
Abstract
Introduction: Interventions are needed to promote utilization of the Medicare Annual Wellness Visit (AWV), an underused opportunity to perform screenings and plan individualized preventive health services.
Method: Using remote practice redesign and electronic health record (EHR) support, we implemented the Practice-Tailored AWV intervention in 2021 (during the COVID-19 pandemic) in 3 small community-based practices. The intervention combines EHR-based tools with practice redesign approaches and resources. Outcomes included completion of AWV and fulfillment of recommended preventive services.
Results: At baseline the 3 practices had 1,513 Medicare patients with at least 1 visit in the past 12 months. AWV utilization went from 7% at baseline to 54% 8 months postintervention implementation; advance care planning increased 10.7% (from 7.9% to 18.6%); depression screening increased 16.3% (from 51.7% to 68.0%); and alcohol misuse screening increased 17.3% (from 42.6% to 59.9%). Every individual preventive health service was received more often by patients with an AWV than those without. At the patient level, fulfillment of all eligible preventive services (of a maximum of 12 evaluated) went from 47.5% to 53.8% (P < .001). Subgroup analyses showed that patients with AWVs completed a greater percentage of their total recommended preventive health services than those without an AWV.
Conclusion: Virtual implementation of an intervention that combined EHR-based tools with practice redesign approaches increased AWV and preventive services utilization in Medicare patients. Given the success of this intervention during the COVID-19 pandemic (when practices had many competing demands), greater consideration should be given to delivering future interventions virtually.
Introduction
The Medicare Annual Wellness Visit (AWV) is an underutilized opportunity to increase patient use of evidence-based preventive health services. The AWV is a free-to-the-patient benefit that gives clinicians dedicated time to focus on evidence-based preventive care and perform health risk assessments. Despite its promise for increasing preventive health services, uptake of AWVs has been low, going from 7.8% of beneficiaries in 2011 to 24% in 2017.1⇓⇓⇓⇓⇓–7 This study, conducted in the midst of COVID-19, aimed to test the effect of a virtually implemented intervention on increasing AWV and preventive health services utilization.
Methods
The Practice-Tailored AWV intervention is a multi-component intervention addressing barriers to completion of AWVs and preventive health services. Tailored to each practice, delivered virtually, the intervention couples electronic health record (EHR)-based tools (to help identify patients who need AWVs) with practice redesign tools and approaches aimed to change practice culture and attitudes toward AWVs. EHR-based tools, coupled with practice redesign approaches and resources, help practices identify and contact patients in need of AWVs and ascertain the preventive health services needed by individual patients. Practice redesign approaches (delivered via a video-conferencing platform) included developing workflows for use of the EHR-based tools, supporting AWV-associated tasks, and improving clinician and staff efficiency. Resources included templates for the collection and documentation of required AWV components such as health risk assessments and patient personalized health plans. Table 1 describes the components of the intervention and options for tailoring in greater detail.
Major Intervention Tools and Approaches and Options for Tailoring*
We implemented the intervention in 3 community-based practices in Colorado that belong to a single organization. Each practice had 2 to 5 clinicians, of which at least 1 was a nurse practitioner. During a 3-month active implementation period (from April to June 2021) we met with a practice champion and other practice leads and worked with them to develop workflows to incorporate AWV-related procedures; trained staff on the use of EHR-based tools; socialized clinicians and staff on the importance of AWVs, required documentation and billing strategies; and met with selected clinicians and staff regarding their perceptions and experiences with AWVs. We tailored the intervention to the needs of the practices by scheduling training sessions to accommodate their requests (eg, including training for both clinicians and staff), adapting the length of the sessions to their needs, helping them select the resources they wished to use in their practice, and tailoring workflows to their practice.
We provided practices with feedback reports describing patient AWV and preventive health services utilization at the conclusion of the implementation and 3 months postimplementation. These reports were reviewed with clinicians and administrators during a clinician meeting immediately postimplementation, and with a practice champion and practice lead 3 months postimplementation, during which we discussed obstacles to AWV utilization and potential strategies for maintaining the momentum that the practices had achieved.
Outcomes
Outcomes were assessed through EHR data extractions. Outcome measures were: AWV completion in the past 12 months, receipt of preventive health services and screenings (being up-to-date at the time of assessment); and percentage fulfillment of all recommended preventive health services at the patient level (out of a maximum of 12 recommended: influenza, herpes zoster and pneumococcal vaccinations; screenings for colorectal, cervical and breast cancers; screenings for osteoporosis, hepatitis C, alcohol misuse, depression, tobacco use; and advance care planning). Prostate cancer screening was assessed primarily as evidence of overuse of a nonrecommended activity. Outcomes were assessed at baseline (4 months before intervention implementation) and 8 months postimplementation for patients aged 50 and older with Medicare insurance and at least 1 encounter in the past 12 months. We planned to assess outcomes 6 months postimplementation, but our data extractions included data up to 8 months postimplementation, so we present all available data.
Statistical Analyses
We calculated descriptive statistics to examine patient characteristics and preventive health service fulfillment on all patients and performed subgroup analyses to compare patients with and without an AWV using Chi-square and t tests (as appropriate for categorical and continuous variables). Repeated measures analyses were used to compare patient fulfillment of preventive health services at baseline and 8 months postintervention implementation, since some subjects are in both cohorts. Within subject correlations are likely high if a service is up to date for a long time after it is fulfilled, thus resulting in small standard errors when estimating changes. We also graphically depicted the percentage of AWVs completed per month among eligible patients across all 3 practice sites, and by individual site.
Results
At baseline the practices cared for 1,513 AWV-eligible patients, versus 1,167 8 months postintervention implementation. Table 2 depicts patient demographics at baseline and 8 months postimplementation. The baseline cohort was younger than the postimplementation cohort, but in both cohorts those who completed an AWV were older than those who did not have an AWV.
Characteristics of Patients Eligible for AWVs at Baseline and 8 Months Post-Intervention Implementation, Overall and by AWV Completion in the past 12 Months
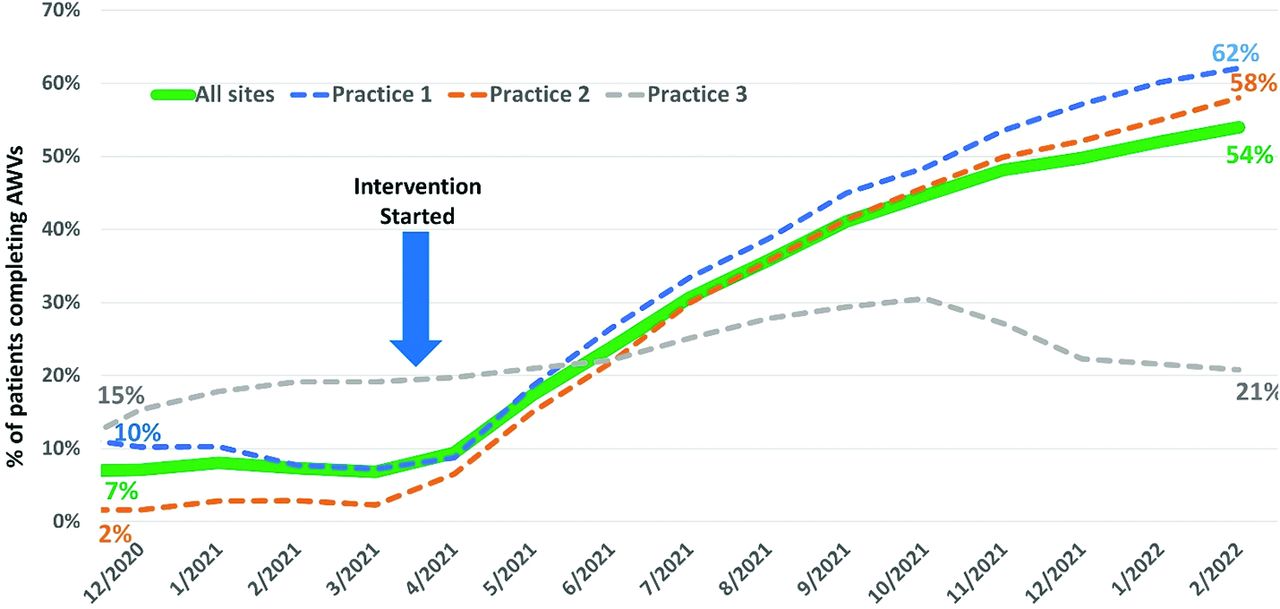
Overall, rates of AWV completion in the past 12 months increased from 7% at baseline to 54% 8 months postimplementation (Figure 1). The 2 larger practices each increased their rates of AWV completion by over 50%; the smallest practice doubled its rates (from 15% at baseline to 30% 4 months postimplementation) before dropping to a 6% increase from baseline at 8 months postimplementation. Table 3 compares fulfillment of different preventive health services at baseline and 8 months postimplementation. Utilization of the majority of preventive health services increased, with the exception of tetanus vaccination (not routinely covered by Medicare Part B), colorectal and prostate cancer screening, and tobacco use screening. Fulfillment of recommended preventive services on the patient level increased from 47.5% to 53.8% (P < .001).

Effect of practice-tailored medicare annual wellness visit (AWV) Intervention on rates of AWVs, overall and by practice site.
Preventive Health Services Completion Among Eligible Patients at Baseline and 8 Months Post-Intervention Implementation
Eight months postintervention implementation, patients who completed an AWV fulfilled all individual preventive health care metrics at higher rates than those without an AWV in the past 12 months (Table 4). On a patient level, those completing AWVs fulfilled more recommended preventive health services (of a maximum of 12 services) than those without an AWV, both at baseline (61.5% vs 46.4%, P < .001) and 8 months postimplementation (65.7% vs 39.7%, P < .001).
Preventive Health Services Completion Among Eligible Patients by Completion of Annual Wellness Visits (at Baseline and 8 Months Post-Intervention Implementation)
Discussion
A practice-tailored, virtually delivered intervention combining practice redesign and EHR tools and approaches increased AWV and preventive health service delivery in small community-based practices, with AWV use going from 7% at baseline to 54% 8 months postintervention implementation. The intervention improved AWV and preventive service use despite the impact of COVID-19 on practice demands during implementation. These increases may partially reflect improved documentation of AWV and preventive service completion. Better documentation often results in short-term improvements that wane over time, so it is encouraging to note that rates of AWV completion continued to increase throughout the measurement period. For the approximately 10% of patients in this study with Medicare Advantage insurance, providers may have replaced annual physical examinations with AWVs. Our intervention was likely effective because it met a demand – the practices and providers were already motivated to perform AWVs, but lacked tools to assess whether patients needed an AWV and to ensure fulfillment of all Medicare requirements for the AWVs.
Unexpected challenges arose during the study, largely resulting from the COVID-19 pandemic. The practices became COVID-19 vaccination sites, requiring attention to be diverted from performing AWVs. Surrounding communities were heavily affected by COVID-19, creating increased demand for acute care. The practices were further impacted when they began caring for COVID-19 patients without a regular primary care clinician. We addressed these issues by ensuring that all aspects of the intervention were tailored to the practices’ needs (eg, timing and duration of meetings with clinicians and staff), and developing workflows in which staff/scribes collected most of the information required for AWV documentation. An additional challenge uncovered by the study, but outside the scope of the intervention, was the mismatch between patients’ and clinicians’ expectations for comprehensive, integrated care, and the limited scope of the AWV.8
Before intervention implementation, these practices already received reminders regarding gaps in preventive service fulfillment at every patient visit. Yet after implementation, patient fulfillment of recommended preventive health services (of a maximum of 12) increased by a mean of 6.3%, or almost 1 additional preventive service per person. The greatest increases occurred for clinician-driven services (eg, advance care planning, depression screening, and alcohol misuse screening). These services incur no patient cost-sharing when performed in conjunction with an AWV, but clinicians rarely bill for them9 because they require specific documentation to satisfy billing requirements, as well as separate billing. These results suggest that the intervention’s focus on using the AWV as a means to deliver and bill for preventive health services can drive increased utilization of services. The COVID-19 pandemic may have attenuated the intervention’s effect, as patients may have been unwilling to make return visits for nonemergent screenings (eg, mammogram, colonoscopy). This is suggested by the decrease in preventive services received in patients not experiencing an AWV.
Patients who completed an AWV received more preventive health services than those without an AWV. Though our intervention did not specifically address the preventive service delivery process, patients in this study were more likely to complete each of the recommended services assessed. This is consistent with studies using Medicare claims data, which have demonstrated that AWVs increased the use of multiple different preventive services.10 Despite the USPSTF’s recommendation against PSA-based screening in men over the age of 70, prostate cancer screening in this population occurred more frequently when they had an AWV (Medicare covers annual PSA testing). This untoward effect warrants further study, and could be directly addressed during future efforts to promote AWVs.
Study limitations include possibly underestimating the intervention effect due to the short postintervention implementation follow-up, which may have limited our ability to capture patients who intended but had not yet completed preventive health services that required follow-up appointments or actions. The smallest site (practice 3), which had only 2 clinicians, experienced staffing issues during the assessment period that likely contributed to a smaller increase in AWV rates compared with the other sites. Generalizability is limited by implementation in 3 practices that belonged to the same organization. Most of the patients in the practices were white. We did not assess whether increased preventive service delivery was accompanied by increased billing for the services, but this warrants future exploration because practices’ ability to bill for screening and counseling services may drive increased utilization of these services. We also were unable to examine the quality or actual content of AWVs. Eight months postimplementation, the practices had several hundred fewer AWV-eligible patients than at baseline. Reasons for this could include patient attrition due to death or lack of patient visits in the past 12 months due to COVID-19.
The majority of the interventions described in the literature to promote AWVs focus on enlisting nonphysician health care providers (as opposed to primary care providers) to perform AWVs.11⇓⇓⇓⇓⇓⇓–18 These interventions may be difficult and costly for small and midsize practices with limited resources to implement. This study supports the use of an EHR-based intervention, coupled with virtually delivered practice-redesign approaches and tools, to enhance patient preventive health services utilization, and might serve as a model for virtual intervention implementation. Future studies are needed to rigorously evaluate the uptake and effectiveness of various intervention components.
This work is worthy of further evaluation in diverse practice settings. In the meantime, these findings support use of a practice-tailored remote redesign and electronic medical record support intervention to improve use of the Medicare Annual Wellness Visit and preventive service delivery and advance care planning.
Notes
This article was externally peer reviewed.
Funding: This study was supported by grant R61AG068946 from the National Institute on Aging.
Conflict of interest: Dr. Tarn has been funded by the BMS/Pfizer Alliance ARISTA-USA to conduct unrelated research studies.
To see this article online, please go to: http://jabfm.org/content/36/3/501.full.
- Received for publication September 28, 2022.
- Revision received January 3, 2023.
- Accepted for publication January 9, 2023.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.