Abstract
Purpose: Social determinants of health (SDoH) including insecure access to food, housing, and financial resources are critical threats to overall health. We sought to examine this relationship among adult primary care patients with multiple chronic conditions.
Methods: We obtained cross-sectional data on 2763 adults with chronic medical and behavioral conditions or greater than 2 chronic medical conditions from a survey of participants in Integrating Behavioral Health and Primary Care, a multicenter randomized trial.
Results: The prevalence of 1 or more insecurities was reported in 29% of participants, including food (13%), housing (3%), or financial (25%). Functional capacity ranged from 2.74 to 9.89 metabolic equivalents (METs) (median, 6.05). The distribution of functional capacity was significantly lower for those with any 1 or more SDoH than for those without. Each insecurity independently affected the functional capacity in multivariable analysis.
Conclusions: Among primary care patients with chronic conditions, SDoH are associated with poorer functional capacity, independent of other social and demographic factors. Primary care offers a promising, if underused, opportunity to intervene in SDoH. There is a need for future studies to explore the role of screening and intervention by primary care providers to mitigate or prevent SDoH.
- Chronic Disease
- Cross-Sectional Studies
- Multiple Chronic Conditions
- Primary Health Care
- Social Determinants of Health
- Social Problems
- Surveys and Questionnaires
Introduction
Social determinants of health (SDoH), including food insecurity, housing instability, and financial hardship, are common in the United States,1 disproportionately impact vulnerable populations, and are associated with poor health outcomes. One in 8 US households are food insecure,2 0.2% of US adults are homeless,3 and 12% are living in poverty.4 Food, housing, and financial insecurities are more common among women, African Americans, younger adults, and those with lower education or chronic conditions.5⇓⇓⇓–9 Food insecurity is independently associated with obesity,10 peripheral artery disease,11 hypertension,12 hyperlipidemia,12 diabetes,13 medication underuse,14 and overall poor health.15⇓–17 Both food insecurity and housing instability are associated with sleep disorders,18,19 social isolation,20 cardiovascular disease,7 and poor overall physical and mental health.18,21⇓–23 There is extensive evidence of the negative effects of financial hardship and poverty on health and access to care.24 Poor health outcomes, financial hardship, and food insecurity are worse in rural areas than urban areas,25⇓–27 although mechanisms differ.
Poor functional capacity is a common physical limitation among the chronically ill and a major risk factor for mortality.28⇓–30 Exercise capacity, a measure of functional capacity, is the maximum sustainable amount of physical exertion. It is typically measured by the amount of oxygen consumed during maximal exercise, often presented in metabolic equivalents (METs). One MET is the amount of oxygen consumed at rest (3.5 mL O2 per kg body weight × min).31 METs can also be estimated from questionnaires such as the Duke Activity Status Index (DASI).32,33 Like other aspects of functional status, functional capacity may influence access to food, housing, and financial resources, often through employment. Conversely, poor diet, unstable housing, poverty, and inability to access care and medications may influence functional capacity. These relationships are often exacerbated among chronically ill populations.7 Despite evidence of a relationship between SDoH, cardiovascular disease, and other health outcomes, the relationship between SDoH and functional capacity has yet to be examined.
Building on prior literature, we sought to characterize the relationship of SDoH, in particular food insecurity, housing instability, and financial hardship, with functional capacity, among highly vulnerable adult primary care patients with chronic medical and behavioral conditions. We hypothesized that the presence of 1 or more SDoH will be associated with reduced functional capacity. Further, we hypothesized that food insecurity, housing instability, and financial hardship will each be independently associated with reduced functional capacity.
Methods
Our primary analysis modeled functional capacity in relation to the presence of any 1 or more insecurities. Our secondary analysis characterized the independent effects of each insecurity (food, housing, and financial) on functional capacity. Finally, a tertiary analysis modeled functional capacity as a function of the total number of SDoH (0 to 3).
Data and Setting
We used baseline survey results from Integrating Behavioral Health and Primary Care, a multicenter randomized study of chronically ill primary care patients from 2016 to 2021, described in detail elsewhere.34 Baseline data were collected before the COVID-19 pandemic. Data were collected from 4023 adults with multiple chronic conditions (arthritis, obstructive lung disease including emphysema, chronic bronchitis or asthma, nongestational diabetes, heart disease manifested as heart failure or hypertension, mood disorder [anxiety or depression], chronic pain [including headache, migraine, neuralgia, fibromyalgia, or chronic musculoskeletal pain], insomnia, irritable bowel syndrome, and substance misuse [substance use disorder, tobacco use, or problem drinking]) from 44 primary care practices across 13 states. To be eligible for this study, participants needed to have either at least 1 chronic medical and 1 behavioral health condition or greater than 2 chronic medical conditions. Participants also needed to be an active patient of a participating study practice as evidenced by at least 2 visits in a period of 24 months for any purpose, including at least 1 in the most recent 6 months. The presence or absence of each qualifying condition, and the dates of office visits, were determined by review of electronic health record visit data, problem lists, medication lists, and laboratory results.
The primary outcome was functional capacity measured by the DASI,32 a 12-item questionnaire that assesses the ability to do self-care, housework, sports, and other activities. The DASI generates an estimated maximal oxygen consumption, which correlates with results of treadmill testing31⇓–33 and long-term health outcomes in chronically ill patients.29,35,36 We converted the DASI to METs (0 to 9.89), where higher METs indicate better functional capacity.
SDoH was captured using 4 yes/no questions (see Table 1). The primary predictor variable was a binary indicator of the presence of any 1 or more of the 3 insecurities (answered yes to any of the 4 questions in Table 1). Food insecurity and financial hardship were captured using 1 question while housing instability was captured using 2 questions. A count variable was created representing the number of SDoH insecurities (food, housing, or financial) present (0 to 3).
Social Determinants of Health
Potential covariates associated with both SDoH and functional capacity were chosen based on clinical knowledge and prior literature. Person-level demographic covariates included age, sex (male vs female), race (white, black or African American, Asian, other), ethnicity (Hispanic vs non-Hispanic), marital status (married vs not), employment status (employed vs not), annual household income (in 7 categories), and education (in 6 categories). We also included medical and behavioral conditions (present vs absent) as potential covariates in the model including arthritis, obstructive lung disease, nongestational diabetes, heart disease, mood disorder, chronic pain, insomnia, irritable bowel syndrome, substance misuse, and medication adherence measured by the Morisky Medication Adherence Scale.37
Each participant's home address was mapped, and various neighborhood covariates were identified for potential inclusion in the final models. The Social Deprivation Index38 (SDI) is a census tract-level composite measure of deprivation based on income, education, employment, housing, single-parent household, and access to transportation. Census tract urban/rural status was based on Rural Urban Commuting Areas,39 which are derived from population density, urbanization, and daily commuting. Population density was assigned from their home census tract.
Potential practice-level covariates included information on behavioral health services, specialty, volume of encounters, type (nonprofit, academic, private), percent of patient population on Medicare, and county-level demographic measures (age, sex, race, income, employment, education).
Statistical Analysis
We used Wilcoxon rank-sum tests to compare the unadjusted distribution of functional capacity between those with and without 1 or more SDoH. Multilevel linear regression models were used to estimate the mean difference in functional capacity in METs by SDoH (with its 95% CI). Practice was included as a random intercept to account for correlation of patient-level measures within the primary care practice in which they were recruited. All predictors and covariates were included as fixed effects. The primary analysis modeled the effect of any 1 or more SDoH on functional capacity. Secondary analyses were independently performed for each of food, housing, and finance and the total number of insecurities. We repeated the main analysis while restricting the sample to those who met criteria for specific subgroups.
For the sake of parsimony and model reduction, covariates (described above) were included in the final model only if they changed the coefficient of SDoH on functional capacity by more than ±10% in a model containing only 2 predictors (SDoH and the covariate). All tests were 2-tailed and the threshold for statistical significance was α = 0.05. Stata 16.1 (StataCorp LP, College Station, Texas) was used for data management and statistical analysis. The University of Vermont Institutional Review Board approved this study.
Results
Two thousand seven hundred sixty-three participants were available for analysis. One or more insecurities were reported by 28%. Financial hardship was the most prevalent (25%), followed by food insecurity (13%) and housing instability (3%). Most participants with an insecurity only had 1 (19%), 8% had 2 insecurities, and 1% had 3 insecurities. Participants with any insecurity tended to be younger, black or other race, female, not married, not working, lower income, less educated, and living in socially deprived, densely populated areas compared with those without an insecurity. Most chronic diseases were more prevalent among participants with insecurities (see Table 2). Functional capacity ranged from 2.74 to 9.89 METs (median, 6.05; interquartile range, 4.73–7.99).
Characteristics of Population Stratified by Any One or More Social Determinants of Health (SDoH) Insecurity (n = 2763)
The final sample had missing information on 249 (8%) of records, of which 229 were missing data on METs and 64 were missing information on some or all of the SDoH. In the final multivariable models, there was 12% to 13% missing data. The records with missing data that were excluded from the final models did not significantly differ from those with complete data in terms of age, sex, race, ethnicity, functional capacity, and SDoH.
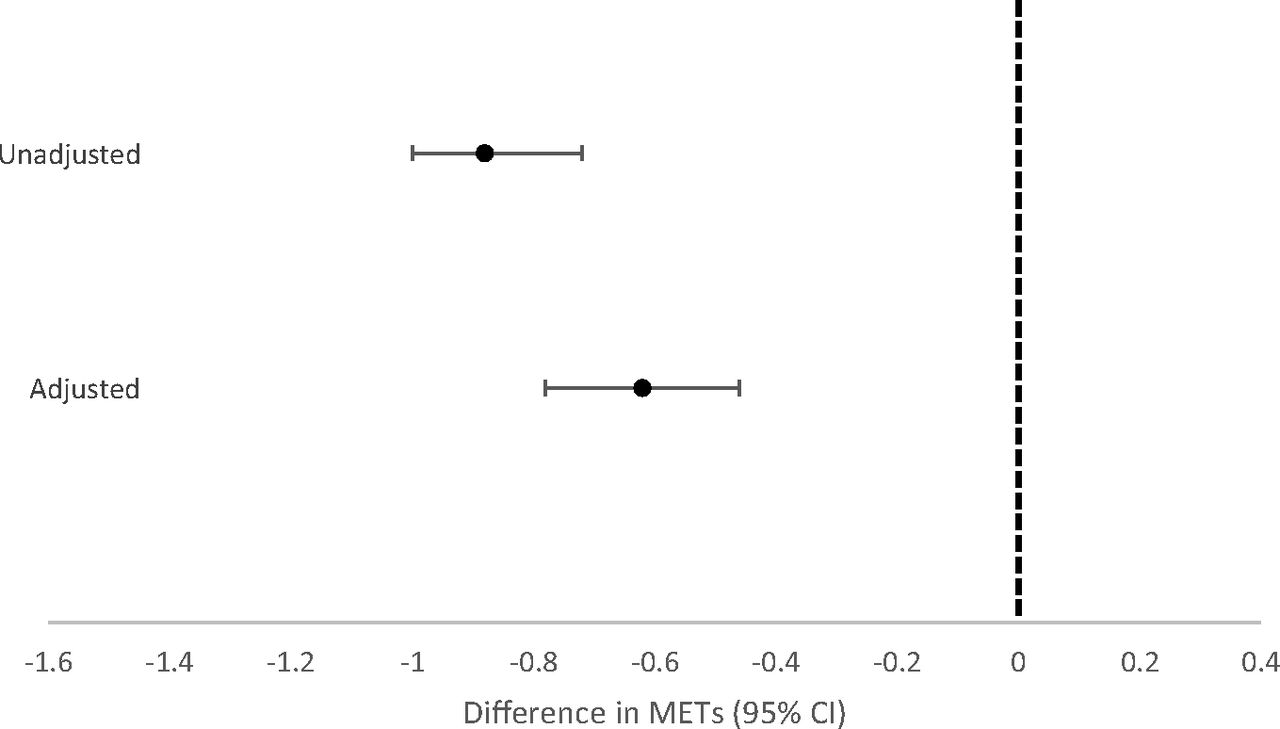
The unadjusted effect of any or more SDoH on functional capacity was −0.88 METs (95% CI, −1.02, −0.74; P < .001; see Figure 1). Age, marital status, income, total count of chronic conditions, and census tract SDI all modified this coefficient by more than 10% and were included in the final model. In a multivariate analysis, the effect of any SDoH was −0.62 METs (95% CI, –0.78, −0.46; P < .001; see Figure 1).

Difference in functional capacity associated with any 1 or more Social Determinants of Health (SDoH) insecurity. Regression coefficient and 95% CI for the mixed linear regression with and without adjustment for all potential confounders that met the 10% inclusion criteria. The vertical line at zero represents a null association. Abbreviation: CI, confidence interval.
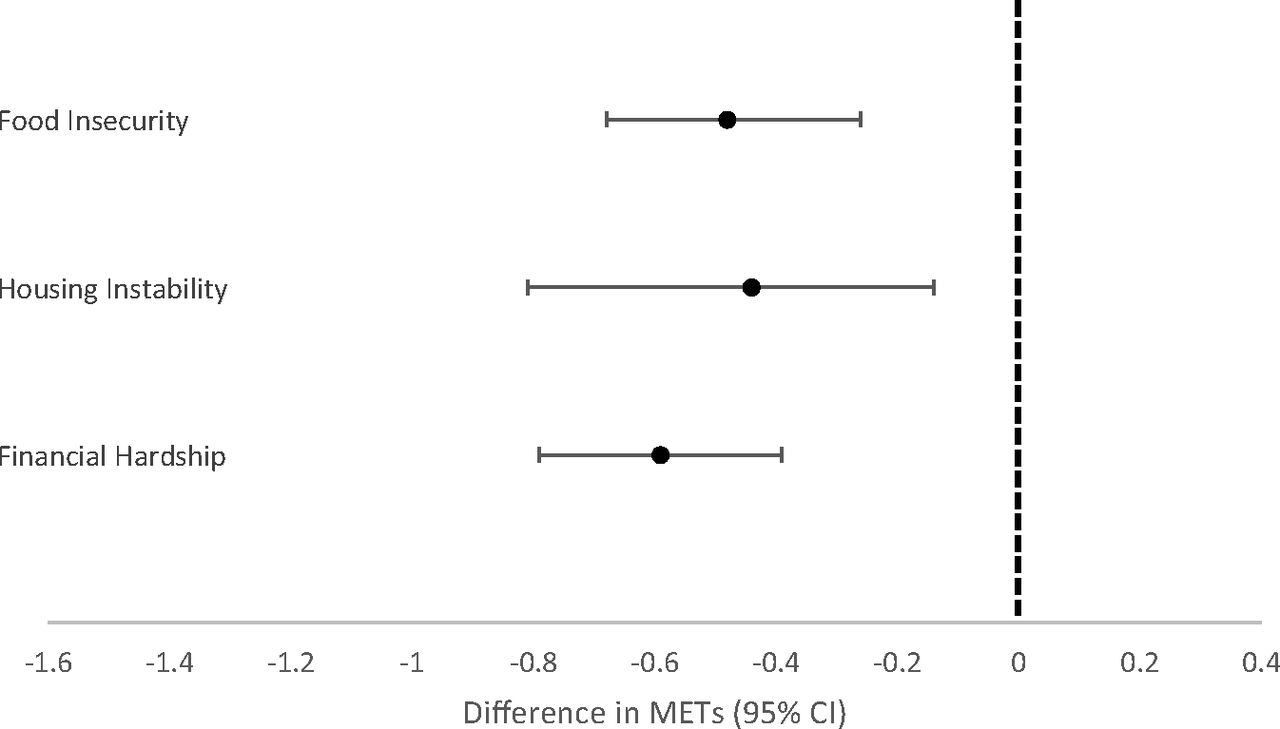
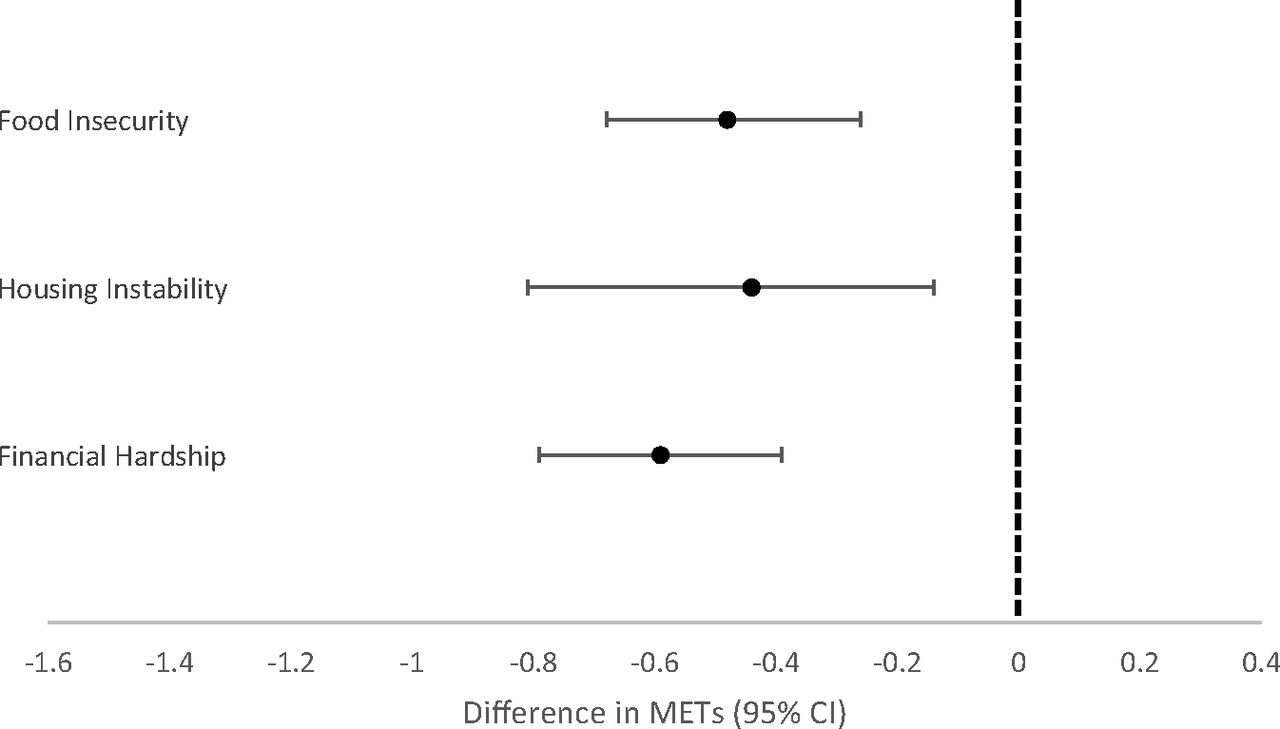
The unadjusted effects of food, housing, and financial insecurities on functional capacity were −0.75 METs (95% CI, −0.97, −0.53; P < .001), −0.60 METs (95% CI, −1.00, −0.20; P = .003), and −0.84 METs (95% CI, −1.01, −0.67; P < .001), respectively. Age, marital status, income, education, and total count of medical and behavioral conditions all modified the coefficient by more than 10% and were included in all 3 models. In addition to these variables, mood disorder and census tract SDI were included in the final food insecurity mode; urban/rural status, population density, mood disorder, and arthritis were included in the housing instability model; and census tract SDI was included in the financial hardship model. In multivariable models, food, financial, and housing insecurities were associated with a reduction in functional capacity of −0.48 METs (95% CI, −0.68, −0.27, P < .001), −0.44 METs (95% CI, −0.81, −0.08, P = .02), and −0.59 METs (95% CI, −0.76, −0.43, P < .001), respectively (see Table 3 & Figure 2).
{kind=link}
{kind=link}
Difference in functional capacity associated with food insecurity, housing instability, and financial hardship. Regression coefficient (β) and 95% CI for the mixed linear regression with adjustment for all potential confounders. The vertical line at 0.00 represents a null association. Abbreviation: CI, confidence interval.
Univariate and Multivariable Regression Results
The number of insecurities had a dose-response relationship with functional capacity. In unadjusted models, each additional insecurity reduced functional capacity by −0.51 METs (95% CI, −0.61, −0.41, P < .001). Age, marital status, income, total count of chronic conditions, and census tract SDI all modified the coefficient by more than 10% and were included in the final model. In multivariable analysis, each additional insecurity resulted in a reduction in functional capacity of −0.38 METs (95% CI, −0.48, −0.28, P < .001; see Table 3).
Discussion
We used a cross section of patient-reported surveys collected from a multicenter randomized trial of adult primary care patients with multiple chronic conditions to investigate the relationship between SDoH and functional capacity. We found that the presence of 1 or more insecurities resulted in a loss of 0.62 METs or roughly 10% of total functional capacity. This is roughly equivalent to being able to walk briskly (3.4 MPH) versus walking at a leisurely pace (2.5 MPH). We also found that food insecurity, housing instability, financial hardship, and the total number of insecurities were each independently associated with functional capacity.
Our findings are consistent with literature showing that SDoH negatively affects health, especially for younger age groups, females, and those with lower education and more chronic illnesses.5⇓⇓–8 Previous studies have shown food insecurity, housing instability, and financial hardship were related to functional disease and lung disease but not stroke.7 Further, SDoH are associated with behavioral and biomedical risk factors for cardiovascular disease.40 This study expands on these findings by confirming this association among primary care patients with multiple chronic conditions and investigating the specific functional outcome of functional capacity.
Improving functional capacity has the potential to help improve physical activity and maintain independence and aging in place for older adults, reduce health care costs, and improve quality of life. Because we saw an association between SDoH and functional capacity in this population, we posit that improving SDoH (whether it be food, housing, or financial) could potentially improve functional capacity. Future longitudinal studies should address this question to confirm a causal link.
The mechanism of the association between SDoH and functional capacity is complex. Food insecurity can reduce consumption and change the foods eaten.41 Cheaper, energy-dense food tends to be higher in calories, sugars, and fats42,43 and may contribute to the development of chronic diseases such as diabetes and hypertension,12,13 which can lead to reduction in functional capacity. Food insecurity is associated with decreased physical activity, potentially related to conserving energy.44 Housing instability and financial hardship can reduce access to care and medications, leading to chronic diseases and poor functional capacity. Another commonly proposed mechanism is that SDoH increases stress, resulting in high cortisol levels that can lead to heart disease and poor functional capacity.45
The prevalence of food insecurity in our sample was similar to national estimates, but housing instability was higher than estimates of homelessness and financial hardship was higher than national estimates of poverty. These findings could be unique to our sample of chronically ill adults or due to the various ways housing and financial insecurity are measured and defined. Food insecurity is ubiquitously defined as “limited or uncertain availability of safe and nutritionally adequate food.”46 In our sample, the prevalence of food insecurity was 11% compared with an estimated 12% in the general US population.2 There are, however, no standard definitions for housing instability or financial insecurity.
Housing instability has variously been defined as frequent moves, difficulty paying rent, spending more than 50% of income on rent, overcrowding, and number of evictions.47,48 In our survey, housing instability is comparable to homelessness and significantly higher than national averages (3% compared with 0.2%), perhaps due to the population being chronically ill and older.
Similarly, financial hardship has been defined directly in terms of consumption (as in our question) or indirectly in terms of income. The prevalence of financial hardship was 24% in our sample compared with national poverty estimates (12%). Our financial hardship question focused on difficulties in paying for life necessities, which may occur more frequently than poverty based on income. Alternatively, our population may suffer more financial hardship than the general population due to chronic illnesses.
Previous studies have shown that individuals with food insecurity, housing instability, and financial hardship are more likely to have access to care problems.7,47 However, our population is unique in that participants have evidence of access to care, suggesting different mechanisms are in play. Perhaps this chronically ill population prioritizes access to care over other necessities such as food or housing. Access to care alone may not be enough to combat SDoH challenges and related sequelae.
Race and structural racism are well documented to be associated with SDoH and health inequities.49⇓–51 Our findings indicate that not only is SDoH associated with function but the effects of SDoH on functional capacity exist above and beyond those mediated through race. In other words, SDoH and race seem not to be proxies for each other. To improve patient functional status and quality of life, it may be important to address SDoH and racism jointly.
This study has important limitations. Although the data were collected from patients with chronic conditions from diverse parts of the country, the results may not be generalizable to other populations and settings, such as those without access to care. Second, because this is a secondary analysis, it used a limited definition of SDoH. We did not have information on transportation challenges, violence, the built environment, or social justice challenges. However, we did obtain robust data on the 3 SDoH that were measured. Third, much of the data, notably the estimates of functional capacity, were self-reported. However, the DASI has been validated multiple times, including in chronically ill patients.29,35,36 Fourth, the cross-sectional nature of the study limits causal inference. For instance, although these data support the hypothesis that SDoH impacts functional capacity, they are also consistent with the reverse (functional capacity determines SDoH). Although we controlled for several potential confounding influences, we cannot eliminate the possibility of an unmeasured confounder. For instance, we did not have data on health insurance. However, all participants received care, indicating good access. Finally, data were missing from 13% of records in the final models. Fortunately, these records did not significantly differ by SDoH, functional capacity, or demographics from those that were included.
Primary care offers a promising, if underused, opportunity to intervene in SDoH. Although primary care physicians understand that social factors influence health, many avoid asking about them,52 and many primary care practices have not invested in developing platforms to address SDoH.53 Nonetheless, strategies to address SDoH in primary care are emerging.54,55 There is a need for future studies to explore the role of screening and intervention by primary care providers to mitigate or prevent SDoH.
This is the first analysis of SDoH and functional capacity. It shows that the presence of 1 or more SDoH is associated with lower functional capacity in primary care patients with multiple chronic conditions and suggests primary care as a fruitful setting for intervening.
Notes
Funding: This work was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (PCS-1409-24372). The views, statements, and opinions presented are solely the responsibility of the authors and do not necessarily represent the views of PCORI or its Board of Governors or Methodology Committee.
To see this article online, please go to: http://jabfm.org/content/34/4/688.full.
- Received for publication January 7, 2021.
- Revision received February 25, 2021.
- Accepted for publication March 11, 2021.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.