
Abstract
There are many words for what physicians commonly refer to as Somatoform Disorder. However, none is particularly patient-centered; to greater or lesser extent, they are all framed by medical jargon. Based on his experience as a seasoned clinician, the author suggests family physicians consider adopting the word PRESSS—an acronym for “Physical Reaction to Emotional Stress of Some Sort”—when describing and explaining to patients with Somatoform Disorder the cause of their suffering. Using examples from practice, the author notes how PRESSS combines simplicity, ambiguity, and directness in one non-stigmatizing, patient-focused word. Combined with a patient-centered manner of communication, the use of PRESSS can help create the kind of shared therapeutic presence that is so important when attending to patients who experience the bothersome, unrelenting symptoms these conditions suggest.
- Behavioral Medicine
- Counseling
- Diagnosis
- Family Medicine
- Family Practice
- Medically Unexplained Symptoms
- Mental Health
- Patient-Centered Care
- Physician-Patient Relations
- Primary Health Care
- Psychiatry
- Somatoform Disorders
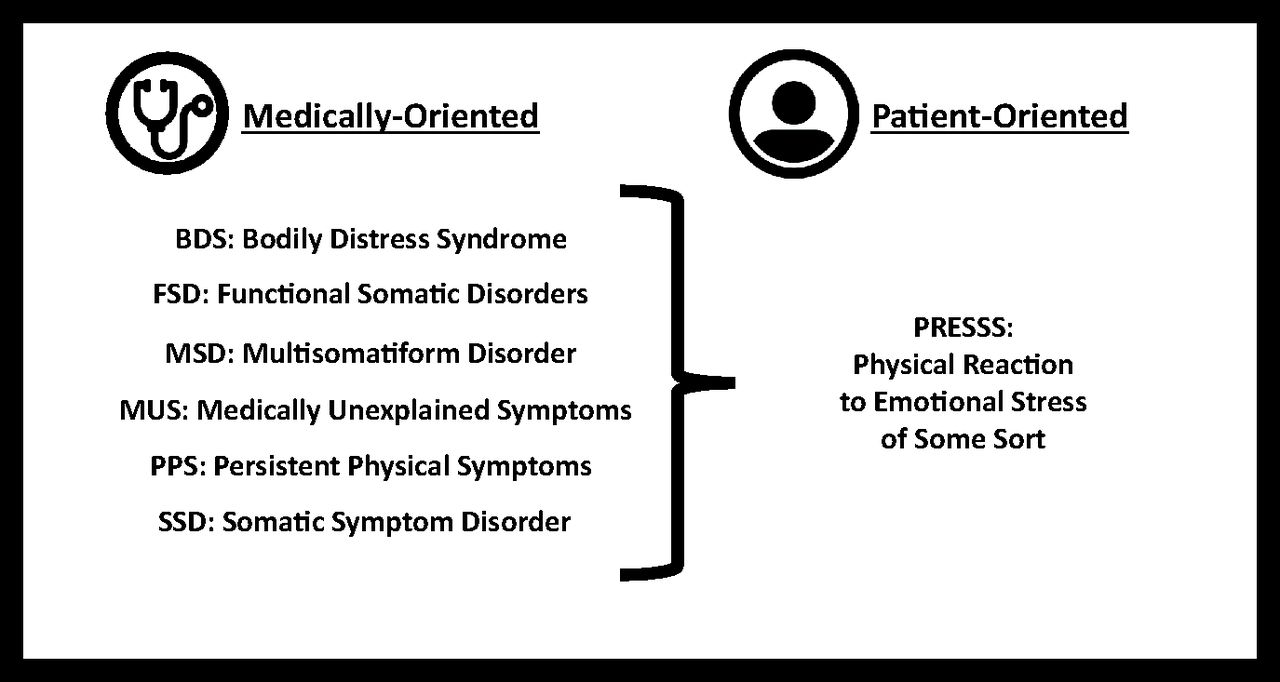
It is a diagnosis we as family physicians frequently encounter in our work1: Somatoform Disorder or Functional Disease. These were the names I learned years ago in medical school, both having replaced the previously used pejorative terms “neurasthenia” and “hysteria.”2 Later, generalists in the United States introduced the less stigmatizing monikers Medically Unexplained Symptoms and Multisomatiform Disorder into the literature.3,4 Clinician scholars in Europe suggested alternative expressions: Functional Somatic Disorders, Persistent Physical Symptoms, and Bodily Distress Syndrome.5⇓–7 Much more recently, the DSM-V recommended as the “umbrella” diagnostic label Somatic Symptom Disorders, with 4 accompanying subclassifications: Somatization Disorder, Undifferentiated Somatoform Disorder, Pain Disorder, and Hypochondriasis.8
Each of these names represents terms for conditions typified by bothersome, unrelenting physical symptoms (including, among others, pain, food intolerance, shortness of breath, fatigue, and dizziness). None can presently be explained by any 1 or more specific medical conditions. All are commonly triggered by adverse social, psychological, and neurological stimuli.9 The Biopsychosocial approach,10 psychodynamic theory,11 and recently introduced concepts of neural pathways notwithstanding,12 these names reflect our current lack of understanding of how exactly minds and bodies function in concert with one another. However, they are all formulated from a professional point of view, framed by using at least some medical jargon. I do not believe any does justice to patients' perspectives on their conditions.
Given these considerations (and after an appropriate, judiciously applied clinical investigation to rule out potential biological etiologies for the symptoms), I propose that we as family physicians adopt the word PRESSS—an acronym for “Physical Reaction to Emotional Stress of Some Sort”—to describe and explain to patients the conditions that the many terms noted above attempt to address. (Figure 1).
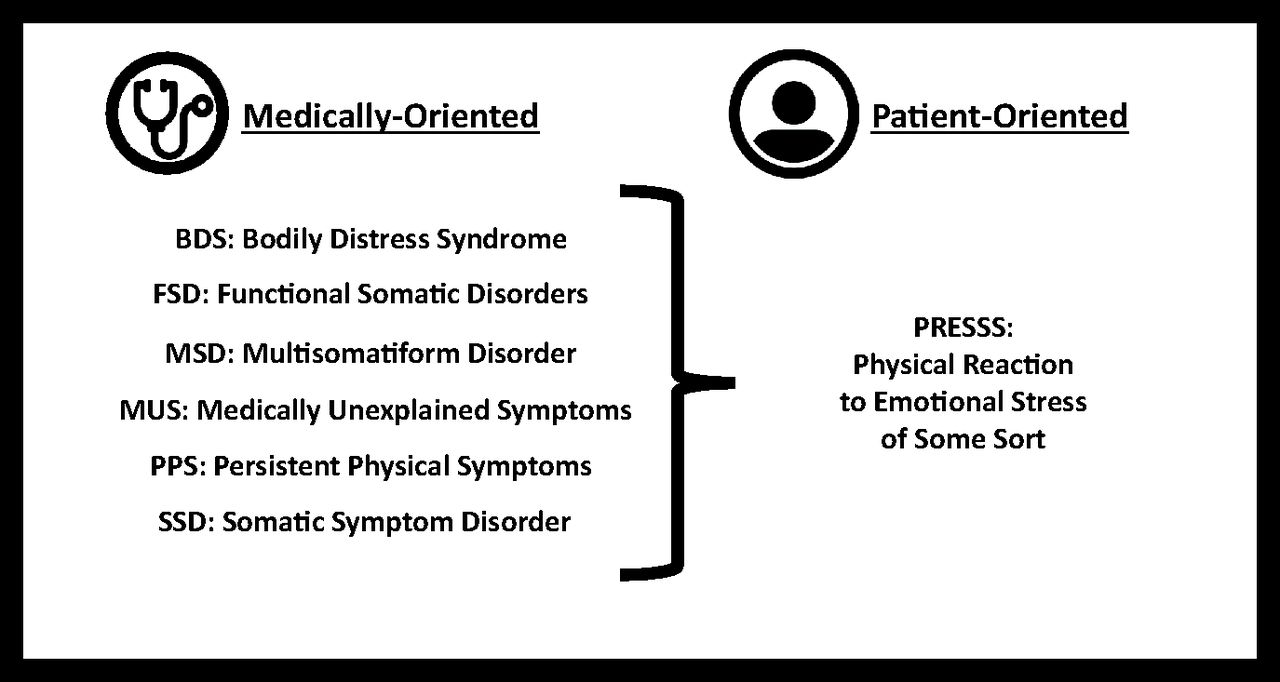
Differentiating PRESSS from Medically Oriented Acronyms.
I commonly use PRESSS in my practice with patients, as in this example situation:
“Ms. Doe, we have investigated what is going on, and while I will continue to explore other causes for your problems, I suspect what you have is a condition called PRESSS—you are experiencing is a ‘Physical Reaction to Emotional Stress of Some Sort.’”
“I wonder,” I continue after a moment of silence to gauge my patient's reaction, “whether have experienced any stress in your life? Or whether you may be experiencing any now?”
Or, using a characteristic pause and probe style13: “Might that explain your problems?”
Or, simply: “Does that ring true to you?”
The advantage of using PRESSS with patients is that it simultaneously balances simplicity, ambiguity, and directness in 1 non-stigmatizing, patient-focused word. First, PRESSS is easy to remember, even when the specific implication of each letter is forgotten in the fog of anxiety and fear that often accompanies patients to their visits with me. I am prone to write “PRESSS” on the examination room whiteboard when reviewing my diagnosis with patients, sequentially commenting on each letter for emphasis. Second, although “of some sort” correctly suggests a lack of exact clarity as to the elements at the root of physical symptoms, its vagueness intentionally invites patients to explore how emotional concerns might contribute to their origin. I purposefully inquire as to patients' perceptions and worries. Third, PRESSS clarifies the connection between emotional and physical, important when patients want some kind of answer to their presenting concerns. I often add, “the mind and the body are not so far apart” when an explanation is in order. I also commonly note that while I cannot for a fact tell the patient what the cause, or “on/off switch,” is, I am sure that emotional reactions act as a kind of “rheostat” or “dimmer” that, when turned up, can worsen symptoms.
The use of PRESSS will not eliminate all the challenges that arise when evaluating or communicating with patients. It will not prevent the conviction among some for whom the essence of the problem is primarily neurophysiological in nature, and for that reason, I am not suggesting substituting PRESSS for other biomedically-oriented terms either in our discussions with colleagues or in the professional literature. Still, whatever one may call it, patients who present with the vague, undifferentiated physical symptoms typical of PRESSS suffer, and the physicians who attend to them often feel frustrated. On both sides of the stethoscope, these issues can cloud abilities to visualize any movement toward understanding, let alone health.
I readily admit my use of PRESSS with patients may be irrelevant to whether they comprehend their symptoms better or can cope with more success. Any improvement in their distress may have less to do with the words I use than how I use them to invite the creation of a shared healing presence between my patients and me.14 Now, over thirty years into post-residency practice, key communicative approaches I long ago learned to use with such suffering patients still ring true. They may very well be more critical to my patients' clinical progress than my choice of PRESSS over other acronyms:15
Take patients' complaints seriously (while attending to cues of emotional distress).
Discuss physical and psychosocial issues with respect for patients' opinions.
Suggest how emotions and symptoms may be linked (noting how addressing the former can improve the latter).
Negotiate diagnostic and treatment plans, balancing hope with reality.
Help patients feel understood.
I can say that many of my patients to whom I offer the diagnosis of PRESSS meet it with less resistance than those with whom I used other words in the past. They seem to make sense of their condition with more awareness and leave the clinic examination room with more hope. So, too, do I. For that reason, I will continue to speak of PRESSS in my encounters with patients. I invite other family physicians to consider using it in theirs.
Notes
This article was externally peer reviewed.
Funding: None.
Conflict of interest: None.
To see this article online, please go to: http://jabfm.org/content/34/5/1030.full.
- Received for publication December 30, 2020.
- Revision received February 20, 2021.
- Accepted for publication April 19, 2021.




{kind=link}