agendas in patients with chronic back pain.
Lifestyle factors can be part of the original cause of the back problem and should be appropriately modified. Cultural factors and patient belief systems and values all affect openness to and response to therapy and should always be considered when developing a therapeutic plan.
Conclusions
Low back pain is extremely common. The most appropriate diagnostic approach is to look for specific biomechanical causes and identify potential anatomic pain generator(s) when possible. Most symptoms resolve relatively promptly with little intervention, but recurrence is common.
Patient history and physical examination are important in distinguishing potential etiologies and immediately identifying red flags denoting more serious conditions, as well as yellow flags that may confound both diagnosis and prognosis. Findings should be consistent with known pathologic processes. Pain that is inconsistent with known patterns of disease represents an important yellow flag and requires careful re-evaluation. Diagnostic imaging should be ordered only when truly necessary because of the high incidence of radiologic abnormalities in asymptomatic persons.
Once serious illness is ruled unlikely, first-line drug therapy with acetaminophen, a nonsteroidal anti-inflammatory drug, or a cyclo-oxygenase-2–specific inhibitor is recommended. Short-term use of muscle relaxants may be considered, but their benefits must be balanced with their sedative properties. Patients should be advised to stay as active as possible while continuing usual daily activities. In patients with complicating comorbid conditions, such as depression, appropriate therapy should be initiated. Opioids should be prescribed if other treatments have been insufficiently effective and there is demonstrated evidence of improved function that outweighs any impairment caused by adverse effects. Adjuvant antidepressants and anticonvulsants should be considered, especially in chronic or neuropathic pain and when coincident depression is suspected. If a structural defect is identified and a diagnostic or therapeutic procedure is available, referral should be considered. If symptoms have not resolved adequately within a 4- to 6-week period, reevaluation and additional diagnostic workup should be considered.
Acknowledgments
We acknowledge the contributions of the other members of the Family Practice Pain Education Project: Gail Cawkwell, MD, Alan Gibovsky, MD, Deborah Haynes, MD, Tanya Jones, MD, Laeth Nasir, MBBS, Trish Palmer, MD, Sunil Panchal, MD, Francine Rainone, MD, PhD, Knox Todd, MD, and James Toombs, MD.
Notes
The Family Practice Pain Education Project (FP-PEP) acknowledges an unrestricted educational grant from Pfizer to Cardinal Health to produce educational materials for primary care doctors about pain management. The information provided here is the opinions and research of the family physicians who served on FP-PEP.
This work was presented in part at the 2003 American Academy of Family Physicians (AAFP) Scientific Symposium.