
Abstract
Purpose: Sexual misconduct by physicians is a consequential violation of patient trust. The purpose of this study was to determine the frequency and patterns of sexual misconduct by physicians certified by the American Board of Family Medicine (ABFM).
Methods: We described a cohort of current or formerly ABFM certified physicians (“Diplomates”) disciplined for sexual misconduct in 2016 to 2022.
Results: Ninety-four physicians, representing only 0.1% of ABFM Diplomates, were identified as having received disciplinary action(s) for reported sexual misconduct. These constituted 8.9% of the 1122 cases that resulted in a physician losing board certification or eligibility for any cause in 2016 to 2022. Ninety-three of the 94 physicians identified as male, with an average age of 56 (range 22 to 88 years). Eighty-nine percent of victims were female, and 90% were patients of the physician. Unwanted sexual behavior/assault occurred in more than half of the cases, whereas one third described an ongoing sexual relationship between patient and physician. Nearly 1 in 5 cases also included controlled substance prescribing. Seven cases involved minors. Noncontact (“grooming”) behaviors were described in 34 cases, 28 of which included subsequent physical sexual behavior. A clinical setting was the site of misconduct in 84% of cases.
Conclusions: Reports of sexual misconduct among board-certified family physicians are infrequent. However, any sexual misconduct by physicians is harmful to patients and the profession. The specialty should work to enhance education and change professional culture to mitigate this important problem.
- Certification
- Family Medicine
- Family Physicians
- Medical Ethics
- Professional Misconduct
- Sexual Misconduct
- Specialty Boards
- Trust
Introduction
Sexual misconduct between physicians and their patients, first documented by Hippocrates,1 has proven intractable across history. However, structured institutional attention to the problem is a recent phenomenon. It was only in the early 1990s that the American Medical Association (AMA) and the Federation of State Medical Boards (FSMB) prompted medical license boards to initiate investigations into sexual misconduct.2⇓–4 By 1998, 23 states had established laws criminalizing sexual boundary violations by a physician, but it took until the early 2000s for regulatory bodies, organized medicine, and scholars to state that sexual contact with a current or former patient is never acceptable. Despite progress, physician sexual misconduct continues to occur within and outside of medical practice.2,5
Physician-patient relationships entail inherent power imbalances as patients share intimate information with physicians in whom they place their trust. Romantic relationships or sexual activity between a physician and patient violate such trust, regardless of any appearance of patient consent, while compromising the physician’s objectivity in decision making and risking patient harm.2,4,6 A sexual relationship with a former patient is similarly subject to potential exploitation of the trust, knowledge, emotions, or influence resulting from the earlier professional relationship.7 The impact of physician sexual misconduct is profound and enduring not only for patients, but their families, the public at large, and the medical profession.
A wide range of behaviors constitute sexual misconduct, including inappropriate noncontact communication (texting, personal phone calls), expressions of intimate or sexualized thoughts or feelings, violations of patient privacy during exams, physical contact not required for evaluation and treatment, ongoing physician-patient sexual relationships, unwanted sexual advances by the physician, or criminal sexual assault.4,8 Any of these may be accompanied by inappropriate prescribing of controlled substances or additional ethical violations such as financial fraud or bribery.9
Reliable data on the frequency of sexual misconduct is difficult to obtain. Under-reporting is likely, due to victims’ feelings of shame, fear of social stigma or retaliation, as well as lack of understanding of the role of state medical license boards (SMBs).10 A Harris Poll commissioned by the FSMB found that only one-third of patients who believed they experienced “unethical, unprofessional, or substandard care” reported the misconduct or filed a complaint with a SMB.11 Reticence to reporting is also found among medical professionals, who also fear retaliation, are reluctant to disrupt professional relationships, and are unsure of the accuracy of information they may have about a given case. Variation also exists across SMBs in their investigatory and regulatory capabilities to manage reports of sexual misconduct and their approaches to determine sanctions. Still, they remain the predominant public source of information about physician sexual misconduct. Studies regarding SMB sanctions for sexual misconduct have demonstrated increasing frequency over time, from 2.1% in 1989, to 5.2% in 1994, to 15% in 2020, as a percentage of total sanctions for professionalism violations.12,13
Among published studies, offenders share common characteristics: predominately male, over the age of 39, and in practice for more than 20 years. Victims are most often female patients ranging in age from 20 to 39 years.13⇓⇓–16 Use of a chaperone is reported to be less common in cases where sexual misconduct is discovered. Up to 70% of cases of sexual misconduct are reported to have occurred among nonboard-certified physicians.15 To date, no studies have reported on sexual misconduct or specialty board responses among a cohort of board-certified physicians.
We selected board-certified family physicians to study, as this specialty is the focus and responsibility for American Board of Family Medicine (ABFM), are the group for which ABFM has unique access to data, and for which it has authority to act in response to the behavior. ABFM routinely compiles this data in its review of potential violations of the ABFM Guidelines for Professionalism, Licensure, and Personal Conduct17 by ABFM certified or eligible physicians. This information is reported to ABFM by SMBs through the American Board of Medical Specialties’ (ABMS) Disciplinary Action Notification Service (DANS) reports of actions against physicians’ medical licenses. Procedurally, ABFM staff notify the physician if their certification is revoked based on a violation of the Guidelines. All physicians have appeal rights and those who choose to appeal have their case adjudicated by the Professionalism Committee of the ABFM Board of Directors, who may determine final sanctions, up to and including revocation of certification.
Methods
In this mixed-methods study, we analyzed cases of sexual misconduct from 2016 to 2022 by ABFM diplomates. This date range was selected because 2016 was the first year of complete data having been entered into ABFM’s data files. We selected cases in which the case summary included the terms “sexual boundary issues,” “sexual misconduct” or similar descriptors, and/or a requirement that the physician use a chaperone when seeing some or all patients.
We identified 146 files for initial review, 52 of which were eliminated when findings did not confirm sexual misconduct, or when the SMB action predated 2016. This resulted in 94 cases included in the present study. Two investigators (EB, SD) reviewed each FSMB report and individual SMB order, additional historic or subsequent professionalism or medical licensure records for the physician, materials submitted by those physicians who appealed the revocation of their ABFM certification or eligibility, and relevant ABFM Board of Directors Professionalism Committee meeting minutes. We obtained physician demographics from existing ABFM data.
All authors reviewed each case and categorized physician behavior by type of sexual misconduct. This was followed by group discussion to resolve discrepancies and consolidate types of behaviors into agreed upon categories for classifying cases.
The study group’s qualitative researcher (AK) conducted further data analysis using NVivo v12 qualitative analysis software to delineate component behaviors of each sexual misconduct category. If warranted by the case description, multiple boundary violations could be identified within 1 case. An additional inductive, focused review was conducted to clarify component behaviors of each category to identify emergent or previously overlooked behaviors. The study team discussed all refined categories for clarification, refinement, and consensus.
The American Academy of Family Physicians IRB deemed this study exempt from review.
Results
We identified 94 physicians as having engaged in sexual misconduct, and ABFM revoked board certification or eligibility in all cases. These represented 8.9% of the 1122 cases in which the physician lost board certification or eligibility in 2016 to 2022 and 0.1% of all ABFM certified physicians. DANS reports were the primary source of information regarding sexual misconduct received by ABFM. Only 8 physicians self-reported to ABFM, while 5 were discovered from media reports and then confirmed from SMB orders. Thirty (32%) of the 94 physicians appealed to the Professionalism Committee of the ABFM Board of Directors and 64 (68%) accepted the loss of certification or eligibility without appeal.
Table 1 provides further details about these cases. Compared with all ABFM diplomates, physicians in the sexual misconduct study were predominantly male (98.9% vs 55.3%, P < .001), slightly older (mean age, 55.8 [S.D., 12.4] vs 52.0 [S.D., 9.5] years, P < .001), and were more likely to practice in rural areas (25.0% vs 15.6%, P < .001). The majority were graduates of US allopathic medical schools, with no significant differences identified by medical training or degree type when compared with all diplomates during this same time period. The average time between initial certification and imposition of a SMB sanction was 17.5 years.
Description of 94 Cases of Sexual Misconduct by ABFM Certified or Eligible Physicians, 2016–2022
Eighty-nine percent of victims identified as female and were patients of the offending physician. Thirty-eight percent of cases involved multiple victims. Reporting of the behavior to the SMB was done by victims in 53% of cases, followed by law enforcement (41%), employers (14%), or the victim’s family (7%). In only 2 cases was the behavior reported by a colleague or staff.
We developed 5 categories of misconduct based on behaviors described in SMB orders, with an additional category for any case that involved minors. These descriptions, along with sample cases, are shown in Table 2. In more than half of the cases, physician behaviors included unwanted sexual behavior and/or assault, while one third described an ongoing sexual relationship between the patient and physician. Nearly 1 in 5 also included concomitant prescribing of controlled substance, while 3 cases included financial incentives to engage in, or cover up, the sexual misconduct. Seven cases involved minors, all among nonappeal physicians. In only 4 cases was the misconduct limited to noncontact behavior (phone, text messaging, social media, letters, etc.). However, these types of “grooming behaviors” were additionally described in 28 cases, typically preceding subsequent physical sexual behavior. The physician’s office or similar clinical setting (hospital, emergency department) was the site of sexual misconduct in 84% cases. In 36% of cases, the behavior occurred solely, or additionally, outside of a medical setting, most often in the victim’s or physician’s home. Physicians who did not appeal staff action to revoke certification tended to have more egregious behaviors described in their SMB orders and were more often found to have had previous sanctions against their medical license.
Categories of Sexual Misconduct by ABFM Certified or Eligible Physicians, 2016–2022
SMB sanctions for sexual misconduct included reprimand, probation, license restriction, or loss of a medical license. Loss of license occurred in nearly half of cases, with 20% of these physicians subsequently regaining their medical license. Among those who maintained their medical license, 22 were given a probationary period ranging from 3 months to 9 years, with an average of 5 years. A chaperone requirement was imposed in 27% of cases. Additional sanctions included prohibition from solo practice, or from caring for a subset of patients (eg, females), and limitations related to controlled substance prescribing. In 12 cases the medical license board issued only a reprimand, requiring CME in professional boundary and/or ethics in nearly half of cases. Nineteen percent were compelled to have a psychiatric evaluation and/or ongoing treatment, generally attached to a probationary status. Evidence of a criminal conviction for the sexual misconduct was found in 14% of cases. More than half of physicians experienced loss of employment and/or clinical privileges. Prior SMB sanctions were evident in 22% of cases, half of which were for previous sexual misconduct.
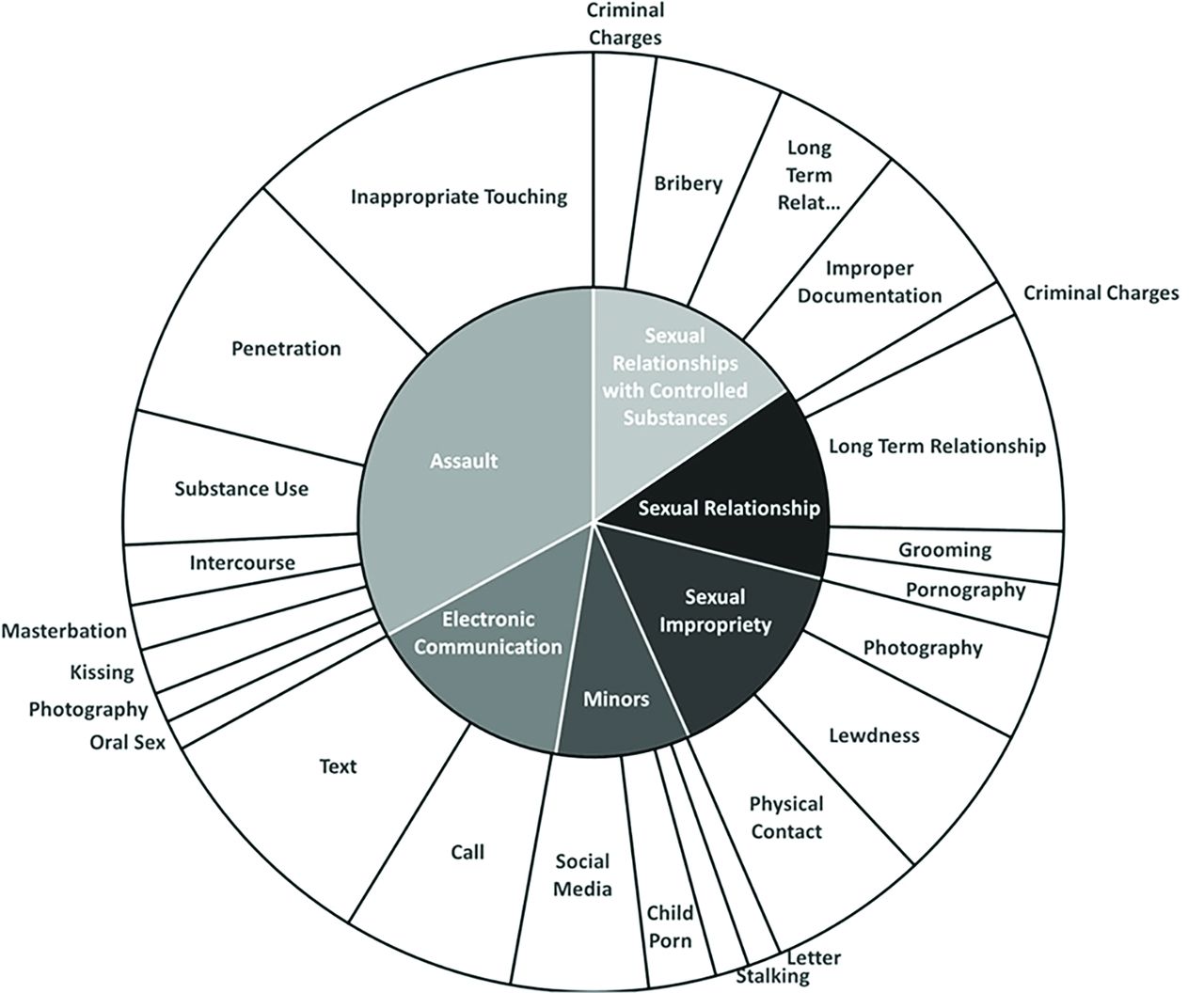
Figure 1 shows results of the qualitative analysis of SMB orders. Each inner ring represents a specific sexual misconduct code, and the outer rings describe component behaviors of each outer ring. Larger sections indicate greater occurrence of that behavior. Inappropriate touching during physical examinations was the most common behavior identified within assault cases. Sexual relationships were separated into those that involved controlled substance prescribing or bribery and those that did not. It is noteworthy that several cases within both categories occurred multiple times, often over multiple years. Noncontact communication most often included text messaging or phone calls, while inappropriate comments and behaviors represented the most common in-person behaviors. Cases involving minors included a range of behaviors, from possessing child pornography to physical sexual contact.

Sexual misconduct typologies nested pie chart. The outer ring contains component behaviors of each inner ring code. The size of each radial slice on both layers represents the relative frequency of occurrences.
Additional information was available in cases in which the physician appealed to the ABFM Professionalism Committee of the Board of Directors for reinstatement of their certificate. SMB orders in some of the appeal cases included information about whether or not the physician accepted responsibility for their behavior. Nine of the 14 physicians who engaged in a sexual relationship with a patient accepted responsibility, while 4 did not. Only 4 physicians whose behavior was categorized as assault accepted responsibility for their behavior while 12 did not. Cases often contained multiple sexual misconduct violations with varied component behaviors. For example, findings from one case began with a physician texting explicit and sexualized comments to a female-identifying patient which progressed to kissing and groping during her next office visit. This patient testified that she felt that this physician took advantage of her vulnerability.
Discussion
Reported sexual misconduct by board-certified family physicians occurs rarely, representing only 0.1% of all ABFM diplomates and only 8.9% of violations of any type reported to ABFM. This is in contrast to higher rates reported in SMB studies, building on data demonstrating that up to 70% of cases of physician sexual misconduct involve nonboard-certified physicians.
ABFM revoked certification for all 94 physicians identified in this report. The ABFM and its Board of Directors take this problem very seriously, with a low threshold for acting when an SMB investigation uncovers findings of sexual misconduct, in any form. Board certification is intended to serve as a credential above medical licensure, and it is the role of all ABMS member boards to set specific standards for being recognized as a board-certified physician. Sometimes, this means that a specialty board will act on the certification of a physician in a more significant manner than a licensing board. There are 70 independent SMBs in the US and its territories, and they often apply different sanctions for what seem to be similar behaviors. In determining who is to be presented to the public as board certified, ABFM strives to act consistently for all physicians based on its established and publicly available Guidelines for Professionalism, Licensure, and Personal Conduct.17
The characteristics of the physicians, victims, behaviors, and locations in this study mirrored those found in the literature. In cases where a sexual relationship was described, 1 in 5 included controlled substance prescribing and/or bribery. Although the higher numbers of cases involved physicians practicing in rural areas compared with all ABFM diplomates was statistically significant, this should be interpreted with caution given the small numbers. Finally, our findings illustrate how these violations involve complex, overlapping behaviors of multiple types.
Sanctions levied by SMBs were similar to those reported in other studies, with most having some period of license suspension, often time-limited, and followed by a probationary period that included chaperone requirements, completion of boundary and medical ethics courses, and personal psychiatric evaluation and ongoing counseling. SMB mandates to have all visits chaperoned or monitored for these physicians is presumed to offer protection for patients while the physician remains in practice during remediation and treatment, though the presence of a chaperone is not protective against this behavior.8 The FSMB has called for greater consistency in how physicians are investigated and sanctioned for sexual misconduct across individual SMBs.
Qualitative analysis suggests that more physicians who engaged in sexual relationships accepted responsibility than those who committed sexual assault, but no explanatory evidence is available. It is possible that physicians were unaware that engaging in a sexual relationship with a current or former patient was unprofessional until the behavior was reported, at which point they assumed responsibility. However, some of these cases also involved concurrent prescription of controlled substances, along with other behaviors that would be easily recognizable as boundary violations.
Limitations of the study include the relatively small number of cases over a 7-year time period and dependency on information received from SMBs and/or criminal convictions, which is often variable in the level of detail provided. If an SMB investigates alleged sexual misconduct and does not sanction a physician’s license, ABFM does not receive this information, perhaps adding to underreporting. In addition, trials are needed to demonstrate outcomes of preventive or remedial educational interventions.
While the numbers of offending physicians in this study is small, sexual misconduct is known to be underreported. Patients and employees are reluctant to report due to power dynamics inherent in the relationship, concerns about being wrong about what they perceived as misconduct, fear of losing their source of medical care, fear of retaliation, and potential loss of employment. Some SMBs have short deadlines for filing complaints, which can further the problem of underreporting. This contrasts with recent recognition by multiple states that victims of sexual assault may need extended time to process and recognize what has happened to them, resulting in extension or elimination of statutes of limitation on criminal and civil actions for sexual offenses.
A culture of silence among medical professionals and employers also contributes to underreporting that may allow these behaviors to continue. This is especially important in earlier stages of misconduct when there is potential to prevent grooming behaviors from progressing to more overt sexual behavior. Physician wellness programs, to divert physicians with substance use disorders into treatment and away from disciplinary proceedings were developed to overcome similar challenges around reporting of physician substance use. The establishment of state mandates that health care professionals report suspected sexual misconduct, such mandates for reporting suspected child abuse, with reporter immunity, were developed to overcome similar reluctance. It is unclear if SMBs have interest in applying such a solution to physician sexual misconduct. Until reporting can occur without concern for retaliation or other negative consequences, and with extended reporting windows, the true frequency and nature of sexual misconduct will remain unknown.
Prevention, not just reporting, is also important. Comprehensive efforts to prevent physician sexual misconduct should begin with undergraduate and graduate medical education, and given the average age of physicians in this study, must also be part of continuing professional development. While most physicians know that sexual assault is morally and ethically wrong, many do not appreciate the full scope of sexual misconduct, including grooming behaviors and having an intimate relationship with a current or former patient. The new Accreditation Council for Graduate Medical Education Program Requirements for Family Medicine Residency programs only address professionalism among competencies that are “not program requirements and are therefore not citable.”18 More robust training and assessment regarding the sacred trust between a physician and patient (with its accompanying vulnerabilities), as well as expectations of medical license boards, certifying boards, employers, and others, is critical. Beyond this, given that the majority of a physician’s career is spent outside of formal medical education, requiring continuing education in topics of professionalism and ethics may be warranted for all physicians, not just for offenders as part of a sanction for sexual misconduct.
Finally, although rates of reported sexual misconduct are lower among board-certified physicians, we believe certifying boards can serve a key role, above and beyond SMBs, to further reduce such misconduct. Family physicians have ongoing, continuous relationships with their patients, and serve as a trusted partner in caring for individuals and families. While important to address this among all specialties, it is critical to do so in a specialty where the strength of the bond between physician and patient is an important part of the therapeutic relationship. This is one of the reasons that ABFM reviews all cases of reported sexual misconduct, even where the physician is permitted by the medical board to retain an active license to practice.
Given the challenges of underreporting, investigating, and sanctioning offenders, the medical community must not be reassured by current rates of sexual misconduct reported in the literature. While this article specifically focused on board-certified or eligible family physicians, this is not merely a family medicine-specific problem. Rather, this discussion focuses on a preexisting reality that has plagued the entire profession of medicine for centuries. As such, it will take a combined effort of SMBs, specialty societies, certifying boards, physician employers, and others to address prevention, early recognition, reliable and transparent reporting, robust remediation efforts, and effective sanctioning of involved physicians to create a safer system of care for all patients. We should also shift the culture within medicine to expect reporting sexual misconduct by colleagues and staff, with assurances that this can be done without personal or institutional retaliation. This will require a renewed emphasis on professional self-regulation and the social contract that medicine has with patients and the public, and the time to do so is now.
Acknowledgments
The authors acknowledge the helpful editorial suggestions provided by Andrew Bazemore, MD, MPH and the data support of Lars Peterson, MD, PhD.
Notes
This article was externally peer reviewed.
Funding: No financial support was provided for this study.
Conflict of interest: The authors have identified no conflicting or competing interests.
To see this article online, please go to: http://jabfm.org/content/37/4/698.full.
- Received for publication November 13, 2023.
- Revision received January 10, 2024.
- Accepted for publication February 5, 2024.




{kind=link}